
Abstract
Background
Estimation of the lateral hindfoot impingement in the standing position in conventional radiography can be difficult due to superimposition of different bones. Patients with flat feet frequently suffer from pain around the lateral malleolus and sinus tarsi caused by osseous impingement in the lateral hindfoot. Weightbearing multiplanar images (tomosynthesis) yield tomographic images and can be taken while full weightbearing.
Purpose
To assess the availability of tomosynthesis to determine hindfoot lateral impingement.
Material and Methods
A total of 14 feet (in 13 patients) with acquired flatfoot deformity and lateral hindfoot pain were included (mean age 64 years; age range 55–80 years). All patients underwent tomosynthesis, radiography, and computed tomography (CT) (non-weightbearing). Talofibular, calcaneofibular, and talocalcaneal impingement were determined. To compare the number of impingements or to determine the area between each image, statistical evaluations were analyzed using the Mann–Whitney U-test (P < 0.05).
Results
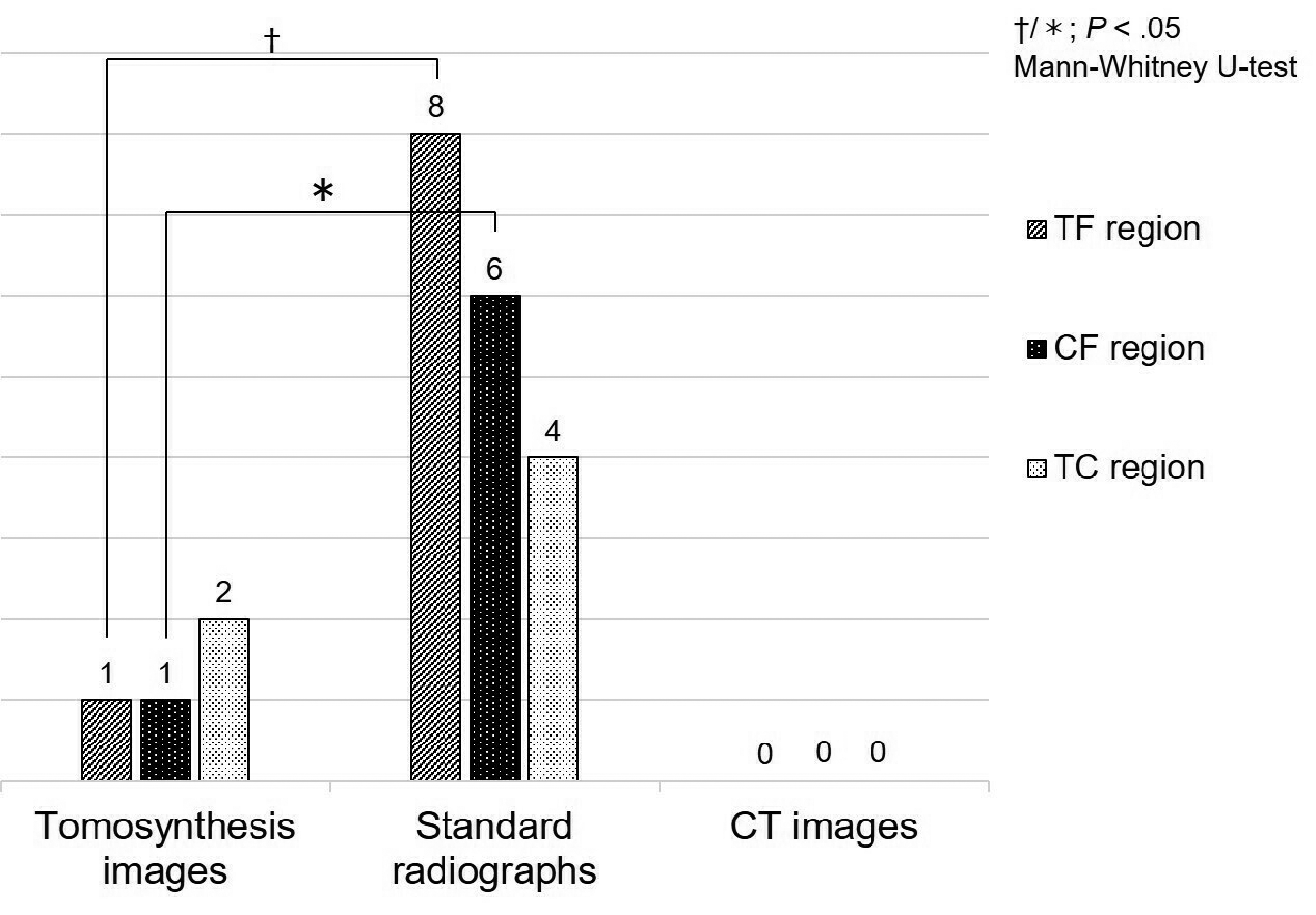
On tomosynthesis, we clearly found talofibular impingement in three feet, calcaneofibular impingement in seven feet, and talocalcaneal impingement in 11 feet. Therefore, we could identify most impingements as “positive” compared to those on normal radiographs and CT images. The number of impingements in the calcaneofibular and talocalcaneal regions was significantly higher using tomosynthesis than when using CT (P < 0.05).
Conclusion
Tomosynthesis imaging makes it easier to obtain CT-like images in a short period of time, in a free position, including while standing, and provides useful information to assess lateral pain in patients with flatfoot deformity.
Introduction
Patients with flatfoot deformity frequently suffer from lateral hindfoot pain, such as pain in the lateral malleolus and sinus tarsi. There have been previous reports of an association between these pains and osseous impingement in the lateral hindfoot caused by the existing deformity and frequent weightbearing (1–5). Estimation of the impingement in the standing position in conventional radiography can be difficult due to superimposition of different bones, particularly due to osseous impingements in the lateral hindfoot (Fig. 1). “Tomosynthesis” has been equipped with flat-panel detectors and enhanced utilities in recent years. It is called limited-angle computed tomography (CT) as it yields a clear tomographic image. Tomosynthesis has already been used for mammography or for images of the head and neck region, and the effectiveness in the orthopedic field has been widely recognized in recent years because tomographic images can be taken under mechanical stress, including the standing position (6–10).

Standard anteroposterior (a) and lateral (b) radiographs in a patient with flatfoot deformity. It is difficult to estimate the osseous impingement due to superimposition of the different bones.
We hypothesized that using tomosynthesis, more impingements were detected than using conventional radiography and CT in some patients with symptomatic flatfoot deformities. The aim of the present study was to search for an underlying cause of preoperative lateral hindfoot pain in patients with flatfoot deformity using the weightbearing multiplanar imaging (tomosynthesis images in the standing position).
Material and Methods
A total of 14 feet with acquired flatfoot deformity among patients (13 patients, two men and one woman) with specific complaints of lateral hindfoot pain from May 2012 to April 2014 were included. The average age of the patients was 64 years (age range = 55–80 years). All patients had stage II (or more) flatfoot deformities (3) that had failed conservative treatment and were scheduled for reconstruction surgery. Before the operation, all patients underwent tomosynthesis, radiography, and CT. All views from each imaging modality were used to determine the presence or absence of impingement in the talofibular (TF), calcaneofibular (CF), and talocalcaneal (TC) regions. The local ethics committee approved the study and written consent was obtained from all patients.
The tomosynthesis examinations were performed using SONIALVISION safire II (Shimadzu Co., Kyoto, Japan) equipped with a digital tomography system. Each patient stood on a wooden platform, fully weightbearing on both feet, and images in the sagittal and coronal planes were obtained in front and lateral views with reference to the plane passing through the axis of the second metatarsal bone (Fig. 2).

Clinical photograph of a patient demonstrating the posture and position of the feet during sagittal image acquisition using the SONIALVISION safire II. Patients were provided with table hand holds for stability and a secure Velcro strap for safety.
A digital radiographic examination included standard two-dimensional anteroposterior and lateral views in the standing position obtained separately for each patient. For the CT examinations, the patient was positioned supine, with the ankles in slight extension, the heels resting on the table, and the feet resting on a cushion. Multiplanar reconstruction images in all required planes were manually created by the authors during image evaluation. All views from the tomosynthesis images, standard radiographs, and CT were used to determine the presence or absence of impingement in the TF, CF, and TC regions. The criteria to determine the impingement status on each image are shown in Fig. 3. To compare the number of impingements or to determine the area between each image, statistical evaluations were analyzed using the Mann–Whitney U-test. Significance was set at P < 0.05 in accordance with literature standards.

Criteria for determining impingement. First, the ambiguity due to superimposition of the different bones was regarded as “impossible” at each location. Subsequently, when the area was determined to have clarity, a “positive” or “negative” result was given according to the presence of an osseous impingement. However, some cases that did not have an osseous impingement but had osteoarthritic changes such as a bone cyst or sclerosis were classified as “suspected,” because the osteoarthritic change may be the result of an impingement during walking or running.
Results
“Positive” impingements, on the tomosynthesis images, were found in the TF region in three patients, in the CF region in seven patients, and in the TC region in 11 patients (Fig. 4). Using conventional ankle radiographs, impingements were found in the TF region in two patients, in the CF region in six patients, and in the TC region in seven patients. Using CT images, impingements were found in the TF region in three patients, in the CF region in two patients, and in the TC region in four patients, respectively. The number of impingements in the CF region was significantly higher using tomosynthesis than when using CT (P < 0.05). Likewise, the number of impingements in the TC region was significantly higher using tomosynthesis than when using CT (P < 0.05). On the tomosynthesis images, more impingements were detected as “positive” compared to those on normal radiographs and CT images (Figs. 5 and 6). “Suspected” results were evaluated based on osteoarthritic changes without direct osseous impingement and occurred most frequently on non-weightbearing CT images compared to the others (Fig. 7). Compared with tomosynthesis, the number of “suspected” results (Fig. 8) was significantly higher in the TF, CF, and TC regions on CT images (P < 0.05). “Impossible” results were mostly observed on normal radiographs, especially in the TF region, where more than half of the cases could not be determined. In addition, we classified “impossible” six times in the CF region and four times in the TC region on normal radiographs. On the other hand, we determined the area with clarity in most cases; “impossible” cases were in a minority on tomosynthesis image. The number of “impossible” cases when using tomosynthesis was significantly lower than that on the radiographs in the TF and CF regions, respectively (P < 0.05). On CT images, there were no “impossible” cases (Fig. 9).

The talofibular (a), calcaneofibular (b), and talocalcaneal (c) impingements on each tomosynthesis image.

Comparison of standard radiographs (a, c) and tomosynthesis images (b, d) in a patient with lateral hindfoot pain. The talofibular and talocalcaneal impingement are more readily apparent on the each tomosynthesis image (arrowhead).

Comparison of the “positive” impingement on each image.

Coronal (a) and sagittal (b) computed tomography images of the same patient as in Fig. 5. We can clearly observe the talofibular and talocalcaneal regions. However, there was no osseous impingement directly on each part because of non-weightbearing.

Comparison of the “suspected” impingement on each image.
Comparison of the regions deemed “impossible” on each image.
Discussion
Several reports used simulated weightbearing CT scans to visualize osseous impingement in patients with flatfoot deformity (2,4). Malicky et al. (4) obtained CT scans of 19 patients with symptomatic flatfeet, simulating weightbearing by applying a 75-N load to the supine subject. They reported that the overall prevalence of impingement within the sinus tarsi was 92%, and the prevalence of impingement in the CF region was 66%. In the present study, TC impingement was 79% and 29%, and CF impingement was 50% and 14% on tomosynthesis and CT images, respectively. On CT images, osseous overlapping is prevented; the impingement can be determined using multiplanar reconstruction. However, little is known about the impingement in light of reproducibility because load testing devices vary according to the studies. In the present study, there were no “impossible” cases and many “suspected” cases were identified through CT images. In other words, osteoarthritic changes were clearly confirmed without direct osseous impingement on CT images. From the presence of osteoarthritic changes, we inferred that some osseous impingements were not determined directly because of a non-weightbearing status. Therefore, in clinical practice, early stage impingements without osteoarthritic changes such as bone cysts or sclerosis may be missed on conventional CT imaging. On the other hand, the degenerative changes do not necessarily correspond to the osseous impingement or therewith pain.
Ellis et al. (1) reported on the reliability of weightbearing multiplanar images similarly to tomosynthesis. Ten flatfoot patients with lateral hindfoot pain were compared to 10 patients with deformity but no pain and underwent conventional radiography and weightbearing multiplanar imaging using the Philips medical systems Multi Diagnostic Eleva scanner. As a result, subtalar arthrosis, CF impingement, and calcaneocuboid arthritis were found to be increased in the pain group. In the present study, most impingements were detected via tomosynthesis compared to radiographs and CT images in all locations.
Providing three-dimensional information at lower doses for a shorter time period, having a higher ability of spatial analysis, reducing some metallic artifact (Fig. 10), and a potentially lowered cost compared to CT in certain clinical imaging situations are all advantages of using tomosynthesis (6–10). Especially regarding the radiation dose of tomosynthesis, it is reported that the average adult chest examination produces 2.3 times the radiation of a typical two-view chest radiographic examination and < 2% of that for the average thoracic CT examination; whereas the effective dose for tomosynthesis has been determined to be 0.124 mSv (8). For these reasons, the tomosynthesis images were widely used not only for diagnostic imaging of the foot and ankle, but also for the follow-up of postoperative or traumatic cases, without a reservation at our facility. The disadvantages of tomosynthesis images are that it is necessary to change positions accordingly to obtain arbitrary sectional images because image reconstruction processing is limited to a plane parallel to a detector plane, and the images are often blurred because the information contained in slice thickness (usually around 5.0 mm) overlap with an arbitrary image. Therefore, these factors may have caused some cases of “impossible” results in the present study.

The postoperative coronal (a) and sagittal (b) tomosynthesis image of the same patient as in Fig. 5. The hindfoot alignment in the standing position improved and each osseous impingement was corrected with surgery (arrowhead).
The present study is primarily limited by the fact that only one observer was involved. For this reason, there was no interrater reliability assessment. A second limitation of the study is that only patients with severe deformity who were scheduled for reconstruction were surveyed. The final limitation of the study is the small number of patients.
In conclusion, the multiplanar imaging (tomosynthesis) assessed in the present study provides tomographic images easily in a fully upright and weightbearing position, and useful information to assess lateral pain in patients with flatfoot deformity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.