
Abstract
Background:
Oral health professionals (OHPs) could have an important role in contributing to tobacco-dependence treatment of patients who visit dental clinics. How the public may perceive the role of OHPs in this capacity, however, has not been formally evaluated. The objective of this study was to assess national awareness and receptivity among Japanese in terms of the implementation of tobacco cessation counseling and treatment (TCCT) by OHPs in dental settings covered by National Health Insurance (NHI). The study participants’ awareness and knowledge on tobacco-related health disparities were also examined.
Method:
A questionnaire survey was used to assess the opinions among patients who visited hospital dental and oral and maxillofacial departments and private dental clinics (n = 27) spread across several prefectures in Japan on their acceptance if tobacco cessation services were given by dentists and dental hygienists.
Result:
Overall, 963 survey sheets were eligible for the analysis. To the inquiry on tobacco-related oral diseases (TRODs), majority were aware of tooth staining (85%) and bad breathe (80%). However, less than half of respondents were aware of oral cancer (47%) and only 32% of oral precancer. OHPs were acceptable to the majority of respondents for TCCT: ≥70 age-group (84%), ex-smokers (84%) or never smokers (81%), never drinkers (83%), and students (86%). Paradoxically, current smokers (60%) were less likely to accept OHP for TCCT. However, those willing to quit within a month (89%) were willing to accept any help from OHP than those with no decision to quit (58%) (p = 0.029).
Conclusion:
The result of this nationwide survey in Japan supported an expansion of duties of OHPs to provide TCCT to dental patients covered by NHI. Japanese patients who were willing to quit smoking were likely to accept TCCT in a dental setting, supporting the scheme for the introduction of tobacco control in dentistry.
Introduction
Oral diseases and disorders related to smoking include oral cancer and precancer, periodontal disease, dental caries, tooth loss, gingival recession, and other benign mucosal disorders as well as implant failure. 1 Cigarette smoking is a major risk factor for oral cancer, and tobacco is regarded as a group 1 carcinogen by IARC. 2 Although tobacco cessation is the most cost-effective intervention for cancer control, there have been reports that dentists are unlikely to conduct tobacco cessation intervention in their clinical practice. 3,4
Japan has ratified the World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC) in 2004. However, progress in translating the recommendations into national policy has been limited 5 due to attempts by the industry to support smokers. In the WHO report on the global tobacco epidemic 2015 6 in Japan (in 2014), 19.3% of population (aged ≥ 20: 32.2% of male and 8.2% of female) were smokers. The proportion of smokers has declined in recent years, but the prevalence is still high in the younger generation, particularly among female. The Japan’s score for implementing FCTC by MPOWER measures was far behind most countries in the world. 6 In the WHO report, under the measurements of cessation program: treatment of tobacco dependence and taxation scored higher than that of other efforts. In 2016, Ministry of Health Labour and Welfare, Japan, has launched a report entitled Smoking and Health, the so-called White Paper on Tobacco, Japan. 7 In this report, further improvements to the treatment of tobacco dependence was raised and suggested commissioning tobacco cessation in dental settings covered by the National Health Insurance (NHI). Although when administered by OHP there is no clear consensus regarding efficacy of tobacco cessation and their cost-effectiveness, this is the official statement in Japan to step into tobacco control conducted by oral health personnel.
The dentists and dental hygienists are expected to conduct appropriate tobacco cessation support and consecutive treatment as an integral part of dental treatment, particularly for those who have tobacco-related oral diseases (TRODs) and/or lifestyle-related diseases. There are few countries (Finland) where dentists regularly conduct tobacco cessation intervention for their patients as part of preventive oral care with reimbursement of the cost. 8 NHS practitioners in the UK report lack of reimbursement, lack of time and training and fears over patient response as barriers to deliver smoking cessation interventions. 9
In this regard, it is important to know if the Japanese citizens have concerns about receiving tobacco cessation advice in dental settings and whether they would accept it or not. The objective of this study was to investigate a national awareness and receptivity to tobacco cessation intervention by oral health professionals (OHPs) as well as to assess knowledge and awareness of the harmful effects of tobacco of the volunteers contributing to the survey.
Materials and methods
A questionnaire survey was self-administered to volunteering patients who visited departments of oral and maxillofacial surgery, periodontology and implantology in university hospitals or general hospitals and private dental clinics in Japan. The study was undertaken during a day to a few weeks in February 2017. The survey sheets were distributed together with a poster for tobacco cessation promotion to designated training facilities joining for an ongoing clinical trial conducted by nine academic societies in dentistry entitled Tobacco Cessation Intervention Study for Oral Diseases (TISOD) (NCT02737176). 10 The acceptance of tobacco cessation intervention by the dentists and dental hygienists was assessed by asking respondents their opinions on tobacco cessation counseling and treatment (TCCT) being performed in a dental setting (Table 1). The information on participants regarding the characteristics of smoking status, age-group, sex, alcohol consumption, and occupation were collected. Questions were included on awareness and knowledge of TROD; oral cancer/precancer and other benign disorders and tobacco-related issues; nicotine dependence, passive smoking, and coverage by NHI for TCCT in an outpatient tobacco cessation clinic. Verbal consent was obtained from all participants prior to the administration of the questionnaire. Ethical approval was obtained from a representative committee; Scientific and Ethical Committee of Oakazaki City Hospital, followed by approvals from each hospital. Overall, 27 nationwide facilities located from the north to south of Japan accepted the survey study, and in total 1009 survey sheets were collected. Of these, 46 were excluded on the grounds of being incomplete and 963 questionnaires were available for the analysis.
Questionnaire survey sheet.

Basic statistics and cross-tabulation analyses for each variable were carried out. We performed a group subanalysis by tobacco smoking status with regard to willingness to quit smoking. Statistical calculations were carried out using the statistical package, JMP version 8.0.2 for Windows (SAS Institute, Cary, North Carolina, USA). Relationship between awareness and knowledge regarding TRODs and smoking and other demographic factors were analyzed by t test or ANOVA. Acceptance of TCCT covered by NHI and conducted by OHP was assessed by chi-square. All statistical tests were two sided, and a significance level of 0.05 was used throughout.
Results
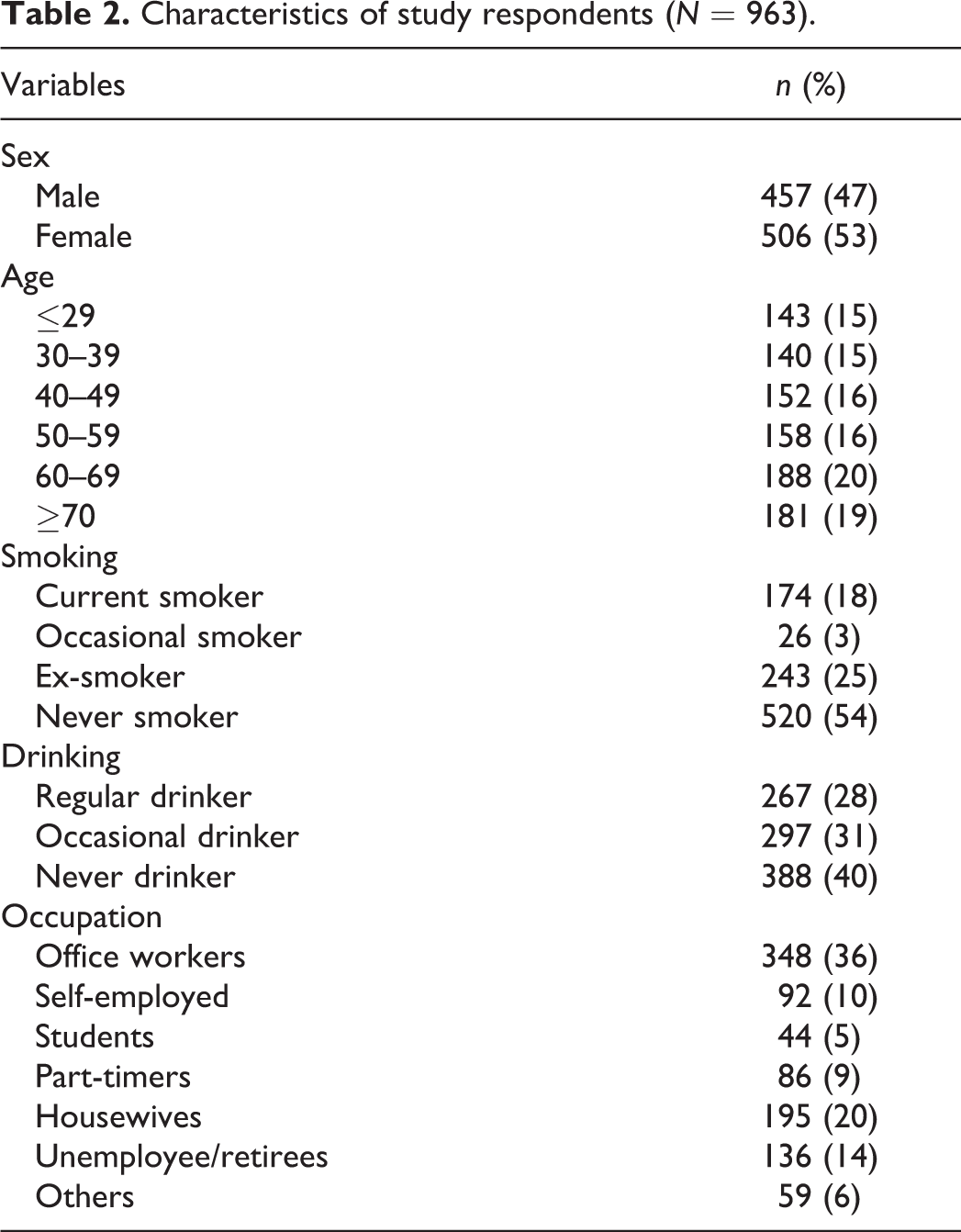
Among respondents, the 60s age-group was the most prevalent. Table 2 shows the demographics of the respondents. Gender ratio was almost the same. Among respondents, 18% were current smokers, 25% were ex-smokers, 3% were occasional smokers, and 54% had never smoked. More than half of the respondents were office workers and housewives. Table 3 lists the outcomes on awareness and knowledge questions regarding TRODs and health; awareness of nicotine dependence, passive smoking, coverage by NHI for TCCT and TCCT by OHPs. A total of 565 (59%) respondents had a regular dental checkup. Eighty-five percent of respondents said they knew that nature of tobacco habit i.e. nicotine dependence is similar to a drug dependence. Eighty-one percent of respondents had correctly answered to passive smoking. A little less than half of the respondents knew of the coverage by NHI for TCCT in an outpatient tobacco cessation clinic.
Characteristics of study respondents (N = 963).
Responses to question of awareness and knowledge questions for the nine TRODs and health.

TROD: tobacco-related oral disease; TCCT: tobacco cessation counseling and treatment; NHI: National Health Insurance; OHPs: oral health professionals.
With regard to the acceptance of TCCT given by OHPs, 78% of respondents agreed to it, and only 1% disagreed and 21% said neither. The persons who had awareness of nicotine dependence, adverse effects of passive smoking, and coverage by NHI for TCCT responded positively to the acceptance of TCCT by OHPs.
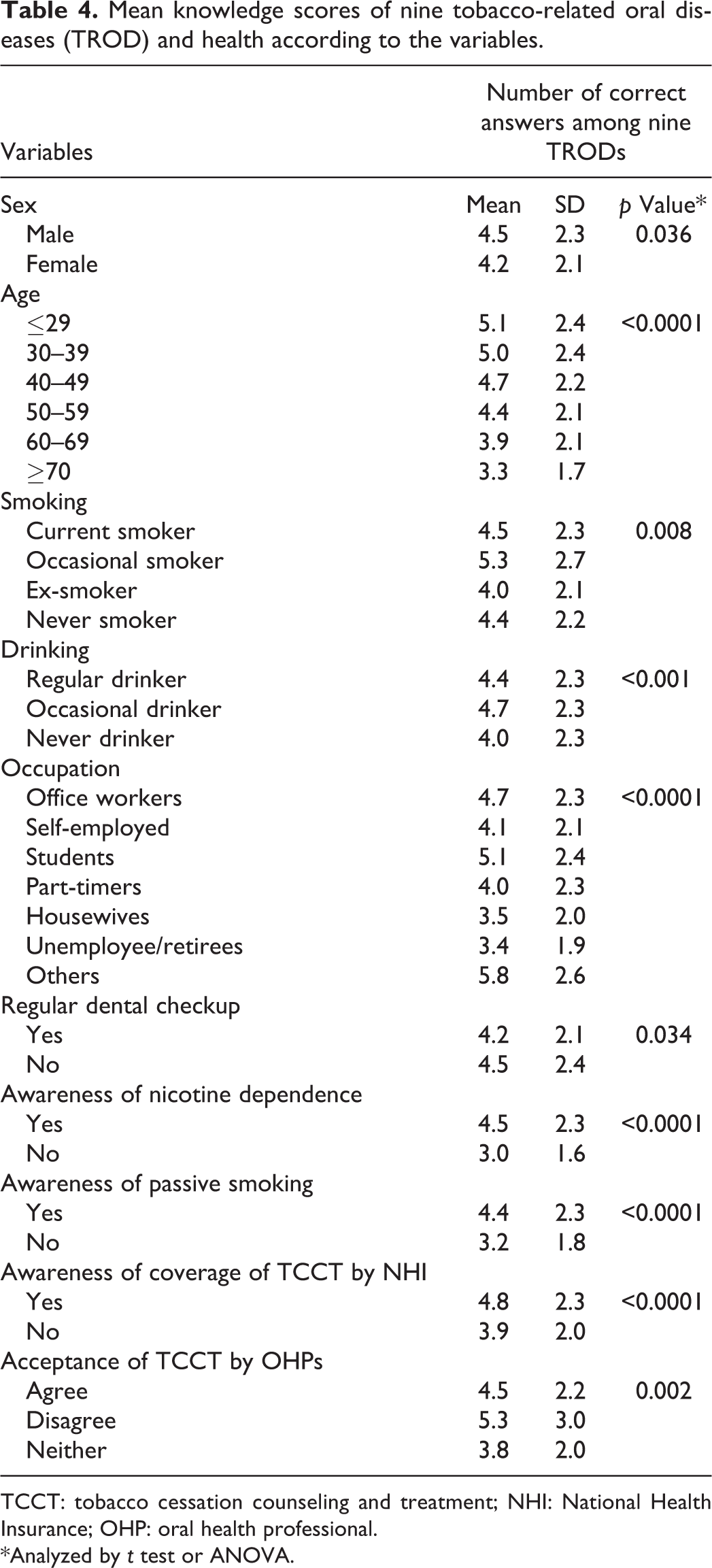
Table 4 shows the mean knowledge scores of each TROD and health by the selected variables. The mean scores out of 9 TRODs were significantly higher in male gender (4.5±2.3) (p = 0.036), ≤29 age-group (5.1 ± 2.4) (p < 0.0001), occasional smoker (5.3±2.8) (p = 0.008), occasional drinker (4.7 ± 2.3) (p < 0.001), students (5.1±2.4) and other occupations (5.8±2.6) (p < 0.0001). Awareness of nicotine dependence, adverse effects of passive smoking, and coverage of TCCT by NHI were significantly higher than those of nonawareness group. On the other hand, the awareness scores on these items by the respondents who disagreed to receiving TCCT by OHPS (5.3 + 3.0) were significantly higher than in the group agreeing to receiving TCCT by OHPs (4.5 + 2.2) (p = 0.002).
Mean knowledge scores of nine tobacco-related oral diseases (TROD) and health according to the variables.
TCCT: tobacco cessation counseling and treatment; NHI: National Health Insurance; OHP: oral health professional.
*Analyzed by t test or ANOVA.
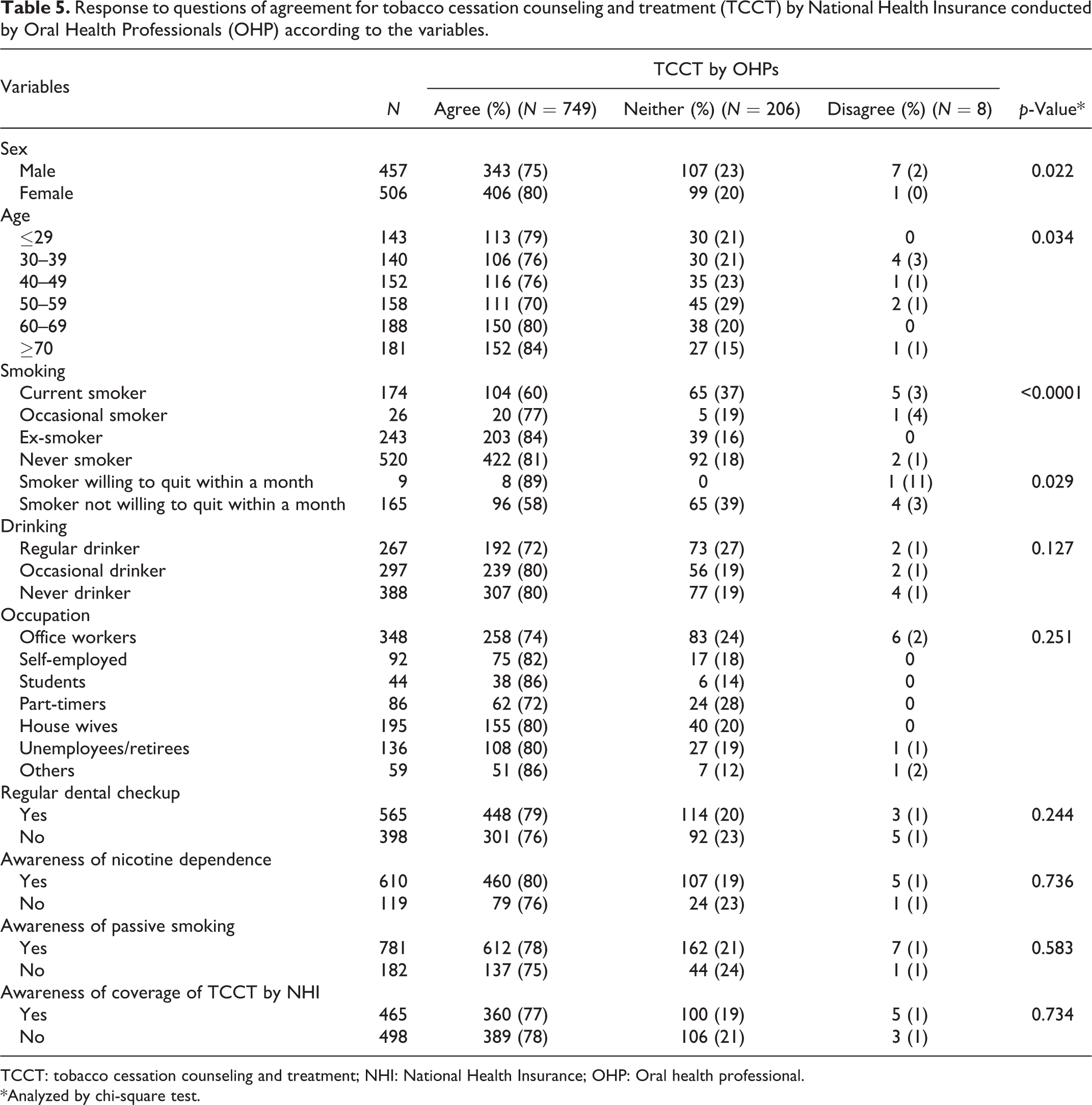
Table 5 shows the responses to the question what do you think if it is the case that the tobacco cessation treatment is implemented in dental settings?. The rates of agreement were higher in female gender (80%), ≥70 age-group (84%), ex-smoker (84%), never smokers (81%), never drinkers (83%), and students (86%).On the other hand, current smokers (60%) were less likely to accept it. However, in the subgroup analysis among current smokers, the rate was significantly higher in the group who were willing to quit within a month (89%) than those with no decision to quit smoking (58%) (p = 0.029).
Response to questions of agreement for tobacco cessation counseling and treatment (TCCT) by National Health Insurance conducted by Oral Health Professionals (OHP) according to the variables.
TCCT: tobacco cessation counseling and treatment; NHI: National Health Insurance; OHP: Oral health professional.
*Analyzed by chi-square test.
Discussion
This study was the first survey so far in Japan to investigate the public’s national awareness and consensus on tobacco cessation services by OHPs. The study was conducted as a component of an ongoing tobacco cessation intervention study. There are few studies (conducted in the United States, Australia, and India) that elucidated the agreement by patients whether dentists should provide quit assistance and services. The findings vary; 60–73% of patients expect their dentists to engage in tobacco cessation. 11 –13 In this study, we determined that the majority of participants who volunteered to complete this survey in various parts of Japan agreed that the TCCT should be conducted by OHPs and this activity should be covered by NHI. This was particularly the choice in female gender, nonsmokers and nondrinkers, elderly, and students. Current smokers being less likely to accept it appears to be a window of opportunity for those who are keen to quit soon. It should be noted that the willingness to receive TCCT by OHPs were not in line with the outcomes of the knowledge of TRODs and awareness of tobacco-related issues such as nicotine dependence, adverse effects of passive smoking, cessation treatment covered by NHI at an outpatient clinic, or having regular dental checkup. In fact, the respondents who disagreed to it had higher scores for the questions on TRODs.
Although there are only a very few countries or insurance companies that cover the cost of tobacco cessation by the dentists, a dental insurance company in the United States believed that screening and interventions for tobacco use was an appropriate part of routine care during a dental visit 14 and a promising venue for preventive screening such as for oral cancer. 15 In many European countries, health systems do not offer any compensation for physicians or dentists to provide tobacco use prevention and cessation, with the exception of patients’ payments or coverage by some insurance companies on a voluntary basis. In Finland though a model for compensation of tobacco use prevention and cessation as a part of preventive care has been available. 8 NHI in Japan cover the cost for 70% of tobacco cessation treatment by the physicians on a similar basis to other medical treatments. A Cochrane Review concluded that full financial assistance to assist interventions aimed at smokers increases the proportion of smokers who attempt to quit, use smoking cessation treatments, and succeed in quitting when compared to no financial interventions. 16 The review also revealed that comparing full coverage against partial coverage did not detect any significant effects. 16 Jannat-Khah et al. 17 in the United States analyzed factors that influence providers’ willingness to offer tobacco cessation assistance if reimbursed for this service and concluded that providers who did not offer assistance but who reported that they would change their practice patterns if sufficiently reimbursed were more likely to be in a group practice, treat patients insured through Medicaid, and have positive attitudes toward treating tobacco dependence. Medicaid enrollees are about twice as likely as the general US population to smoke tobacco: 32% of people in the program identify themselves as smokers. 18 In 2014, the New York Department of Health included coverage for smoking cessation counseling for Medicaid patients by dental practitioners. 19 An European Working Group recommended that tobacco intervention-related compensation should be made accessible to all dental professionals and be on an appropriate remuneration scale to other therapeutic interventions. 20
Tobacco use and oral diseases have a strong association. 21 Global variations in the incidence of oral cancer relate to variations in the rates and different patterns of tobacco use. 22 In this study, more than 90% of respondents were aware of at least two oral diseases caused by smoking. Hanioka et al. 23 performed a randomized clinical trial study in Japan to evaluate effectiveness in terms of the abstinence rate following smoking cessation intervention delivered by dental professionals. The authors concluded that 3-, 6-, and 12-month continuous abstinence rates in the intervention group were 51.5%, 39.4%, and 36.4%, respectively, while the rates in the nonintervention group were consistent at 13.0%. Warnakulasuriya et al. 1 concluded that there is compelling evidence to support significant benefits of tobacco use cessation with regard to various oral health outcomes. Choi et al. 24 in a prospective study of 590 newly diagnosed head and neck cancer patients found that smoking cessation, even after a cancer diagnosis, may have beneficial effects on long-term overall mortality [quitters (Hazard ratio [HR]: 2.38, 95% CI: 1.29–4.36) vs. continuing smokers (HR: 2.71, 95% CI: 1.48–4.98)]. However, the authors raised a quandary in that only half of respondents in their study answered oral cancer as a TROD and 32% for oral precancer. These figures were quite similar to our study. In this regard, it is advisable that tobacco cessation activity together with oral cancer screening should be implemented at the point of delivery of dental care. Apart from that, many smokers in Japan who were interested in quitting, particularly young women, those who regularly visited dental clinics, and most dentists believed that smoking was harmful for their patients. 25 However, the detrimental effects of smoking may not be clearly realized by dental professionals, unless the smoking status of all patients is identified. 26 Furthermore, as shown by a survey conducted in European dental schools, education opportunities for tobacco cessation should be strengthened within undergraduate dental education 27 and by continuing professional development.
There were several limitations in this study. This questionnaire was answered on a voluntary basis; therefore, it is possible that smokers were less likely to enroll on the study. Furthermore, a bias is likely in that there might be a positive outcome shown by respondents who visit the clinic regularly to maintain a good relationship with the dental staff. Even though the outcomes may not represent the opinions of the Japanese society, 86% of students and 89% of respondents who smoke regularly and willing to quit smoking within a month accepted TCCT in the dental setting. There is not enough evidence available to assess whether these interventions are cost-effective. 28,29 Further studies will be considered to assess cost-effectiveness of tobacco cessation intervention in the dental practice and to determine incentives appropriate for both patients and dentists.
The level of care to be offered under TCCT during a dental consultation under Japan’s NHI scheme needs to be determined. The evidence-based method that could be adopted in a dental practice is the 5A model that could be delivered, if necessary over repeated visits, as brief interventions. 30,31 Ramseier 32 has described a three-tier care model under basic, intermediate, and advanced care generally dependent on the amount of time spent by the practitioner on the topic. In formulating any policy to involve OHP in this new activity, and to set the level of care that could be delivered in a dental practice, it is necessary to consider the resources available and additional training needs of dentists and other OHP staff.
In conclusion, although there are yet various issues to implement TCCT by OHPs. The results of this nationwide survey support an expansion of services for TCCT in dental settings covered by NHI. Japanese citizens were likely to accept TCCT in dental settings, suggesting that there is good evidence to introduce tobacco control in dentistry, that will not only lead to improvement of oral health but general health as well. In order to promote efficiency of this service, an introduction of a policy to encourage the current smokers for attending dental clinics is a crucial matter. In this regards, community awareness education will be necessary using media. Another strategy is to combine tobacco cessation advice during opportunistic dental screening in industrial settings or within municipal periodical disease screening conducted by local dental societies. Further intervention studies are desirable to promote smokers to make regular dental visits and to receive TCCT in dental settings.
Footnotes
Acknowledgments
The authors thank Drs Teppei Tsukiyama, Yasushi Hariya, Tadaaki Sasaki, Shigeru Aoyama, Maiko Yamada, Mitsuo Goto, Takao Imai, Shohei Kasugai, Reiko Suda, Hiroshi Ito, Yorimasa Ogata, Tsuguo Sano, Yasuo Hanazawa, Nobuo Yoshinari, Hidetaka Kimura, Hideaki Hirai, Daichi Chikazu, Satoshi Takada, Keisuke Ohno, Hiroshi, Shigeto Koyama, Takahiro Oneyama, Hiroshi Kurita for conducting the questionnaire surveys, and Obayashi N and Goto Y for assisting the study. We gratefully acknowledge Prof. Saman Warnakulasuriya for his editing and useful insights.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant-in-Aid for Project Research from Japanese Association for Dental Science, No.2015D-1 and a grant from Japanese Dental Science Federation, JDSF-DSP1-2016-000-1.