
Abstract
Background
Since multiparametric magnetic resonance imaging (mp-MRI) of the prostate exceeds 30 min, minimizing the evaluation time of significant (Gleason scores > 6) prostate cancer (PCa) would be beneficial. A reduced protocol might be sufficient for the diagnosis.
Purpose
To study whether a short unenhanced biparametric MRI (bp-MRI) matches mp-MRI in detecting significant PCa.
Material and Methods
A total of 204 men (median age, 65 years; mean ± SD, 64.1; range 45–75 years; median serum PSA level, 14 ng/mL; range, 2.2–120 ng/mL; median prostate volume, 60 mL; range, 23–263 mL) fulfilled the criteria for being enrolled. They underwent mp-MRI and prostate biopsy from January through June 2014. Of the included patients, 9.3% underwent prostatectomy, 90.7% had TRUS-bx, and 10.8 had MRI-targeted TRUS-bx. Two radiologists separately assessed the mp-MRI examination (T2-weighted [T2W] imaging, diffusion-weighted imaging [DWI], apparent diffusion coefficient map [ADC-map] and dynamic contrast-enhanced imaging [DCE]). Two months later, the bp-MRI version (T2W imaging, DWI, and ADC-map) was evaluated.
Results
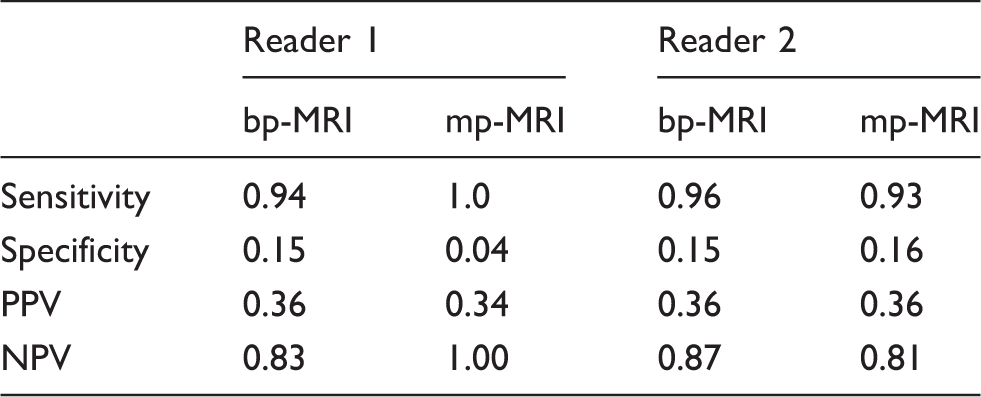
Reader 1: Assessing mp-MRI: 0 false negatives, sensitivity of 1, and specificity 0.04. Assessing bp-MRI: four false negatives, sensitivity of 0.94, and specificity 0.15. Reader 2: Assessing mp-MRI: five false negatives, sensitivity of 0.93, and specificity 0.16. Assessing bp-MRI: three false negatives, sensitivity of 0.96, and specificity 0.15. Intra-reader agreement Cohen’s Kappa (κ) was 0.87 for reader 1 (95% confidence interval [CI], 0.83–0.92) and 0.84 for reader 2 (95% CI 0.78–0.89).
Conclusion
Bp-MRI is as good as mp-MRI at detecting PCa. A large prospective study seems to be strongly warranted.
Keywords
Introduction
The diagnosis and treatment of insignificant prostate cancer (PCa) defined as Gleason scores ≤6 is a problematic issue. Insignificant PCa is found in approximately 19% of referred patients at Herlev Hospital and it would be preferable to avoid TRUS-bx or reduce the number of biopsies. The PCa diagnosis is currently based on a histological examination of 10–12 TRUS-bx cores (1). The standard biopsies do not cover all parts of the prostate; hence the biopsies are not representative of the whole gland in most cases. Furthermore, TRUS-bx has complications: bleeding, 14.5%; prostatitis, 1%; and urosepsis, 0.3% (1). In addition, ultrasonography cannot identify more than 50% of the cancers (1).
Magnetic resonance imaging (MRI) is more accurate in detection (2–4), pinpointing that significant cancer and biopsies should only be taken from areas identified by MRI. Implementing a policy involving fewer biopsy examinations and fewer cores would reduce the workload of the pathologist and the risk of complications.
The scanner occupation time for a multiparametric MRI scan (mp-MRI) is about 45 min (scan-time < 30 min). This is too long for a diagnostic procedure, whose only goal is to find the presence of significant PCa or rule it out. Based on our 4 years of experience, we have chosen three sequences that might be suitable in answering the question: Does the patient harbor significant or insignificant/absent PCa? (5–8). In order to confirm the usefulness of the selected sequences we undertook a retrospective study comparing biparametric MRI (bp-MRI) to mp-MRI in the diagnosis of significant PCa.
Material and Methods
A total of 216 patients underwent mp-MRI and biopsy or prostatectomy of their prostate from January 2014 through June 2014. The study was approved by the Danish Data Protection (03228, ID: HEH-2014-093). The patients were identified through our RIS/PACS (Radiology Information System/Picture Archiving and Communication System).
Inclusion criteria
Patients were included if they had had a mp-MRI and a prostate biopsy with a time gap not exceeding 2 months, and the biopsy was not taken within the last 6 weeks before mp-MRI (because bp-MRI does not include a T1-weighted [T1W] sequence that could detect bleeding after the biopsy).
Exclusion criteria
Patients were excluded if the histological examination only revealed high-grade prostatic intraepithelial neoplasia (high grade PIN) or if the histological examination was inconclusive. They were also excluded if the images were not satisfactory (multiple artifacts from, for example, total hip replacements, patient movements).
MRI examination
All mp-MRI examinations were performed on a 3.0-T clinical MRI system (Ingenia, Philips Healthcare, Best, The Netherlands) and according to European Society of Urogenital Radiology (ESUR) guidelines of 2015 (9).
Mp-MRI examination
Peristaltic movement was suppressed with an intravenous injection of hyoscinbutylbromid (Buscopan, 20 mg/mL, injection fluid, Boehringer Ingelheim GmbH, Ingelheim am Rhein, Germany) and with an intramuscular injection of Glucagon (GlucaGen 1 mg, Novo Nordisk A/S, Bagsværd, Denmark) in absence of contraindications (Buscopan: allergy of hyoscinbutylbromid or trouble emptying the bladder, narrow alimentary canal, etc.; GlucaGen: allergy of glucagon or lactose or adrenal gland tumor).
Mp-MRI includes triplanar (axial, sagittal, and coronal) T2-weighted (T2W) turbo spin-echo images, diffusion-weighted images (DWI) in the axial plane with multiple b-values (b = 0, 100, 800, 2000) where b = 2000 s/mm2 is used for visual assessment and the remaining three b-values in the calculation of the apparent diffusion coefficient-map (ADC-map) and dynamic contrast-enhanced (DCE) T1-weighted (T1W) images in the axial plane (Fig. 1) (3).
A 74-year-old man with a Gleason score 7 (4 + 3) cancer. The cancer is located posterolaterally at left in the peripheral zone. An mp-MRI revealed a lesion that was categorized as significant cancer.
Mp-MRI protocol.

The scanned sequences included in the bp-MRI.
FOV, field of view; NSA, number of signal averages; TE, echo time; TR, repetition time.
Bp-MRI examination
From the mp-MRI three sequences were selected and copied: T2W images in the axial plane, DWI likewise in the axial plane with multiple b-values (b = 0, 100, 800, 2000), the b = 2000 s/mm2 is used for visual assessment and the remaining three values were used in the calculation of the ADC-map (Fig. 2). The scan time would have been approximately 17 min and the scanner occupation time only slightly longer as no drugs including contrast medium were used.
A 61-year-old man with a Gleason score 7 (3 + 4) cancer. Three MRI-targeted TRUS-bx with Gleason score 7 (3 + 4) in 90%, Gleason score 7 (3 + 4) in 100% and Gleason score 7 (4 + 3) in 80%. A bp-MRI with a T2W imaging in axial plane, an ADC-map, and a DWI b-value = 2000 and revealing an anterior lesion that was categorized as significant cancer.
Histopathologic examination
The results of the histologic examinations were obtained from the national pathology bank (a database for pathologic reports). In all cases the specimens were treated according to the standard procedure of the Department of Pathology at Herlev Hospital. The specimen would either be a prostatectomy specimen or a set of biopsies. If it was a prostatectomy, the entire specimen was fixed in 4% buffered formalin for 3–5 days according to specimen weight. The surfaces were inked with four colors corresponding to the axes right–left and anterior–posterior and the specimen was then cut into 4-mm thick slices perpendicular to the posterior surface. The apex and basis slices were further cut into sagittal slices and processed in standard cassettes, while the intermediate slices were processed as whole mount slices. The vesicles were cut off approximately 5 mm from their basis and the bases of the vesicles were included in the slices from the base of the prostate. Slices close to the suspect volume and a longitudinal slice from the apical region of the vesicles were processed in small cassettes. All slices were paraffin-embedded and 3–4 -µm slices were cut and stained with hematoxylin and eosin (H&E). Areas with adenocarcinoma were marked on a template depicting the axial slices in order to make the comparison with the MRIs more accurate.
If the specimen consisted of biopsies from the TRUS-bx/MRI-targeted TRUS-bx, they were placed separately in cassettes, fixed for at least 4 h in 10% buffered formalin, and embedded in paraffin. They were then cut at two levels and stained with H&E. Biopsies with suspicious lesions were cut at further levels and if relevant stained immunohistochemically for presence of basal cells (high molecular weight antibody 34βE12) and AMACR (antibody P504S). Areas with adenocarcinoma were Gleason scored according to the 2005 ISUP modification (10) and the amount of adenocarcinoma was given in percent. Moreover, the presence of high grade PIN and/or inflammation was stated.
Reader assessment process
All the images were assessed via our iSite module (iSite Radiology, Philips Healthcare, Best, The Netherlands). The images were anonymized prior to assessment and using a common reporting questionnaire (Fig. 3), two radiologists, specialists in mp-MRI of the prostate, assessed all six sequences determining whether a significant lesion was visible or not. Whether the images were categorized as significant or not were down to the subjective opinion of the experienced readers. They made a fast and consistent visual assessment of the images sequence for sequence (significant cancer yes/no). Lastly, they concluded if this set of images had a significant cancer lesion or not (Fig. 3 [question 7] and Fig. 4 [question 5]). No grading was used to assess the images; they were only categorized according to harboring significant cancer or not. This was done separately, but with the same controller present. The controller made sure that the specialists assessed each mp-MRI the same way and noted the findings in a table. During the next 2 months, the radiologists did not look at the images included in the study, but continued to report new examinations (>100) as part of their normal assignments. All images that would have been obtained according to the proposed bp-MRI protocol were examined (Fig. 2). The same evaluation procedure was undertaken of the three sequences (Fig. 4).
Reporting questionnaire used on mp-MRI to classify as significant cancer or not. Reporting questionnaire used on bp-MRI to classify as significant cancer or not.

Statistical analysis
All analyses were performed with statistical software (R studio) with the level of statistical significance set at P < 0.05 (11). The pathology was categorized by Gleason score. Gleason scores were divided into two groups (significant/insignificant) non-significant PCa lesions (Gleason ≤ 6 [3 + 3]) were separated from significant PCa lesions (Gleason > 6). This was compared with the reader assessments. If the conclusion of the reader was significant cancer and the pathology showed significant cancer of the specimen, that was equaled as the same result. Sensitivity and specificity, positive predictive value (PPV) and negative predictive value (NPV), and accuracy were calculated for both readers and both methods. In addition, a comparison of the mp- and bp-readings was made (intra-reader agreement).
Results
Clinical-pathologic features in the study population (n = 204).

Number of patients with percentages of total in parentheses.
The assessments from Reader 1 and Reader 2 are compared with the histologic results. Then the true positives, true negative, false positives, and false negatives can be extracted.

The detection rates of Readers 1 and 2.
Comparison of false negatives.

As a measurement of intra-reader agreement, Cohen’s Kappa (κ) was calculated. κ was 0.87 for Reader 1 (95% confidence interval [CI], 0.83–0.92) and 0.84 for Reader 2 (95% CI, 0.78–0.89) (12).
Discussion
To the best of our knowledge the three sequences of the bp-MRI and the six of the mp-MRI has hitherto never been compared in the same patient with regard to presence or absence of significant PCa.
Our study showed a very good agreement between the two examinations according to Cohen’s Kappa (12), indicating that a short examination may be sufficient in patients that were biopsy naive (5,6). Mp-MRI is recommended by the ESUR prostate group (9).
The bp-MRI may have increased the amount of false positives (Table 3) as it lacks some of the sequences of the mp-MRI (13), but we would rather have too many false positives than to miss significant cancer (i.e. avoiding false negatives). Consensus reading may be the way to keep this number low (Table 5). Further actions to keep the false positives low are discussed later.
The present study shows that if the consensus rule is held to be that identification by one reader of the presence of significant cancer is sufficient, there would only be one false negative examination (i.e. both readers mis-identified the presence of significant cancer) when bp-MRI was performed. Using the same rule, mp-MRI had no false negative examinations. The single false negative case was in a stage T1c patient, who had a MRI-targeted TRUS-bx with a Gleason score of 7 (3 + 4) in 2/10 biopsy cores. In one of two biopsies, the Gleason score was 7 (3 + 4) in 40% and in the other the Gleason score was 7 (3 + 4) in 30%. The Gleason score might be the reason why the cancer was not detected in the bp-MRI (Fig. 5). Furthermore, the lesion was only 4 mm on the mp-MRI/bp-MRI and located on the apical edge of the prostate tissue. When the case was re-examined it was clear to both readers that they should have detected this lesion and that it should have been categorized as significant at the first reading. This is an example of what we can do better and what we hope to learn from.
A 69-year-old man with a Gleason score of 7 (3 + 4) in 2/10 biopsy cores. An mp-MRI revealed a lesion that was categorized as insignificant cancer.
The rate of false negatives was 0.49% with bp-MRI and 0.0% with mp-MRI in the current study. Thus MRI outperforms TRUS-bx which has a false negative rate of approximately 25% (14). Hence it seems reasonable to use bp-MRI as a first line sorting method but it would be preferable to have less false positives. This suggests that the readers need further knowledge/education in separating the true positives from the false ones. We hope this is achieved with a closer cooperation with the pathologic department. We need to discuss and compare findings even more than we do now.
The sensitivity of the bp-MRI was in the range of 0.94–0.96 and of the mp-MRI 0.93–1.00 (Table 4). These figures are as good as or better than the figures in a review by Fütterer et al. reporting a sensitivity in the range of 0.58–0.96 (15). The lower sensitivity may be due to the fact that the studies enrolled in the review demonstrated diversities in the definition of significant cancer (15). Based on our material, it seems reasonable to conclude that the bp-MRI may be suitable for identifying significant cancer. Furthermore, sensitivity and specificity are not dependent on prevalence as these are more representative of the general population than NPV and PPV due to the selection bias discussed below.
The study population consisted mainly of patients who had previously had a biopsy of their prostate. This may affect the results in at least two ways: (i) the study population has a higher prevalence of cancer than a normal population, which affects the NPV and PPV, but not the sensitivity and specificity; or (ii) it could have biased the readers (observer bias) into diagnosing more cancers, because they knew this was more likely.
The PSA levels were not the true PSA levels. Some of the patients were undergoing treatment with 5-alpha reductase inhibitors like Finasterid (Finasterid 5 mg, PharmaCoDane, Herlev, Denmark) or Dutasterid (Avodart, PharmaCoDane, Herlev, Denmark) which affects the PSA levels, halving the actual level (16).
When the Gleason scores were divided into two groups (significant/insignificant) the threshold was set at Gleason score 6 (3 + 3) (Table 2). It is a matter of active debate whether the threshold should be set at 3 + 4 instead and whether the volume and extra prostatic extension should be included (15,17). Extra prostatic extension and volume of the lesion could have been used to distinguish between significant and insignificant cancer but only one anatomical sequence is included in the bp-MRI and therefore extra prostatic extension cannot be detected. Furthermore, we wanted a fast workflow so measuring the lesion was not an option (18).
The study has some limitations. First, the study is retrospective and most of the patients had been biopsied previously. This confounds the purpose of bp-MRI being used to detect significant cancer and thereby determine whether a biopsy should be performed or not. Second, the true negatives reflect the number of patients who could possibly avoid biopsies. Unfortunately, the number of true negatives is underestimated as the population mainly consists of previously biopsied patients. So the true negatives in this study can only be used as an indication of the potential number due to selection bias. A more accurate assessment of how many patients could avoid biopsies demands a prospective study on a larger scale. A third limitation is that only 10.8% had an MRI-targeted TRUS-bx. Therefore we cannot be sure that the biopsies were from the foci detected on the mp-MRI/bp-MRI. If the foci found in MRI were not biopsied it will appear negative when it might not be, a kind of false negative. A fourth limitation is because one of our main focuses was to avoid false negatives then when in doubt the readers tended to classify the cancer as significant cancer rather than insignificant. This may have affected the specificity. The bp-MRI was 0.15 and the mp-MRI 0.04–0.16 compared with 0.23–0.87 in the review (15). This suggests that we need to work more on our ability to find images which are not harboring significant caner. At the start of the study, only PI-RADS (Prostate imaging reporting and data system) version 1 was available (19). PI-RADS version 1 was a scoring system, where you multiplied amounts from each sequence and then the sum decided if the lesion was suspicious of cancer or not. As the bp-MRI has fewer sequences compared with the normal mp-MRI it would automatically have had a lower score and thereby a lesion would be less cancer suspect on bp-MRI compared with mp-MRI only because of the fewer sequences. Because of this we could not use PI-RADS in comparing the two kinds of MRIs. This is a limitation as we later learned for instance that T2W imaging should be preferred in the transition zone from PI-RADS v2 (18). PI-RADS v2 would have been use if the study was done today. Fifth, the mp-MRI images in the study were acquired after IV buscopan/glucagon and the bp-MRIs were deduced from the mp-MRIs. We assume that images without peristaltic inhibition would have the same quality because we will not be using IV buscopan/glucagon when performing the bp-MRIs in the future. This is a limitation as we cannot be sure of this yet.
In conclusion, bp-MRI is as good as mp-MRI at detecting PCa. This study has shown that the mp-MRI can be reduced and still be effective in detecting PCa but a large prospective study is needed. We need to assess the bp-MRI without as many limitations and on a much larger scale before it can be considered as a new standard procedure.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.