
Abstract
A 52-year-old patient referred to our hospital for a screening mammogram showed a suspicious new architectural distortion. Previously, a fibroadenolipoma within the right breast was diagnosed clinically and radiologically. Further work-up with tomosynthesis, magnetic resonance imaging, and magnetic resonance-guided biopsy showed an invasive ductal carcinoma within the fibroadenolipoma, which are usually benign breast lesions not associated with malignancy. This case report offers a review of the literature and a discussion of signs, which should alert the radiologist.
Case report
A 52-year-old patient with no personal history of breast cancer or previous breast interventions was referred to our hospital for screening mammogram. One younger sister had been diagnosed with breast cancer at the age of 45 years. This was the patient’s second round of screening with the previous mammogram having been performed two years prior, in which a well circumscribed mass had already been clinically, mammographically, and on ultrasound described in her right breast with diffuse microcalcifications. She had had this lump for years; in addition, the referring gynecologist reported it as stable and palpable for years. This was determined to be a probable fibroadenolipoma (also called hamartoma or breast-in-breast) (Fig. 1). Furthermore, she had a heterogeneously dense breast corresponding to the ACR-BI-RADS Atlas category c. Since 2017, women presenting at our institution with heterogeneous or extremely dense breasts receive a full digital craniocaudal (CC) view and tomosynthesis in the mediolateral oblique (MLO) view with a reconstructed synthetic MLO mammogram to reduce the overlapping effect in the dense breast. In the tomosynthesis for the patient in this report, the well circumscribed mass in the right breast could be delineated (Fig. 2a); within its mediocaudal border, a spiculated area could also be identified (Fig. 2b). It was classified as BI-RADS 5. The lesion could not be seen on ultrasound, so the patient received magnetic resonance imaging (MRI) of the breast to confirm the lesion and identify further differentiation.

A 52-year-old woman presented for a bilateral screening mammogram. (a–d) Bilateral mammogram from 2016: (a) right breast –craniocaudal (CC) view; (b) left breast – CC view; (c) right breast – mediolateral oblique (MLO) view; (d) left breast – MLO view. (e–h) Bilateral mammogram from 2018: (e) right breast – CC view; (f) left breast – CC view; (g) right breast synthetic – MLO view; (h) left breast synthetic – MLO view. Especially in the right MLO view (c, g), a partially well circumscribed 8.7 × 4.7 cm mass is seen and indicated by white arrows.

(a) Slice of the tomosynthesis of the right breast, where a well circumscribed mass occupying almost the whole upper quadrant is seen. (b) Another slice of the tomosynthesis 23 mm medial from (a). The yellow arrows indicate an anomolous architectural distortion with spicular borders at the mediocaudal boarder of the well circumscribed mass.
The MRI confirmed a solid mass in the right breast (Fig. 3a and 3b), measuring 7.7 × 4.5 cm, and was hyperintense compared with the surrounding tissue on T2-weighted (T2W) images. Within the lesion, the small milk ducts showed protein-rich liquid and cysts. Furthermore, at the mediocaudal border of the mass, a hypointense lesion was detected on T2W images with a strong and early enhancement on the dynamic T1-weighted (T1W) images that correlated to the lesion detected by tomosynthesis. It was classified on the MRI report as BI-RADS 5.
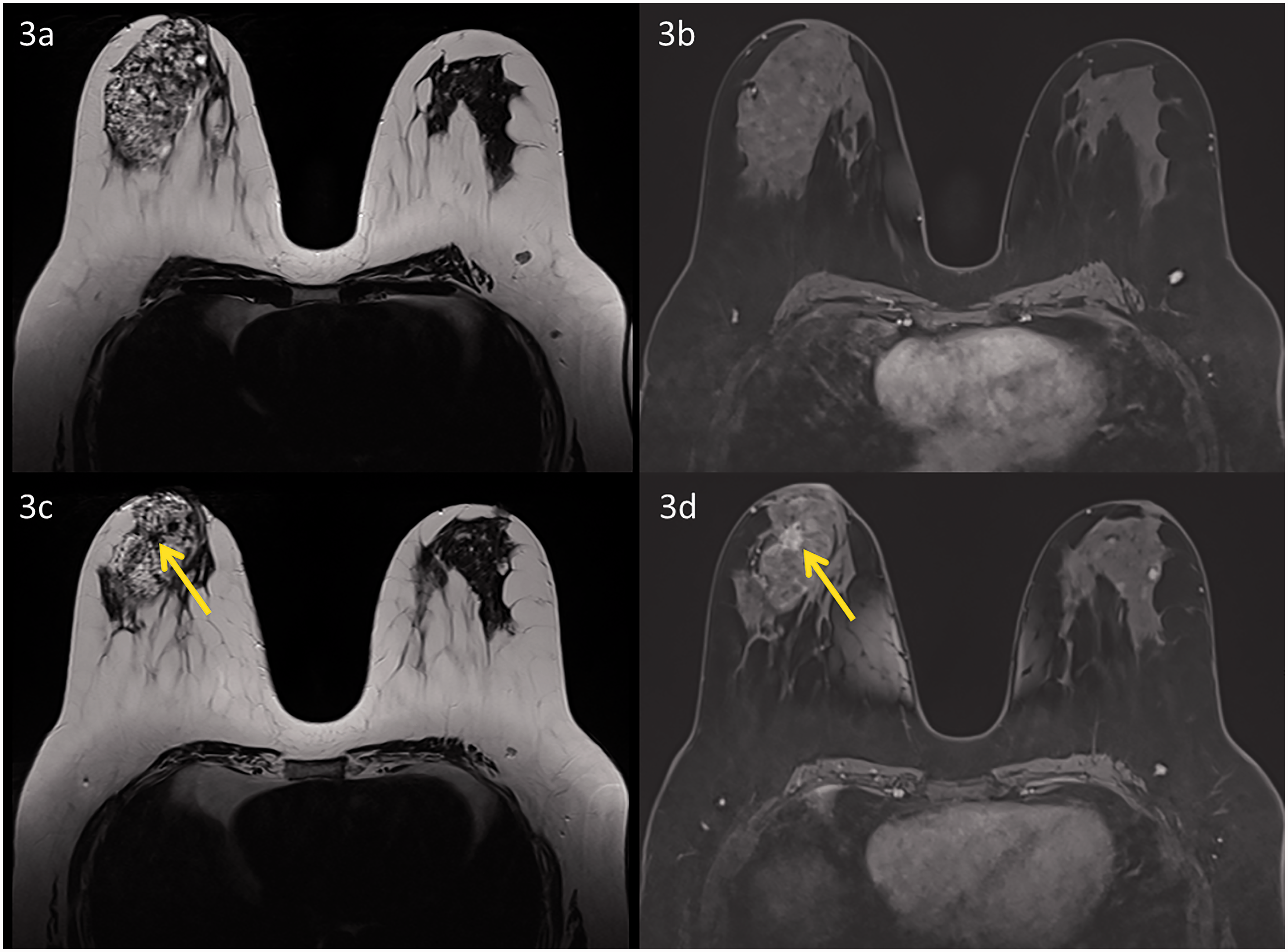
MRI of the breasts undertaken to investigate the lesion detected on tomosynthesis (Fig. 2b) in a 52-year-old woman. On the right breast, a well circumscribed mass can be delineated on T2W (a) and on T1W fat-suppressed images (b). In the T2W image, the mass is especially bright compared with normal glandular tissue and in native T1W shows fat-suppressed images and some protein-rich content. Additionally, a small pseudocapsule can be distinguished in the T2W image. In correlation to the tomosynthesis images (Fig. 2b), a dark lesion on T2W can be detected with some distortion of the surrounding tissue, shown by the yellow arrow (c). After administration of gadolinium this lesion was enhanced significantly compared with the surrounding tissue (yellow arrow) (d).
Because our mammographic system does not allow tomosynthesis-guided biopsies, the patient underwent MRI-guided biopsy (Fig. 4c and 4d). Histopathology revealed an invasive ductal breast cancer with expression of estrogen receptors (ER) (95%), progesterone receptors (100%), androgen receptors (100%), Her-2 (negative), and Ki67 (5%).

Lesion with the first dynamic contrast series (a, b), marked with yellow arrows. (a) Axial view, (b) reconstructed sagittal view. The lesion is approximatively 23 mm from the nipple and is located at the mediocaudal boarder of the abovementioned mass. Because the lesion could not be seen on ultrasound, the patient underwent an MRI-guided biopsy. (c) T1W images without fat suppression after administration of gadolinium. The yellow arrow shows the lesion with a marked enhancement. (d) Control T1W image after placing the needle within the lesion.
To ensure that the main/bigger mass was indeed a fibroadenolipoma and not a non-enhancing low-grade carcinoma, another ultrasound-guided biopsy at the upper edge of the mass was performed (Fig. 5c and 5d) with the histopathological results corresponding to the imaging finding of normal breast tissue.

(a) T1W image of the fibroadenolipoma, which is well defined as highlighted by the arrowheads. The corresponding ultrasound images (b) also show a well-defined mass (highlighted by the arrowheads) with hyperechogenic breast parenchyma and some accentuated milk ducts. The upper part of the fibroadenolipoma was biopsied under ultrasound control to confirm the diagnosis and exclude low-grade carcinoma. (d) Pre-fire image (biopsy needle in front of the mass, yellow arrow). (d) Post-fire image with the needle inside the mass, indicated by the yellow arrow.
The patient underwent a breast-conserving operation with sentinel lymphonodectomy. The final histopathology demonstrated a 13-mm invasive ductal carcinoma with a peritumoral carcinoma in situ (DCIS, G1), pT1c, pN0 (0/4), G1, L0, V0, Pn0.
Discussion
Fibroadenolipomas are uncommon benign masses of the breast. The entity was first described by Arrigoni et al. in 1971 (1). They usually occur as painless masses, resulting from a benign proliferation of fibrous, glandular, and fatty tissue surrounded by a thin capsule of connective tissue. Because of the varied composition of the mass, some authors also termed the entity lipofibroadenoma or adenolipoma, dependent on the predominant components of the breast tissue. The reported incidence of breast hamartomas is 0.7% of benign breast tumors in women (2). Diagnosis is often made mammographically, where the tumors have a characteristic appearance consisting of a circumscribed mass of mixed fatty and soft-tissue elements with a thin pseudocapsule (3). Digital breast tomosynthesis offers a cross-section in plane acquisition, which adds more details, reduces summation of overlapping tissue, and depicts the margins of masses at far greater detail than mammography. Thus, a hamartoma imaged with tomosynthesis characteristically appears as a round or oval mass with a thin water-density capsule delineating a border of fat. The central portion of the mass generally contains mixed fibrofatty elements with radiolucencies (4). On ultrasound, hamartomas resemble normal breast tissue, which results in the margins being difficult to delineate. The internal echo-texture of most hamartomas is either hyperechoic or composed of mixed echogenicity. Retrotumoral acoustic phenomena usually are absent (5). On MRI, a hamartoma appears as an encapsulated fatty mass with a fibroglandular signal and having the same value of apparent diffusion coefficient (ADC) as normal glandular tissue. In addition, the enhancement pattern is comparable to normal breast tissue (6).
The incidence of malignant lesions associated with hamartomas is rare. In 2012, Kai et al. described 12 case reports in the literature (7), most of them invasive ductal carcinomas as in our case. Currently, there are no significant data on the incidence of carcinomas within hamartomas and consequently patients with hamartomas are not considered to have a higher risk for developing carcinoma. In the study by Kai et al., the carcinomas were mostly detected as architectural distortions on mammography. This case report is the first showing a breast cancer within a hamartoma detected by tomosynthesis, a technique that is developing an increasing role in the daily work of radiologists.
In conclusion, although an invasive carcinoma arising within a benign fibroadenolipoma is a rare entity, the radiologist should be aware of the possibility and thoroughly investigate any architectural distortion or stellate lesion within an otherwise typical fibroadenolipoma.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.