
Abstract
Chronic mechanical irritation (CMI) of the oral mucosa has been proposed as a risk factor for oral cancer (OC), but the available evidence is limited and controversial. One of the main limitations is the lack of proper criteria to define and classify CMI. The objective of this narrative review is to apply the Bradford Hill causality criteria to assess such an association based on the published literature. The level of evidence is not conclusive, mainly due to methodological shortcomings. Hence, to systematize future CMI research, we recommend the following items should be included: a clear definition for CMI, ascertaining any temporal association, recording all types of CMI: dental, prosthetic, and functional. Finally, it is important to emphasize that studies dealing with risk factors for OC should not only be restricted to established factors such as tobacco, alcohol, and areca nut consumption but should also consider other factors including the patient’s dental condition. In this regard, CMI, tooth loss, periodontal disease, and many others could be included. The causality criteria set out by Bradford Hill could be used for studying different controversial risk factors for OC.
Introduction
Historically, advanced age, tobacco, and alcohol consumption are considered the most important risk factors for oral cancer (OC). In the recent past, due to advances in epidemiological and biomolecular research, other risk factors for OC have been identified. Among them, there are emerging and controversial factors. 1 Dental factors such as periodontal disease, tooth loss, and chronic mechanical irritation (CMI) to the oral mucosa belong to this group. CMI, also called chronic trauma to the oral mucosa, is the result of repeated mechanical irritative action by an intraoral injurious agent. Defective teeth (malpositioned or with sharp or rough surfaces because of decay or fractures), ill-fitting dentures (sharp or rough surfaces, lack of retention, stability or overextended flanges), and/or parafunctional habits (e.g. biting of oral mucosa or sucking, tongue thrusting), acting individually or together, could all be responsible for such mechanical irritation. 2
The current evidence supporting the association between CMI and OC is limited. In a recent meta-analysis of this association, 22 studies satisfied the requirements that allowed evaluating the relationship between a traumatic factor and OC. 3,4
The aforementioned meta-analysis and the studies in which they were based showed an important progress towards considering CMI as a risk factor for OC. As it is expected that more studies on the topic would be conducted, it is necessary to set a standard and uniform criteria to define CMI cases.
To determine if CMI is a risk factor for OC, it is necessary that this relationship fulfills causality criteria. Accordingly, the causality criteria of Bradford Hill can be used as the reference. 5 As the author himself expressed, they are not strict rules for fast application but could be better regarded as general guidelines. The causality criteria of Bradford Hill have evolved with time, considering that in the beginning they were applied only to unicausal diseases. It's application in the epidemiological field has demanded an adaptation to multifactorial and multistage diseases, such as OC. 6 The Bradford Hill criteria can aid researchers in filling the gaps within the body of literature, either to reveal a causal relationship, to refute an association or to identify areas where more research is needed. 7
Thus, the aim of this narrative review is to assess the relationship between CMI and OC using the Bradford Hill causality criteria, to identify methodological flaws, propose reliable measures to assess CMI and to provide future directions for research.
Discussion
Hill’s criteria are widely accepted to assess causality, offering the best guidance for causal inference. However, there is no agreement on what weightage should be given to each criterion, so a more practical approach would be to use them to estimate the likelihood that an association is causal. 8 The Bradford Hill criteria are listed in Table 1 and would be discussed in that order.
Bradford Hill’s criteria.
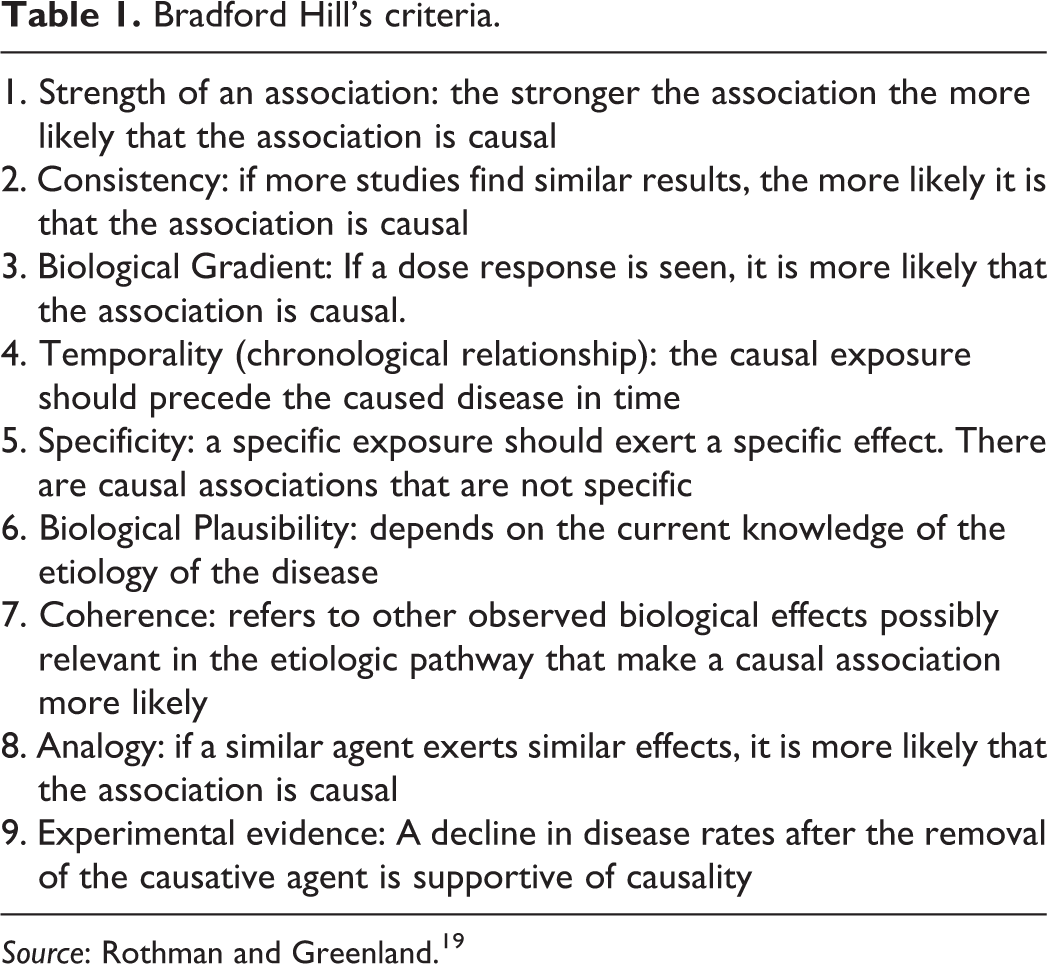
Source: Rothman and Greenland. 19
Strength of an association
In studies analyzing the statistical association between a disease and a potential risk factor, the stronger the statistical association the greater the weight, provided that bias and confusing factors are controlled with an appropriate methodological design. 6 Strength is no longer interpreted as the magnitude of an association. Understanding of multifactorial diseases has been improved because of the existence of determinant risk factors that are small in magnitude yet statistically strong. Today, statistical significance is the accepted benchmark for judging the strength of an observed association, and thus its potential causality. 7
However, causal inference through epidemiological research should be done with caution. Once sufficient studies have been conducted in diverse settings, adequately limiting random error (an intrinsic property of a stochastic universe), systematic error (bias) and logical error (confounding), then the causal nature of an association can be properly assessed. 6
The random error is a variation that is generally regarded as strictly random. The main source of it is the selection of the study sample, which is why it is also known as sampling error. The most effective way to reduce this error is by increasing the size of the study sample. This enhances the accuracy of the risk calculation and, consequently, the study. In our experience, we found a significant statistical association (p < 0.0001) between CMI and OC, both in cross-sectional 2 and in case-control studies. 9 OC studies recording CMI have relatively smaller samples than those on alcohol and tobacco consumption. This problem could be tackled carrying out a meta-analysis, which may reduce sampling error. Be that it may, there are not many meta-analyses about CMI and OC. Among those, two are worth mentioning, are the one by Manoharan et al. and another by Singhvi et al. 3,4 Both papers found a significant statistical association between OC and CMI in relation to wearing defective prosthetic devices.
The systematic error is the product of defects in the selection method of the sample or in the information gathering process, producing flawed outcomes called bias. Information bias is a failure in the measurements for risk factors of a selected disease, rendering inadequate information. Incorrect measurements could produce a wrong assessment of the sample. There are many ways in which information bias can happen, and some examples are as follows:
When there is a defective assessment of a variable: Essentially, CMI can only be properly recorded with an objective clinical lesion that should be in direct contact with an injurious factor: teeth or dentures. Furthermore, always taking into account potential functional factors that could increase any interaction. Finally, such contact should be long-standing. Nevertheless, in both meta-analyses published on this topic, most of the studies did not have clear criteria to define the CMI, or they assessed partially the potential sources of CMI.
3,4
In 2010, Piemonte et al.
2
published a study on CMI and OC, where CMI was clearly defined and using the criteria required to state its presence (Table 2). Certainly, it could be improved through a detailed description on how to identify CMI, considering individually each CMI factor: dental, prosthetic, and functional.
The researchers electively seek and gather data (deliberately or not) in such way that the variable under study loses reproducibility. To prevent this bias, CMI could be assessed in a double-blind fashion using predetermined criteria. Only the study by Piemonte et al.
9
used that methodology, rendering a correlation coefficient of 1 (kappa), which suggests that CMI could indeed be a reproducible variable.
The patients under study have an inaccurate or an incomplete recollection of the events in relation to the studied variables. This so-called recall bias is usually due to the long development time of OC, and usually the individual cannot remember the evolution exactly. Furthermore, the patient could not remember since when the potentially injuring factor existed. Recall bias is inherent to CMI and OC, and its impact can only be decreased using a rigorous clinical inspection and anamnesis, and proper assessment of dental, prosthetic, and functional factors in each case.
Chronic mechanical irritation criteria.

Some authors have suggested that CMI should produce a preexisting lesion before evolving into a carcinoma, 3 and chronic traumatic ulcer (CTU) could be one such presentation. Herein we find one of the main hurdles: being able to develop a study model that allows analyzing the relationship between CTU and OC. Case-control studies of CMI could not be fulfilled using the same research setting as other oral potentially malignant disorders (OPMDs), such as leukoplakia or lichen planus. Those diseases can be studied using cohorts (follow-up studies), and they often have lesions in close proximity to the malignancy or in additional areas of the oral cavity. Whereas, CTU would be exactly in the same location where subsequently the OC is going to arise. CTU—or any other CMI lesion—rarely exceeds 2 cm in diameter, while 60–70% of the newly diagnosed OC is seen at advanced stages, with a size larger than 4 cm. 10 Therefore, more than half of the OC have a size far larger than most of the CMI lesions. On account of this, it is logical that even if an OC has indeed originated from a CMI lesion, it most likely would be completely transformed (hidden) as a consequence of lateral tumor growth. To consider indispensably the presence of a CMI lesion previous to OC appearance is a proposal that generates bias and an under-registration of the CMI associated cancers, because in many cases CMI lesions simply could not be seen.
To reduce logical error, the confounding factors have to be carefully controlled, since these are very common in multifactorial diseases such as OC. Causality in OC should be analyzed under multifactorial models, considering that not a single factor—alcohol and tobacco included—could explain all of the OCs. As a matter of fact, not every person who consumes tobacco and/or alcohol, even in large quantities, develop OC, so these factors could not be considered as sufficient causes. On the other hand, not all OC individuals are tobacco or alcohol consumers, which indicates that they are neither necessary factors for OC. Thus, the association of different factors in the same patient could be considered a sufficient cause to the development of OC. 11
In a multifactorial context, a factor with low prevalence could become important if these complementary factors are very common. Thus, the strength of any given causal risk factor is dependent on the distribution of the other causal factors in the population. 12
Consistency
If the same association is observed repeatedly in different populations/studies, particularly using diverse methodologies, a causal relationship would be greatly reinforced. On the other hand, shared flaws in different studies would tend to replicate the same wrong conclusion. 13 Conversely, the results of the studies of the same phenomenon may vary because of an interaction with another variable, which warrants further investigation, rather than a noncausal conclusion. 6
Regardless of methodological limitations, few case-control studies have addressed the relationship between CMI and OC, most of them focusing only on injury caused by removable prosthetic devices. 3,4 The ones addressing dental CMI have produced conflicting results. Initially, this lack of consistency could be explained by the methodological heterogeneity to identify CMI. Almost every study analyzes the relationship between CMI and OC using only a single potential CMI source: teeth or dentures. Moreover, some do not properly describe when a tooth or a prosthetic device could be regarded as an irritative factor. The mechanical irritation is produced when an object harder than the oral mucosa contacts it, but the actual source of CMI could induce different lesions. 14 Accordingly, it is essential to register whether CMI was produced by teeth or dentures. Indeed, having defective teeth/denture does not mean that it would produce a CMI lesion. A patient could have a diastemata, tooth loss, dental malposition, and defective teeth/dentures with no clinical lesions arising from them at all. Bearing this in mind, we set the criteria that not only a clinical lesion is necessary to determine CMI, but also that the lesion should be in direct contact with the potential injuring factor, whatever it may be. Finally, only few studies included functional factors—parafunctional and dysfunctional—in studying CMI. 2,9,15
According to Lazos et al., almost 75% of the CMI lesions arise from a joint action of a dental and/or prosthetic factor plus a functional factor (e.g. tongue thrusting). Therefore, for teeth to produce damage to the oral mucosa, typically another variable is required: a functional factor, which has not been considered in most of the published studies. In view of all the foregoing reasons, the mere presence of defective tooth or denture could not be regarded as an indicator of CMI. 15
Biological gradient
Refers to the dose–response relationship between variables, meaning that higher exposures may produce greater effects, nonetheless, it may present at a biological threshold. 6
Most studies indicate that the presence of defective or fractured tooth is not related to OC. 9,16 -18 As we explained in the “Consistency” section, to actually produce the mechanical irritative lesion, often dental and prosthetic factors need to be combined with functional factors. Moreover, to produce a CMI lesion, only a single tooth is enough, regardless if there are other teeth with irritative potential. In summary, the number of potential injuring factors is not a useful variable to gauge OC risk from CMI.
The CMI exposure time has not been studied accurately either. To some extent, this is a by-product of it’s recording being conditioned by recall bias, but more importantly, simply because it hasn’t been recorded at all. Even with this limitation, Lazos et al. found that OC associated with CMI presented higher exposure time to CMI than other traumatic lesions. 15 Furthermore, OC cases associated with prosthetic factors presented higher exposure time than the ones associated with dental factors. This could be due to the fact that the dental factors are fixed—cannot be modified by the patient—having a continuous action, and consequently, they require less time to produce damage. On the other hand, the irritative action period of dentures could be reduced by the patient when they remove the denture, needing more time to induce a lesion. This suggests that persistent exposure to CMI could play an important role in the OC development. 15
The CMI intensity is difficult to be assessed. Sometimes an apparently similar irritative source can produce different lesions: indentation, atrophy, or ulcer. Nonetheless, it is already difficult to define the presence of CMI, so defining CMI intensity would be even harder.
There is also limited evidence of the biomolecular process studying CMI with OC. Maybe the measurement of some molecular intermediaries (e.g. methylation, chronic inflammation, and others) can aid clarification of a possible dose–response relationship.
Temporality (chronological relationship)
As per definition, an advocated factor should precede the effect to be considered as a cause. This is the only indispensable condition to establish a causal relationship. 19 According to Hill, temporal direction might be difficult to establish if a disease develops slowly and initial forms of disease are difficult to identify, as it happens in OC. 13
Mechanical irritation usually produces painful ulcers that are quickly submitted to consultation and treatment. For that reason, persistence ensues only in a minor number of cases, possibly because of decrease or loss of sensitivity. Furthermore, unlike another OPMD like lichen planus or leukoplakia, it is not possible to conduct study cohorts of CMI. Ethically, it would not be conceivable to leave CMI untreated in order to study its evolution. 15 When the causative factor of a CMI lesion is addressed, it typically heals quickly, disrupting any microenvironment inflammation and other conditions that could foster carcinogenesis. 20 Hence, study cohorts in humans may not be used to determine the relationship between CMI and OC.
Some authors have proposed that a CMI lesion should exist before OC ensues. Even though some case reports described a carcinoma in situ located on a CTU border, those are based on temporally fortuitous incidents, and therefore difficult to systematize. 21
Only a few studies dealing with CMI and OC have stated chronological relationship. Some authors use recurrent denture-related sores to display temporality. 22,23 Even though evolution time is not specified in those studies, factual data of trauma occurring before the OC diagnosis are referred to. It is more appropriate to determine CMI when there is an objective lesion—malignant or not—in direct contact with a potential injurious factor, and such mechanical factor should be present before the appearance of the lesion. This requires a meticulous anamnesis and analysis, in order to determinate when the mechanical irritation started. Figures 1 to 9 display clinical cases with the proposed requisites for establishing CMI.

Male, 44-years old, with a verrucous carcinoma (T2) on tongue border. Linguoversion of 35 and 37; rough lingual surface of the lower partial denture for at least 48 months.

Female, 53-years old, with a squamous cell carcinoma (T2) on tongue border. Palatoversion of 27; mandibular and maxillary transverse deficiency, tongue thrusting, and absence of canine protected occlusion for at least 36 months.

Male, 61-years old, with a squamous cell carcinoma (T4) on tongue border. Tongue thrusting on isolated 45 for at least 24 months.

Male, 71-years old, with a squamous cell carcinoma (T3) on buccal mucosa. Broken teeth, absence of canine protected occlusion, and bruxism for at least 60 months.

Male, 74-years old, with a squamous cell carcinoma (T3) on tongue border. Absence of 25 and 27, absence of canine protected occlusion, and tongue thrusting for at least 120 months.

Female, 75-years old, with a squamous cell carcinoma (T2) on buccal mucosa. Sharp crowns of upper and lower complete dentures, absence of canine protected occlusion, and loss of vertical dimension for at least 24 months.

Male, 79-years old, with a squamous cell carcinoma (T3). Broken lower molar in tongue border, already extracted, 4 months prior to taking the illustration.

Female, 82-years old, with a verrucous carcinoma (T2) on ventral tongue. Overextended lower denture used for at least 180 months.

Female, 83-years old, with a squamous cell carcinoma (T2) on dorsal tongue. Upper denture without retention and denture stabilization with tongue for at least 3 months.
The temporal association between CMI and OC has also been questioned arguing that the mucosal irritation could be the product of tumor growth. In this scenario, CMI would be a consequence and not the cause of tumor growth, so it would be expected that larger tumors are more associated with CMI. Piemonte et al. assessed the association of OC to CMI depending on tumor size, comparing small (Tis, T1 and T2) with big tumors (T3 and T4), finding no significant differences. 9 This suggests that CMI could be found in early OC stages and could play a role at least as a promoter and progressor of oral neoplasms.
Specificity
A factor that influences specifically a particular outcome. More specific the association is, stronger is the cause–effect association. Nonetheless, this is a rather ambiguous topic, considering that a single factor could generate multiple effects, and also multiple factors could induce the same effect.
In chronic diseases such as OC, there is not a single known factor present in all cases. 24 For example, not all OC patients are smokers and tobacco consumption is not always present in OC.
So to tackle specificity, it is useful to apply the multicausal criteria of Rothman. This model of causation describes causes in terms of sufficient causes and component causes, stressing the important principles such as multicausality and interaction between component causes.
12,19
The Rothman model offers the following features:
None of the component causes are superfluous: all the possible causal factors should be considered, not only the most studied ones such as tobacco and alcohol, as it has been done in most of the studies about OC risk factors.
25
No specificity required: the same effect could be produced by different causes; OC could develop even in a nonsmoker, non alcohol user and may be due to another cause.
A component cause could be part of more than one sufficient cause for the same effect. If a component cause is part of sufficient causes for a given effect, it is referred as a “necessary cause.” Until now, no studies have been able to prove that tobacco and/or alcohol are associated with all OCs, so neither of them are sufficient causes but we recognise them as major risk factors associated with the disease.
The same component cause can take part as different sufficient causes for several effects. In relation to CMI, this could mean that according to other existing causes (age, medication, habits, etc.), CTU, denture-induced fibrous hyperplasia, and even OC could arise because of CMI.
Two-component causes of a sufficient cause are considered to have biological interaction, so none of them may act by itself. However, the level of interaction could be subject to other component causes. For example, even in a former smoker, in a mucosa initiated by tobacco, CMI could produce a promoter effect, allowing the cancer development.
The multicausal model directly affects the strength of an association. To complete a sufficient cause, any given component cause that requires other components with low prevalence is thereby a weak component cause. On the other hand, a component cause which requires factors nearly ubiquitous to complete the sufficient cause is a strong component cause. Thus, the strength of a causal risk factor depends on the prevalence of the component causes.
Biological plausibility
Biological plausibility relies heavily on the current knowledge, which explains why many previously rejected relationships are accepted later on, and vice versa. 19 Researchers might assign a higher weight to the evidence if it agrees with their own prior opinion. The question remains on how to weigh prior opinions relative to observed results. 13
The available evidence suggests that CMI could play at least a role as a tumor promoter, but the pathological mechanisms are still not completely understood. Among others, proposed pathways include enhanced carcinogen penetration, increase of replication and division of cells, creation and preservation of an inflammatory microenvironment.
Carcinogens penetration is frequently suggested to explain the CMI's role in the oral carcinogenesis. Nevertheless, this hypothesis does not have concrete evidence. If CMI could act by increasing exposure or penetration of carcinogens, its role would be tied to the absorption of a carcinogen. Thus, if CMI only allowed more tobacco substances to be absorbed, it should have a statistically significant association with OC in smokers, whereas it's effect in nonsmokers should be nonexistent. The same could be said regarding alcohol consumption. However, Piemonte et al. found that CMI consistently showed a statistically significant association with OC in all groups disregarding alcohol or tobacco consumption. 9 Consequently, the promoter role may be exerted through other ways. CMI, and also episodes of CTU of the oral mucosa, could expose the basal cells, allowing human papillomavirus (HPV) penetration. This mechanism has been proved in animal experiments but not in humans. 26
CMI induces a hyperproliferative condition and an inflammatory microenvironment that could foster carcinogenesis, through the release of chemical mediators and oxidative stress. 27 Thus, sites exposed to chronic irritation could develop metaplasia (major change of the tissue phenotype), which represents an epigenetic reprogramming. 28 It has been shown that cancer could arise in an area of metaplasia, and usually, the sequence metaplasia–dysplasia–carcinoma is seen, as in Barrett’s esophagus. 29 Experimental, clinical, and epidemiological studies have shown a strong association between chronic inflammation and cancer, linking the persistence of an inflammatory environment with a considerable increase in the cancer risk. 30 Chronic inflammation is considered an important risk factor for cancer development, and it is thought that at least 20% of the malignancies are borne in association with it. 20
Nevertheless, the potential link between CMI and OC by means of chronic inflammation has not been studied yet. Owing to that if CMI has a specific action site, it is possible to analyze the biomolecular markers using the so-called split-mouth design. In this model, one sample is taken from the injury site associated with CMI and another from a contralateral clinically healthy site (without CMI). Since the Piemonte et al. criteria for CMI allows an objective assessment as to whether there is a CMI lesion, this offers a simple and secure method to select the sample site. Furthermore, split-mouth provides an exceptional adjustment of the confounding variables, such as tobacco, alcohol, and even individual traits. Overall, this research approach could be useful in the study of molecular markers to explain the relationship between CMI and OC.
Coherence
A given cause-and-effect relationship should not contradict present fundamental knowledge and disease biology. Nevertheless, the absence of such knowledge would not be indicative of a noncausal explanation, since this criterion—same as biological plausibility—is determined by current knowledge and the subjectivity of the researcher. 13
Since CMI is an understudied condition, the limitations of its association with OC originate more from debates with colleagues than from actual evidence, and from those we have drawn the following:
One is regarding CMI as a consequence and not a cause of the tumor growth. Even though the evidence that supports a causal relationship between CMI and OC is limited, indeed much more limited is the evidence supporting the CMI as a consequence of the tumor growth. As a matter of fact, with the exception of the study by Piemonte et al., there is no literature assessing tumor size with CMI. 9 In consequence, this notion is based on bias instead of facts.
Another shortfall is the lack of statistical association between OC and the number of defective or fractured teeth, a fairly common situation in many populations. Even though there is evidence to support this claim, it disregards the dynamic of the CMI lesions. As stated before, a high percentage of the CMI lesions requires a functional factor, so that the teeth or prosthetic factor can injure the oral mucosa repeatedly and persistently. 15 Additionally, it does not matter having many fractured teeth, because only one could be enough to generate a CMI lesion (see the “Biological gradient” section).
Albeit scarcely described in the literature, CMI is a relatively common condition. In one study, CMI was found in more than 30% of the control group of patients. 9 Given its high occurrence, it could be argued that if CMI is a risk factor for oral malignancies, then the OC incidence should be immensely high. Whereas it is accepted that tobacco and alcohol both contribute in the OC multifactorial model, the rejection of CMI as a risk factor is based on a unicausal specificity concept. If we apply to alcohol and tobacco consumption the same specificity criteria, none of them should be accepted as an OC cause, given that those factors could not substantiate all of the oral malignancies. If CMI is to be considered as a risk factor, by no means that implies that other known factors are dismissed, only that all of them should be included in a multifactorial model.
Analogy
When one causal agent is known, the standards of evidence are lowered for a second causal agent that is similar in some way. 7 If the effects for a certain factor are known, we can expect that exposure to similar factors would produce similar effects. According to Bradford Hill, the only limit of this criterion is the imagination of the investigator. 6 Also, similar to biological plausibility and coherence, it depends on the available knowledge.
The use of this criterion has probably led to many studies about OC risk associated with tobacco, when in the middle of the 20th century the relationship between tobacco and lung cancer was recognized. 31 Even though those studies found a strong statistical association, they were initially not adjusted. 32 Other risk factors analyzed more recently, such as diet, 33 HPV, 34 tooth and periodontal disease, 35 symbolize factors that have consistency. They are considered as probable and even as likely OC factor risks. All those factors were subject to exhaustive multivariate analysis, whereas tobacco and alcohol were infrequently studied adjusting them to other statistically significant factors, except age and gender. 32 This shows a marked difference between the requisites demanded for factors such as CMI in relation to others.
Analogy and Biological plausibility criteria were probably accepted in early-stage studies dealing with causes of OC, but in light of the current knowledge, they may need to be reassessed. Especially, keeping in mind that the oral mucosa is in a unique situation, being exposed to hard tissues like teeth or prosthetic devices in a continuous fashion. Within the suggested biological explanations for the relationship between CMI and OC, we can briefly mention a few.
Chronic inflammation is now being associated with many cancers of epithelial origin: chronic gastritis and stomach cancer, Crohn’s disease and colon cancer, hepatitis and liver cancer. 30 CMI, as it could be observed in CTU biopsies, generates a localized and persistent inflammatory reaction, so it could be suggested that through an inflammatory microenvironment, CMI lesions could increase the OC risk.
Favoring penetration of other carcinogens: In uterine cervical cancer, the mucosal micro erosions produced during coitus are considered to provide access to HPV virus, so it can reach the specific membrane receptors in epithelium basal cells. 36 If the genital mucosa can suffer HPV penetration under these conditions, it is possible to suggest that such mechanism is operative in oral mucosa too, which is exposed to far more aggressive and abrasive factors, such as teeth or dentures. We have recently shown that CMI can favour penetration of oral mucosa by HPV. 37
Experimental evidence
Causation is more likely if evidence is obtained in a randomized experiment. There is an ongoing debate about what kind of experiments Bradford Hill meant when he postulated causality criteria. Some authors believe that maybe Hill referred to population interventions where a certain causal factor was controlled. 38 Currently, there are no studies of this kind analyzing CMI and OC.
Rothman and Greenland stated that results from randomized experiments provided stronger evidence than results based on other designs. 19 Experimental studies in animal models are often necessary to provide mechanistic support for an epidemiologic observation that involves complex temporality. 7 Because of ethical reasons, experimental studies about CMI and OC are not possible in humans, so animal experimentation could be used. Animal studies allow a better adjustment of the variables, although the results are not always easily extrapolated into human beings, because of the complex interaction that multiple factors may have in a certain population. 6
Even with these restrictions, studies of chemically induced carcinogenesis with mechanical irritation of oral mucosa showed an increase in frequency, higher malignancy grade, and shorter latency period, suggesting that CMI could play a role as a promoter. 39,40
Conclusions
This review offers an in-depth analysis of the causal relationship between CMI and OC, discussing some shortcomings of current knowledge while also suggesting future directions for research, as could be seen in Table 3.
Existing limitations and future directions for research in CMI and OC.
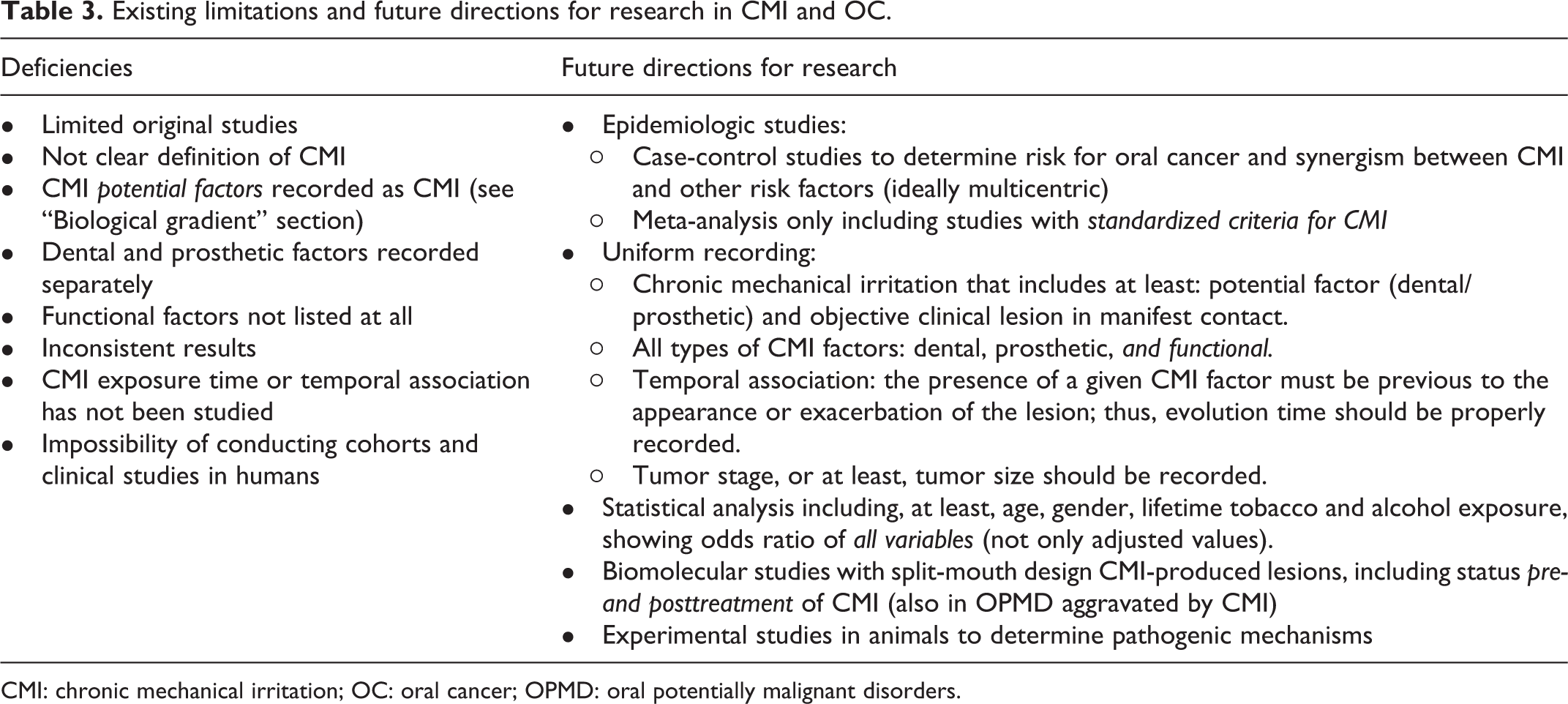
CMI: chronic mechanical irritation; OC: oral cancer; OPMD: oral potentially malignant disorders.
Despite that the level of evidence is not conclusive, it is important to emphasize that studies dealing with risk factors for OC should not be restricted only to lifestyles such as tobacco/alcohol but also consider other variables reflecting the dental condition. Furthermore, we also hope to see an increase in studies exploring the biological pathways of CMI and OC.
Finally, we strongly believe that rigorous methodological standards are required to systematize CMI research, since there is not even consensus on the terminology used to describe it. A tooth/denture could be a CMI factor if and only it indeed produces a lesion on the oral mucosa. It is also essential to assess functional factors, as they increase contact intensity and frequency. In consequence, clear methodological guidelines are needed for CMI: criteria, examples, definitions, and even a glossary of CMI terminology. We propose to explore these in a future article on methodological aspects to assess CMI.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.