
Abstract
Keywords
Introduction
Recall and cancer detection rates improve with digital breast tomosynthesis (DBT) because it resolves summation artifacts and highlights subtle mammographic lesions.
1
These benefits have increased demand for tomosynthesis-guided biopsy (TB), which is performed with either a prone table or an upright DBT unit. With either system, the needle can approach the target in two directions: the vertical needle approach (VNA, needle perpendicular to compression plate) and the lateral-arm needle approach (LANA, needle parallel to compression plate) (Figure 1). Advantages of LANA include high safety and efficacy, a fast learning curve, quicker procedure times, and the ability to sample lesions within breasts that compress as thinly as 1.0 cm.2-6 The primary disadvantage is difficulty anesthetizing deep lesions.
3
Our study aimed to compare technical details and outcomes for LANA and VNA. We hypothesized that LANA would have longer procedure times due to radiologist inexperience, use fewer exposures, and target more non-calcified lesions than VNA. (A) Photograph showing the lateral-arm needle approach for prone tomosynthesis-guided breast biopsy with the 9-gauge biopsy needle (Eviva, Hologic). (B), Post-fire craniocaudal tomosynthesis view during prone tomosynthesis-guided biopsy with the lateral-arm needle approach documents the needle trough within the centre of the targeted architectural distortion, thus affording a high degree of confidence in tissue sampling. Biopsy yielded a complex sclerosing lesion with atypical ductal hyperplasia, and subsequent excisional biopsy diagnosed high-grade ductal carcinoma in situ.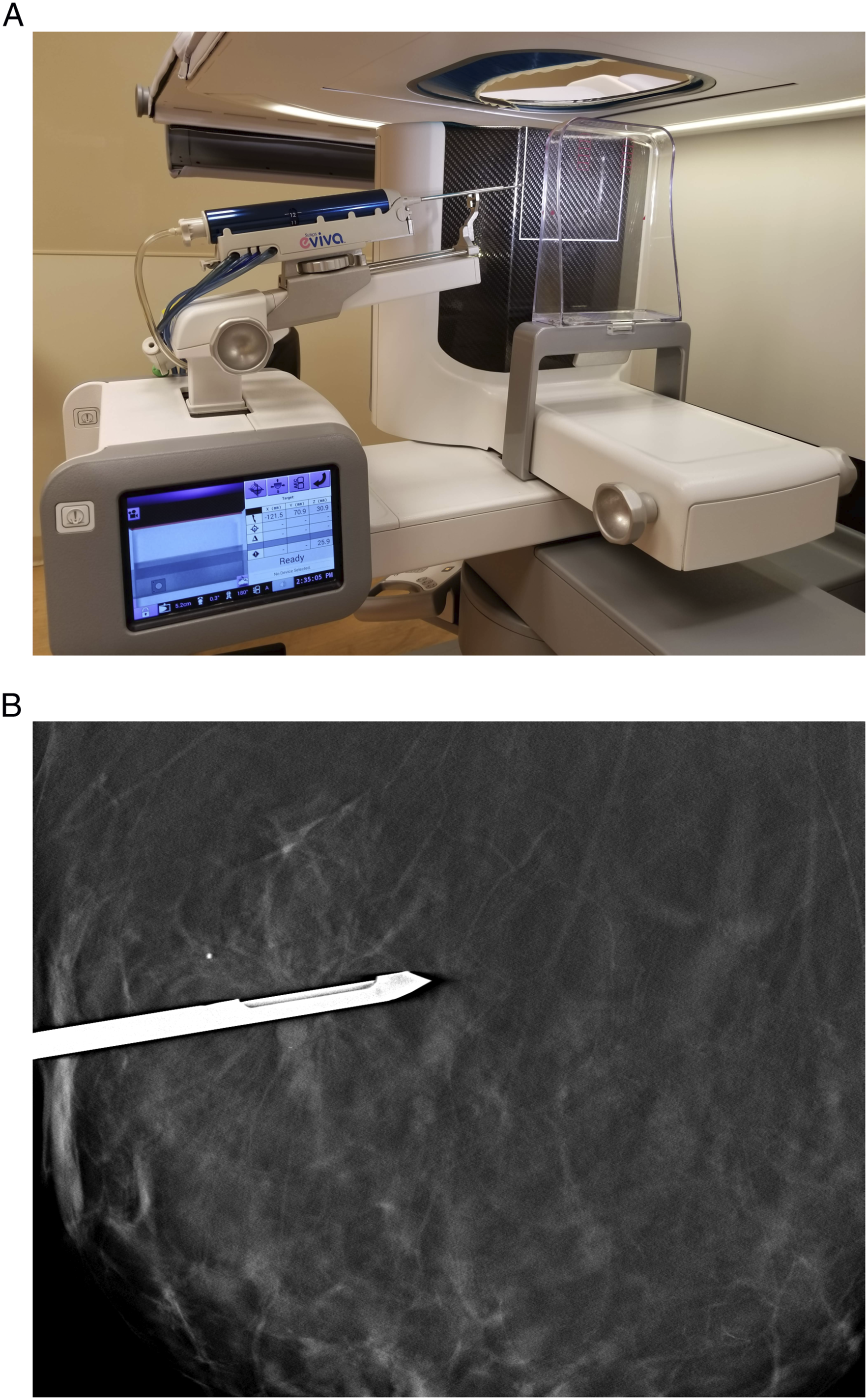
Methods
The institutional review board approved this HIPAA-compliant, retrospective study. Informed consent was waived. We reviewed 324 consecutive prone TB on 304 patients performed at one community-based breast centre during 21/04/2016–31/12/2019 by one of ten academic, fellowship-trained radiologists (1–10 years of experience). LANA was unavailable prior to the study period. LANA or VNA was selected based on radiologist preference, which was most often determined by lesion type (calcification, distortion, asymmetry, or mass), lesion location, and breast compression thickness. Biopsy methods have been previously described5. All patients in that study who underwent biopsy with LANA overlapped with this study’s population. Biopsy image timestamps were used to calculate total procedure time (time between first scout and last biopsy clip images), lesion targeting time (time between first scout and first pre-fire images), and tissue sampling time (time between first pre-fire and last biopsy clip images). Statistical analysis included Two sample t-test and Fisher’s exact test. P-values<.05 indicate statistical significance.
Results
Procedure Details and Outcomes for Biopsies Performed with the Lateral-Arm and Vertical Needle Approaches.
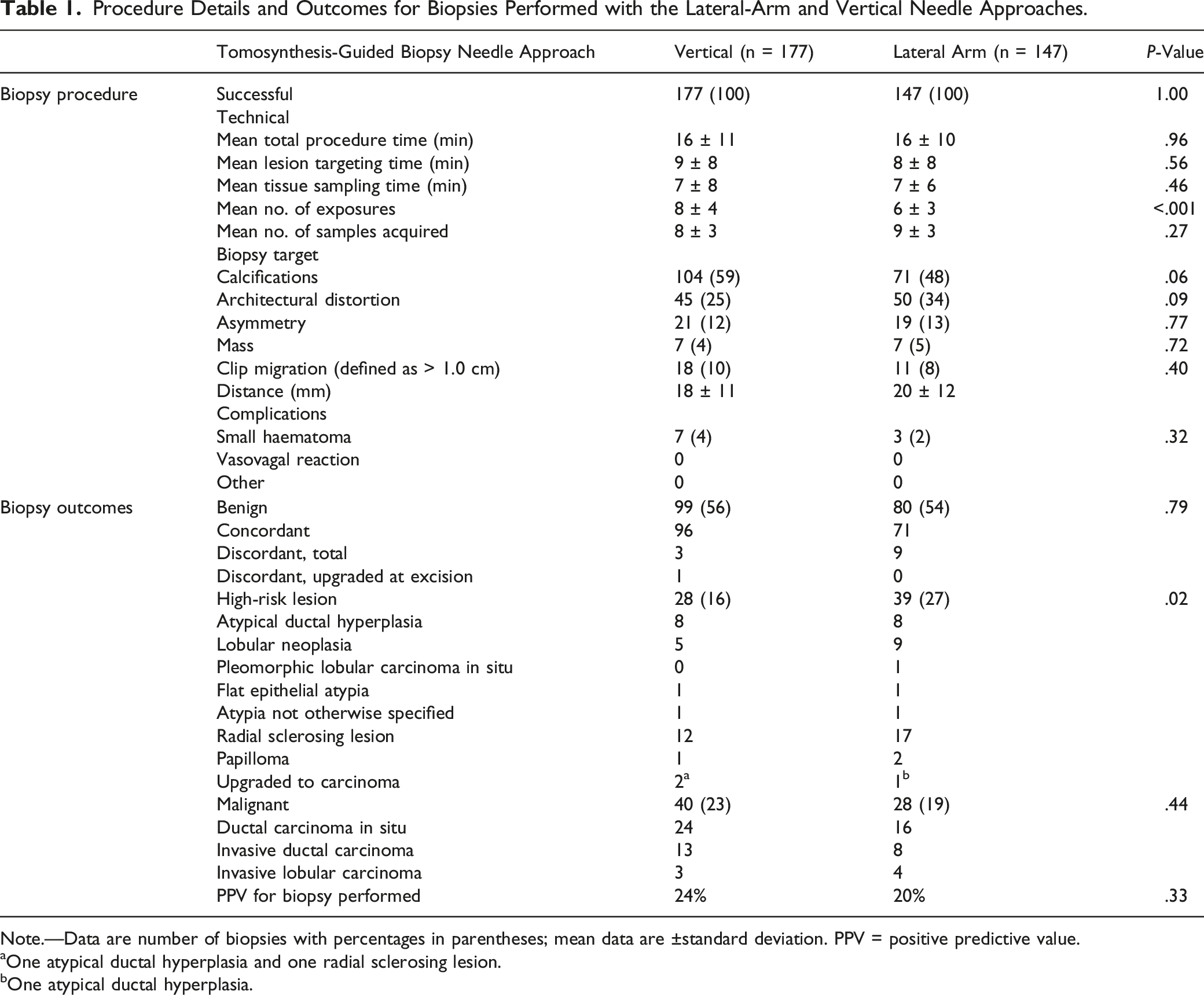
Note.—Data are number of biopsies with percentages in parentheses; mean data are ±standard deviation. PPV = positive predictive value.
aOne atypical ductal hyperplasia and one radial sclerosing lesion.
bOne atypical ductal hyperplasia.
Discussion
Our review of 324 consecutive prone TB found 100% success for both needle approaches. More calcifications were targeted with VNA, while fewer exposures were used, more architectural distortions were targeted, and more high-risk lesions were diagnosed with LANA. Interestingly, the needle approach did not affect total procedure time as we had hypothesized, despite radiologist inexperience with LANA (both 16 minutes, P = .96). This indirectly suggests a fast learning curve for LANA. Also, because LANA vs VNA was nonrandomly selected by the radiologist, we believe our findings indicate radiologist preference for LANA with non-calcified targets, which do not appear within specimen radiographs. Intuitively, LANA should afford greater confidence in sampling because the needle is perpendicular to the tomosynthesis beam, rather than parallel, allowing for confident visualization of the biopsy target at the needle trough (Figure 1).
Our findings compare similarly to prior studies that indicate LANA is safe and effective for normal and thinly compressed breast tissue.2-6 We found no major complications, and the thinnest breast in our study compressed to 1.3 cm (compared with 2.9 cm for VNA). Weaver et al 5 observed no significant difference between LANA and VNA for bleeding or clip migration, again consistent with our findings. Kerger et al 2 reported faster procedures and increased patient throughput with LANA, though we noted identical total procedure times for LANA and VNA (both 16 minutes, P = .96).
Study limitations include reduced generalizability given the retrospective study design with academic, fellowship-trained radiologists performing biopsies at one community-based breast centre. Moreover, the needle approach used for each procedure was nonrandom and potentially introduced bias. However, we believe our study accurately reflects community radiology practice. In conclusion, the LANA and VNA for prone TB are safe and effective. The main advantage of LANA is fewer exposures and its ability to sample lesions in very thinly compressed breasts.
Footnotes
Acknowledgements
The authors thank Scientific Publications, Research Medical Library at The University of Texas MD Anderson Cancer Centre and the staff of Memorial Hermann Texas Medical for their assistance with this article. We would also like to acknowledge support by the NIH/NCI under award number P30 CA016672.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Disclosures
Cohen, Weaver, Korhonen, and Sun: None.
Leung: (not relevant to this work): Scientific advisor to Subtle Medical and speaker for Fujifilm and GE Healthcare.