
Abstract
Hemangioma of the rib is a rare benign tumor that is often difficult to distinguish from malignant bone tumors. Rib hemangioma often shows bony disruption with a slight cortical disruption, extraosseous lesion, and expanded bone on computed tomography (CT). We report the case of a 68-year-old man with atypical rib hemangioma with a slight cortical disruption and no expanded bone. The tumor showed relatively high 18FDG-uptake on positron emission tomography (PET)/CT. Rib hemangioma often shows higher 18FDG-uptake. PET/CT may not provide useful information for distinguishing rib hemangioma from a malignant tumor. Close observation without surgical resection may be feasible if the tumor is diagnosed as a rib hemangioma by biopsy.
Keywords
Introduction
Bone hemangiomas are benign hamartomatous vascular tumors. They account for less than 1% of all bone tumors (1). Approximately 50–80% of bone hemangiomas occur in the vertebral body or the skull (2). Hemangiomas of the rib are relatively rare; hence, they are often misdiagnosed as malignant tumors, such as metastatic tumors or primary malignant bone tumors. Given that 60–80% of the primary rib tumors are malignant (1), it is important to have knowledge of the features of rib hemangioma images.
We experienced a case with hemangioma of a rib showing relatively high 2-fluoro [fluorine-18]-2-deoxy-D-glucose (18F-FDG) uptake (maximum standard uptake value [SUVmax] = 2.9) on positron emission tomography (PET)/computed tomography (CT), which was difficult to distinguish from a malignant tumor. In this manuscript, we review the features of the rib hemangioma images and discuss the usefulness of PET/CT for distinguishing rib hemangiomas from malignant tumors. We discuss the surgical indications of rib hemangioma.
Case report
A bone tumor, 2 cm in diameter, of the fourth left rib was incidentally identified in a 68-year-old man upon a CT scan performed as part of his periodic examination for chronic pancreatitis. He did not want further investigation at the time, but the tumor had enlarged over half a year, and he then presented to our institution for a closer inspection.
He had no physical or visible symptoms. He had a history of myocardial infarction, hypertension, and chronic pancreatitis, but no history of malignancy. CT revealed a tumor in the neck of the fourth rib, 1.8 × 1.6 × 2.1 cm in size, presenting as a multicystic lesion with soap bubble appearance, with a slight cortical disruption, extraosseous lesion, but no expanded bone (Fig. 1).
CT image of the fourth left rib. The tumor occurred in the neck of the rib and showed bony disruption with a slight cortical disruption.
On magnetic resonance imaging (MRI), the lesion showed low to intermediate signal on T1-weighted (T1W) images, intermediate to high signal on the T2-weighted (T2W) images, and enhancement with gadolinium (Fig. 2a–c).
MR images of the affected rib. (a) T1W sequence, (b) T2W sequence, and (c) T1W fat-saturation sequence with gadolinium enhancement.
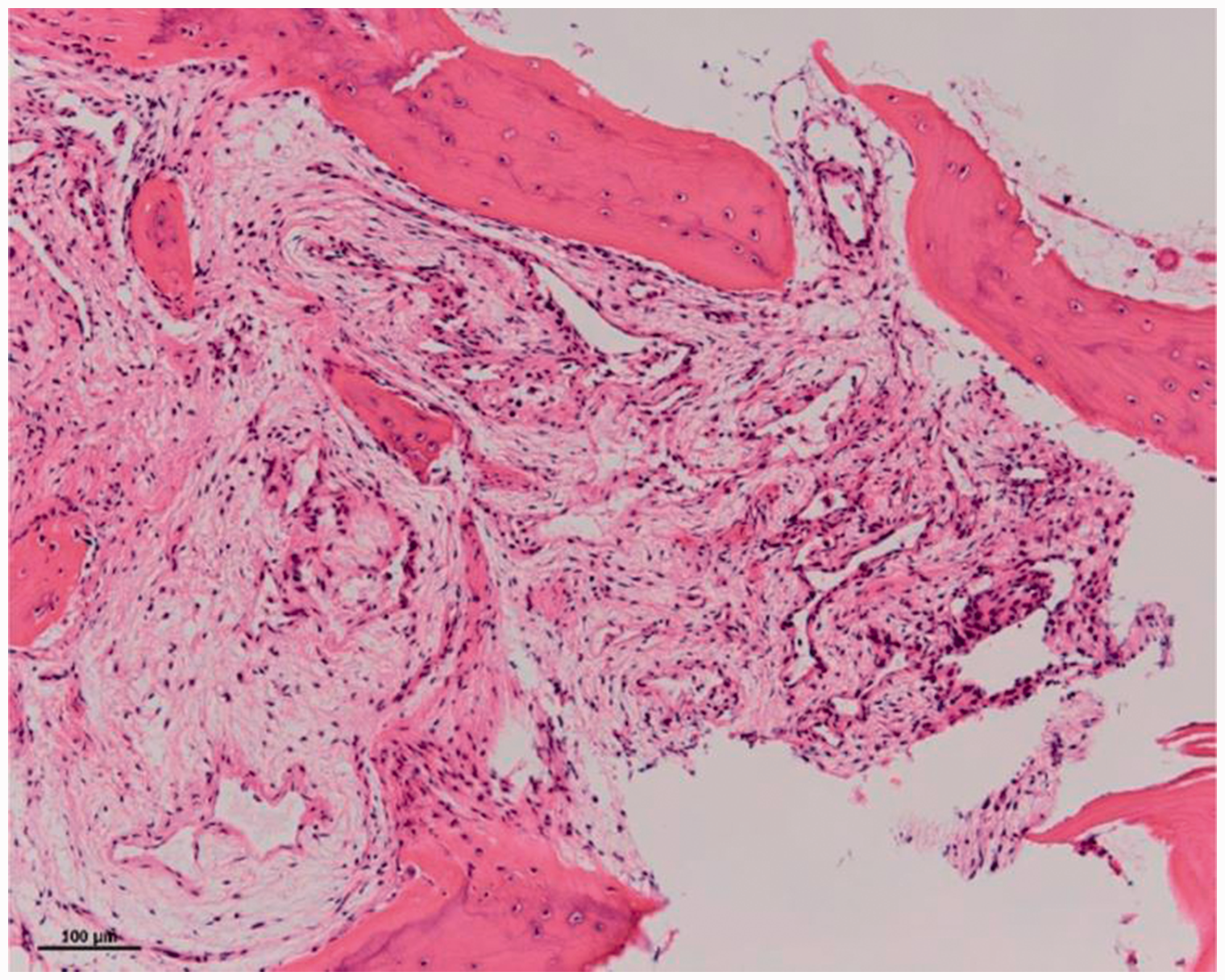
On PET/CT, the lesion showed relatively high 18FDG uptake (SUVmax = 2.9) (Fig. 3). Blood analysis demonstrated no remarkable findings and the tumor markers were negative. The tumor grew larger over the subsequent six months. In order to distinguish whether this was a malignant tumor, we performed open biopsy, with 20 mL bleeding. The specimen showed hyperplasia of the small vessels in the bone marrow (Fig. 4). No malignant findings of endothelial cells of the vessel were made and he was diagnosed as having a hemangioma of bone.
Slightly increased FDG accumulation in the tumor on PET/CT image. The SUVmax value of the tumor was 2.9. Hematoxylin and eosin stain (original magnification × 100). The tumor showed hyperplasia of the small vessels in the bone marrow, and a diagnosis of hemangioma was made.
Surgical resection of the rib was not conducted as he was asymptomatic and hemangioma of the bone being a benign bone tumor. The patient was discharged on the eighth postoperative day without any complications. The tumor showed calcification formation but without any further growth, as assessed by CT one year after the biopsy (Fig. 5).
CT image of the fourth left rib one year after the biopsy. The tumor showed calcification, but had not enlarged since the biopsy.
Discussion
Hemangioma represents 1% of primary bone tumors; the tumor occurs in the vertebral body or the skull in 60–80% of patients. Hemangioma of the rib is a relatively rare tumor. Hemangioma of the bone is usually asymptomatic, but one or more symptoms occur in 42.6% of cases if the lesion occurs in a rib (3).
Of primary rib tumors, 89% are malignant (2). The differential diagnosis of rib tumor is usually primary or metastatic. Malignant tumors include malignant lymphoma, myeloma, chondrosarcoma, osteosarcoma, and Ewing sarcoma (2). Thus, it is important to distinguish hemangioma from malignant tumors in the rib and this requires knowledge of the imaging features of rib hemangioma.
Hemangiomas in flat bones, including the rib, show cortical destruction with extraosseous mass and osteolytic lesions (4). We reviewed 22 previously published reports, 23 cases with 24 hemangiomas, obtained by using the key words “hemangioma AND rib,” and investigated clinical and radiological findings. Patients in these reports were aged 11–76 years.
Summary of the previous reported cases.

Hemangioma of the rib demonstrates low to intermediate signals on T1W images, intermediate to high signals on T2W images, and enhancement with gadolinium on MRI (15), similar to Ewing sarcoma or malignant lymphoma on MRI. Hemangioma of bone shows various signals, according to the proportion of vessel and lipomatous soft tissue elements. Thus, MRI images of hemangioma may not be specific for diagnosis.
18F-FDG PET/CT is increasingly being used to obtain more information about benign and malignant tumors, including metastatic tumors. On PET/CT, hemangioma of the rib presents with an SUVmax of 2.2–6.7 (3,12,23). Therefore, PET/CT may not provide useful information for distinguishing rib hemangiomas from malignant tumors.
A mainstay treatment for hemangioma is reported to be surgical resection (20). In our review of the literature, resection was conducted in all cases. In some cases, embolization was conducted preliminary to reduce intraoperative blood loss or bleeding after biopsy (20,21). Resection of the tumors was often performed without biopsy. Complications, such as massive bleeding and hematoma, may occur during a preoperative biopsy, complicating the process of distinguishing malignant tumors from benign entities (15). Preoperative needle biopsy before resection was found to be valuable because the most suitable treatment for the rib tumor could then be determined (12). However, in some cases, resection was performed after the diagnosis of rib hemangioma by means of needle biopsy, because it was not possible to exclude the possibility of malignant tumor (3). We chose to use open biopsy, because the tumor occurred in the neck of the rib and obtained enough specimen with little bleeding.
Hemangioma is a benign tumor; hence, we did not perform surgical resection of the tumor. The tumor in our case showed calcifications and did not enlarge over the duration of one year after the biopsy (Fig. 5). Close observation without surgical resection may be feasible if the tumor is diagnosed as hemangioma by means of needle biopsy.
Preoperative embolization of large rib hemangioma can reduce the size (20), and cement or alcohol injection have been conducted as treatment of vertebral hemangiomas (24).
If observation for rib hemangioma is decided, such percutaneous treatment might be one of the optional treatments.
In conclusion, the most common feature on CT was expanded bone. Observation without resection might be one of the treatments for rib hemangioma.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.