
Abstract
Acute pulmonary thromboembolism occurring during cancer treatment has been increasing with the number of cancer patients and chemotherapy cases. Computed tomographic pulmonary angiography (CTPA) for evaluating the pulmonary artery is generally performed using rapid injection of contrast medium. However, intravenous catheters for contrast medium injection might cause extravasation due to rapid injection. This case series describes three patients who underwent contrast-enhanced computed tomography combined with low-tube-voltage imaging and slow injection. Low-tube-voltage slow-injection CTPA can be an effective technique for obtaining high contrast enhancement while accommodating fragile veins and low injection rates.
Keywords
Introduction
The recent increase in chemotherapy with molecular-targeted drugs has also promoted an increase in thromboembolism. The diagnosis of acute pulmonary thromboembolism (PTE) via computed tomography (CT) is versatile due to its high spatial resolution and simplicity. 1 The important roles of CT diagnosis include both determining the treatment efficacy in patients with carcinoma and diagnosing PTEs that need to be clinically ruled out.
Contrast-enhanced CT is effective in diagnosing subsegmental branches of the pulmonary artery and is the first choice for imaging. Generally, computed tomographic pulmonary angiography (CTPA) has been used to evaluate the pulmonary artery and is performed under rapid contrast medium injection. 2 However, certain conditions increase the difficulty of CTPA. Notably, intravenous catheters for contrast medium injection might cause extravasation due to rapid injection. To reduce the risk of extravasation, slow injection of contrast medium can be one solution; however, low fractional doses result in a decrease in the CT values of the pulmonary vessels.
We have some experience with contrast-enhanced CT combined with low-tube-voltage imaging and CTPA under slow injection without a decrease in CT values. We found that the contrast enhancement effect of low-tube-voltage imaging was comparable to that of conventional CTPA. In this case series, we detail our experience with three patients who underwent CTPA using low-tube-voltage CT under slow injection.
Case reports
Detailed case characteristics and data acquisition.
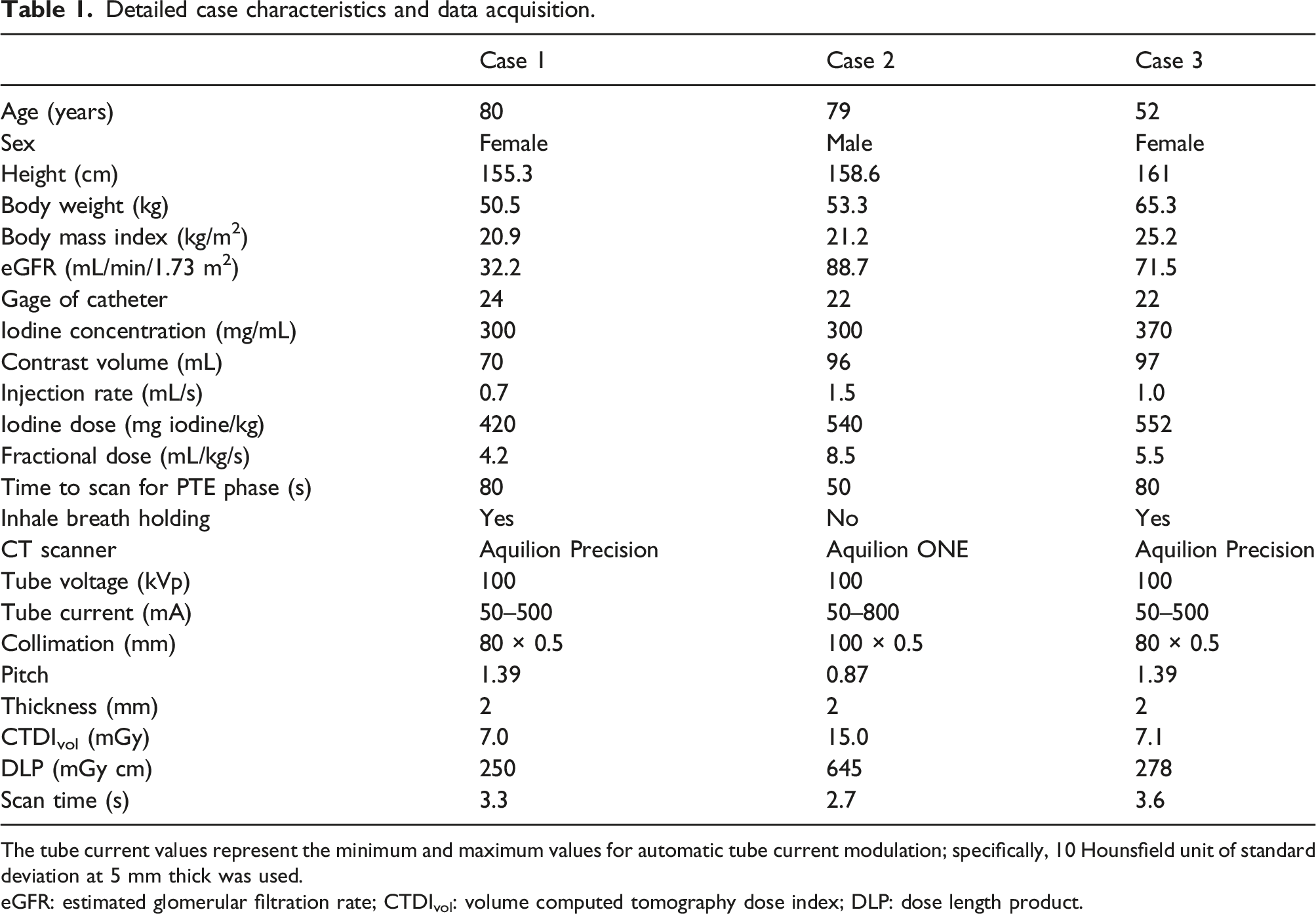
The tube current values represent the minimum and maximum values for automatic tube current modulation; specifically, 10 Hounsfield unit of standard deviation at 5 mm thick was used.
eGFR: estimated glomerular filtration rate; CTDIvol: volume computed tomography dose index; DLP: dose length product.
Contrast enhancement attenuation for each anatomical location.

Values represent CT values (Hounsfield unit). The attenuations were measured with a circular region of interest larger than 60 mm2 using Synapse Vincent software (Fujifilm Medical, Tokyo, Japan).
Case 1
Case 1 was an 80-year-old woman who had undergone surgery for uterine cancer and adenocarcinoma of the lung. Contrast-enhanced chest-to-pelvis CT was performed to evaluate for recurrence and rule out PTE.
A small peripheral catheter (24-gage) was inserted intravenously for a slow contrast medium infusion at 0.7 mL/s (70 mL of contrast agent containing 300 mg/mL of iodine). Scanning was commenced 80 s after the contrast medium was injected. The mean pulmonary artery attenuation was 274.9 Hounsfield units (HU). PTE was ruled out following CTPA examination. The iodine dose was reduced by approximately 25% due to reduced renal function. The use of a low tube voltage (100 kVp) was effective in maintaining contrast enhancement (Figures 1). An 80-year-old woman underwent chest-to-pelvic computed tomography (CT) for evaluating recurrence and ruling out a pulmonary artery thrombus. (a, b) Two different levels of axial images and (c) a coronal image. The iodine dose was reduced (420 mg iodine/kg) due to reduced renal function. CT values were 274.9, 232.9, 239.2, and 390.1 Hounsfield units (HU) at the pulmonary artery, left atrium, acceding aorta, and superior vena cava, respectively. Images were displayed with a window level and width of 60 and 300 HU, respectively.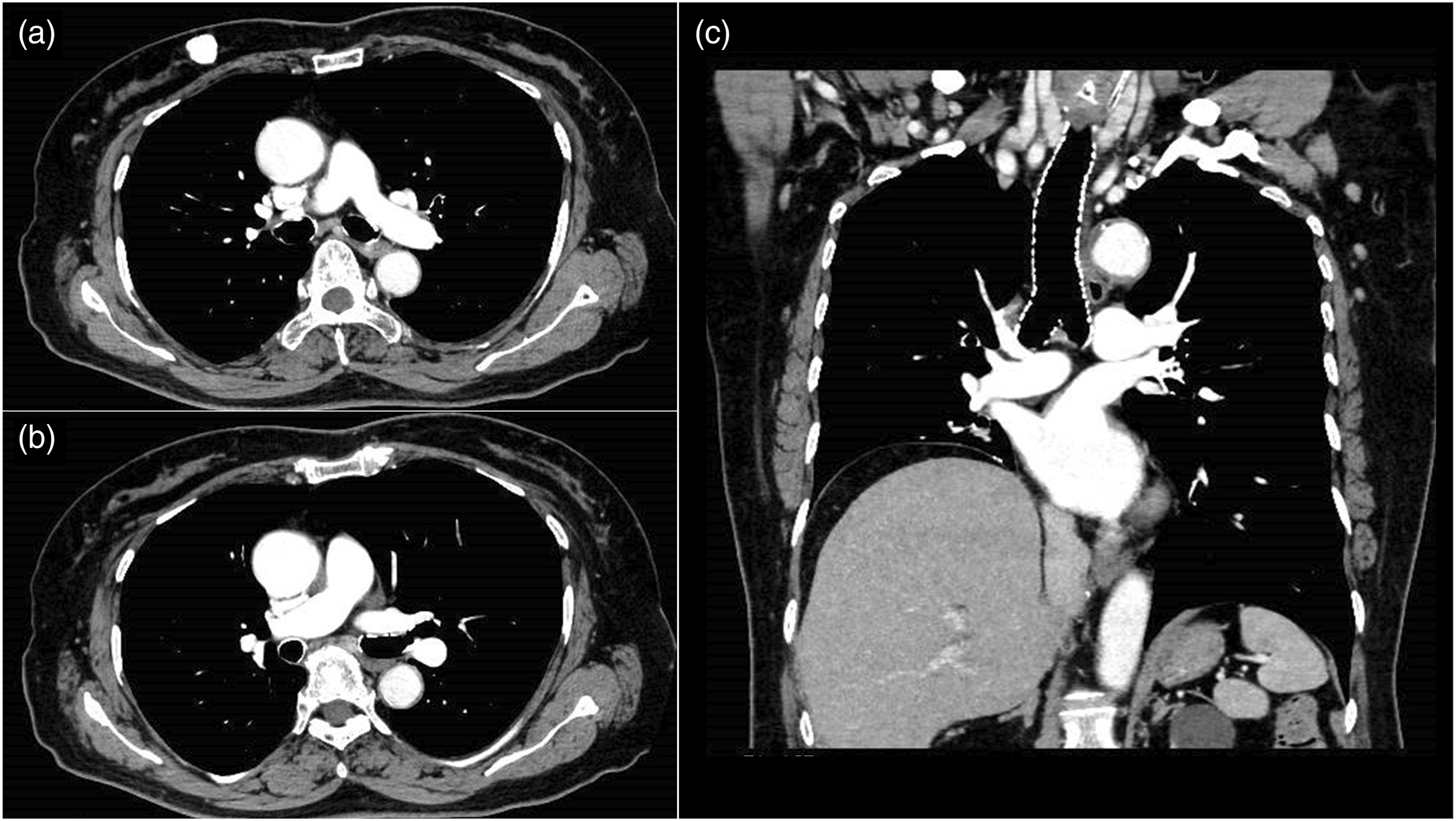
Case 2
Case 2 was a 79-year-old man who had undergone surgery for a right abscess that had developed as a complication after resection of the lower right lobe of the lung. This case developed acute respiratory distress syndrome with severe pneumonia (Figure 2). A 79-year-old man underwent surgery for a right abscess as a complication of resection of the lower right lobe of the lung. Same-level axial images reconstructed by (a) soft and (b) lung kernel. (c) A coronal image. Diffuse consolidation and ground-grass opacity can be observed in both lungs. CT values were 307.3, 279.8, 293.4, and 446.6 Hounsfield units (HU) at the pulmonary artery, left atrium, acceding aorta, and superior vena cava, respectively. Although the attenuation of SVC was the highest among the three cases, no evidence of streak artifacts was present. Images were displayed with a window level and width of 60 and 300 HU, respectively.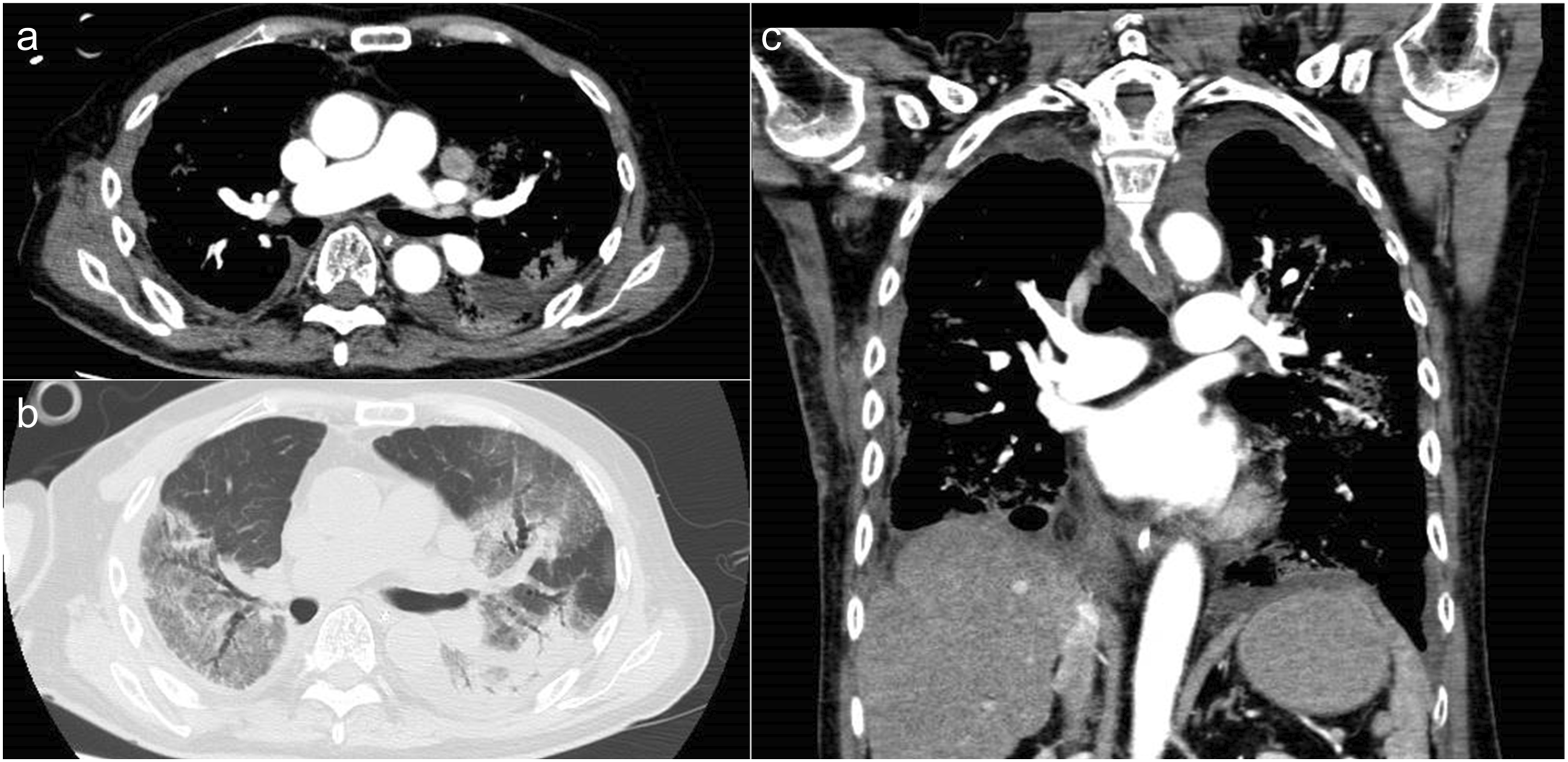
Contrast-enhanced chest-to-pelvis CT was performed to rule out a pulmonary thrombus and determine the source of his fever. Although a dynamic CTPA was attempted under ventilator management, the fragile veins made it difficult to secure a large-gage catheter. A 22-gage catheter was inserted intravenously, after which contrast medium was injected at a rate of 1.5 mL/s (96 mL of contrast agent containing 300 mg/mL of iodine). Scanning was commenced 50 s after the contrast medium was injected. Given that it was impossible to perform the scan under breath-hold, motion artifacts were reduced by high-speed acquisition. The mean CT value of the pulmonary artery was 307 HU, ruling out PTE.
Case 3
Case 3 involved a 52-year-old woman under chemotherapy after primary transverse colon cancer resection with hepatic and peritoneal metastases. Chest-to-pelvis contrast-enhanced CT was performed to determine the efficacy of chemotherapy and exclude PTE. A 22-gage catheter was inserted intravenously, after which contrast medium was injected at a rate of 1.0 mL/s (97 mL of contrast agent containing 370 mg/mL of iodine). Scanning was commenced 80 s after the contrast medium was injected.
Here, thrombi were diagnosed in both lower lobe pulmonary arteries as shown in Figure 3. Moreover, we found that CTPA with slow injection can depict thrombus in the subregional branches or those located more peripherally. A 52-year-old woman received chemotherapy after resection of primary transverse colon cancer with hepatic and peritoneal metastases. Two different levels of (a, b) axial images and (c, d) coronal images. A thrombus can be observed in the peripheral pulmonary artery of the left lower lobe (arrowhead). The mean CT value of the pulmonary artery was 290.8 Hounsfield units (HU), which was sufficient to identify a small thrombus. Images were displayed with a window level and width of 60 and 300 HU, respectively.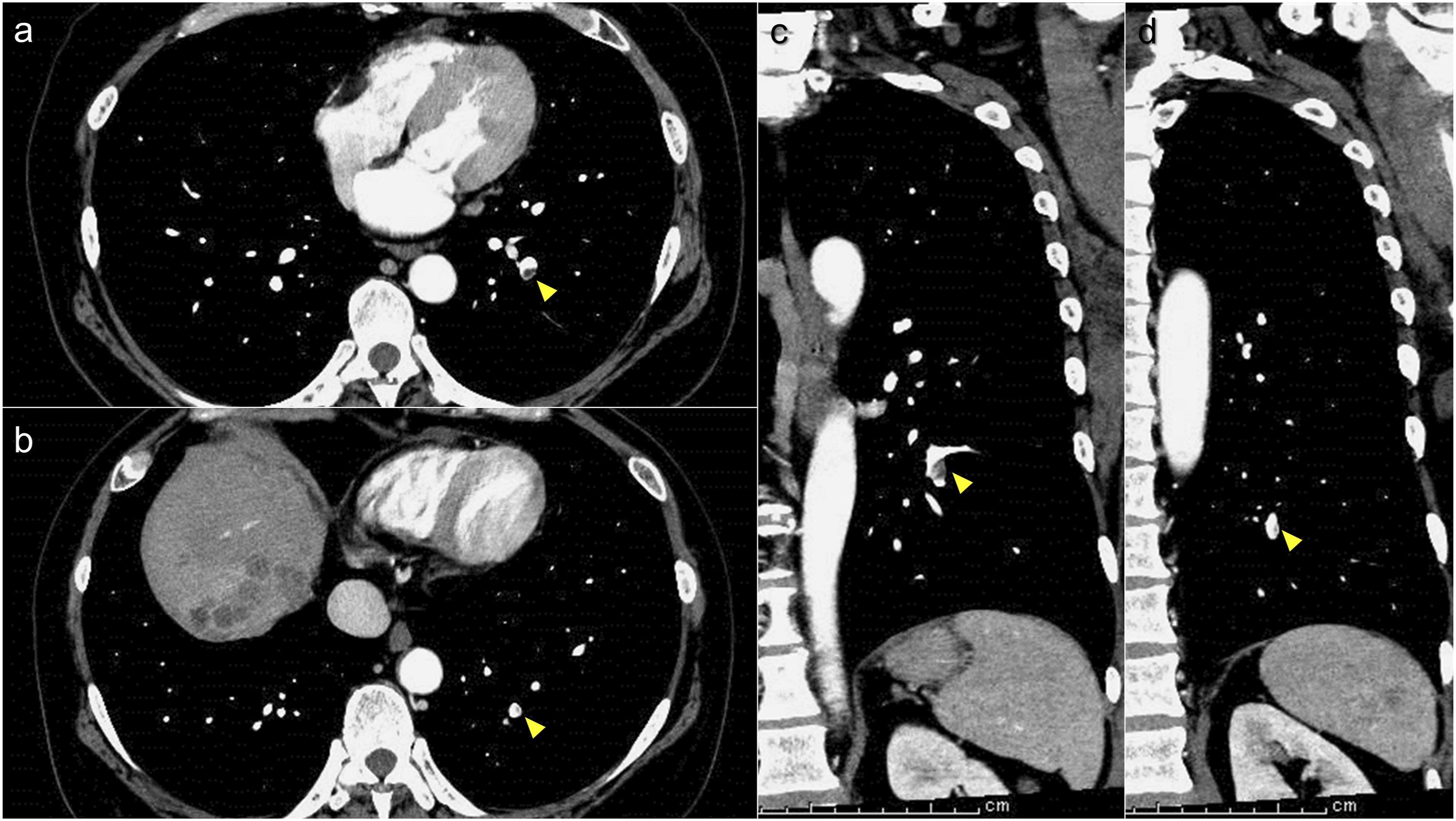
Discussion
This series compiles cases in whom diagnosis of PTE was underwent via CTPA under slow contrast medium injection. CTPA is the first-line imaging procedure for PTE diagnosis.3,4 Generally, CTPA requires rapid contrast medium injection at a rate of approximately 3.5–4.0 mL/s. 2 A large-gauge peripheral catheter must be placed intravenously to safely perform CTPA. Patients with carcinoma have an increased incidence of PTE 5 and often possess fragile veins in the upper extremities due to frequent chemotherapy or other treatments. Dynamic CT with catheters placed in fragile vessels often lead to extravasation. The slow-injection CTPA allows for contrast enhancement compared to that of conventional CTPA in cases wherein placing large-gage catheters prove difficult. The mean CT values of the pulmonary artery in all three cases ranged from 275 to 307 HU. Scanning was commenced when 75%–80% of the contrast volume had been injected. To maintain the contrast effect during CTPA at low fractional doses, a tube voltage of 100 kVp was used. One study showed that conventional CTPA performed under rapid injection was essential in single-helical CT given its insufficient ability to diagnose subsegmental thrombosis. 6 However, our proposed imaging protocol provides sufficient diagnostic performance with a high spatial and temporal resolution multi-detector-row CT.
The saline flush often performed in CTPA 7 could be omitted via slow injection. In the current cases, the maximum CT value of the SVC was 447 HU, with no strong beam hardening artifact having been observed (as shown in Case 2). The use of a significantly lower fractional dose compared to conventional CTPA allowed for a reduction in the extreme concentration increases and artifacts of the SVC. 8 The omission of the saline flush has the advantage of increased throughput during examination in addition to economic benefits.
An inspiratory transient attenuation artifact, which is rarely encountered in CTPA, can be characterized as a temporary decrease in contrast enhancement in the right heart system caused by inspiration.9,10 This artifact decreases the diagnostic performance of PTE. Exhalation CT is effective in preventing artifacts. However, in cases where respiratory control is impossible, such as in Case 2, or when the diagnosis of pneumonia is required, expiration reduces diagnostic performance. Slow-injection CTPA is performed after a long delay time. Given that the injected contrast agent is already circulating throughout the body and that contrast enhancement from the inferior vena cava has also been achieved, it is unlikely that an inspiratory transient attenuation artifact would occur even when imaging is performed under inspiration.
The slow-injection low-tube-voltage protocol proposed herein might cause dose starvation in obese patients due to a maximum tube current limitation. Advanced protocols using dual energy CT and/or deep learning–based reconstruction might solve these problems.11,12
In conclusion, low-tube-voltage slow-injection CTPA is a promising technique for achieving high contrast enhancement while accommodating fragile veins and low injection rates. Although our proposed method does not require a saline flush, artifacts produced by the SVC are minimal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent statement
This retrospective study was approved by the institutional review board (J2022-17). Given the retrospective, noninvasive nature of this study, the requirement for written informed consent from the patients was waived and information was instead made available on the institutional website.