
Abstract
Background:
Clinical stage and pathology grading have consistently failed to predict survival in patients diagnosed with oral squamous cell carcinoma (OSCC). There is a need to develop a grading system that could have a predictive value in assessing the prognosis of patients with OSCC. The aim was to evaluate the prognostic significance of several parameters of the modified Bryne’s malignancy grading system.
Methods:
Malignancy grading of invasive fronts of 60 OSCCs from Sri Lankan subjects was undertaken using Bryne’s criteria.
Results:
Of the five morphological features assessed at the invasive fronts of the tumours, the range of scores derived for keratinization was low, and the host response in the stromal tissue was marked compared with reported series from European countries. There were no tumours scoring a malignancy grading under 9, regarded as tumours with a ‘good prognosis’. In logistic regression analysis among patient factors, age had a positive association on survival, and among tumour factors, the malignancy grading was significantly predictive of overall survival.
Conclusions:
Bryne’s malignancy grading is predictive of overall survival in patients with OSCCs.
Introduction
Histological grading has long been used to predict clinical behaviour and the prognosis of oral squamous cell carcinomas (OSCCs). Histopathological grading of SCCs was first introduced in 1920 by Broders 1 based on the proportion of differentiated cells to undifferentiated or anaplastic cells within the entire tumour cell population and graded as highly/well, moderately, poorly differentiated and undifferentiated tumours. Broders evaluated his grading system using a number of epithelial malignancies from various body sites and recommended it for the prognostication of epithelial malignancies. 2
Several later studies, however, have revealed that the correlation between prognosis and the degree of differentiation of oral tumours as assessed by the Broders’ classification was poor. 3–5 This may arise because an individual squamous cell carcinoma will often contain a heterogeneous population of tumour cells with variations in the degree of differentiation, and thus cell populations may have different propensities for invasion and metastasis.
Other malignancy grading systems were developed later for evaluating the prognosis and the behaviour of OSCC. These included assessing not only the tumour cell population but also the histological relationship of the neoplasm to the host tissue. 6–8 The reported prognostic significance of parameters used in these systems has, however, varied from one study to the other. 4,5,9–13 Bryne et al. 14 modified the Anneroth grading system, hypothesizing that the morphological features within the invasive fronts are important in prediction of a tumour’s clinical behaviour and prognosis. His hypothesis was that the tumour cells at the invasive fronts of the tumour are likely to be those which metastasize, so that their features are likely to be more predictive than those in the bulk of the tumour. Based on various molecular features, later studies also highlighted that the exclusion of central and superficial parts of tumours would increase the prognostic power of any grading system as these latter areas did not represent the metastasizing phenotype. 15 , 16 The modified malignancy grading system of Bryne et al. graded only the most anaplastic areas at the invasive fronts of the tumours. 14,15
Bryne’s malignancy grading system was subsequently applied to grade and prognosticate OSCC in several western laboratories. 16–19 But to our knowledge so far, it has not been applied to OSCC from any of the high incident countries in South Asia where these neoplasms characteristically arise within long-standing white or red mucosal lesions associated with betel quid or oral smokeless tobacco and run a more indolent course than most oral carcinomas in the West. 20 The aim of the present study was to evaluate the prognostic significance of several parameters of the modified Bryne’s malignancy grading on a cohort of South Asian OSCCs and to identify any challenges pertaining to the application of this grading system.
Methods
Sample
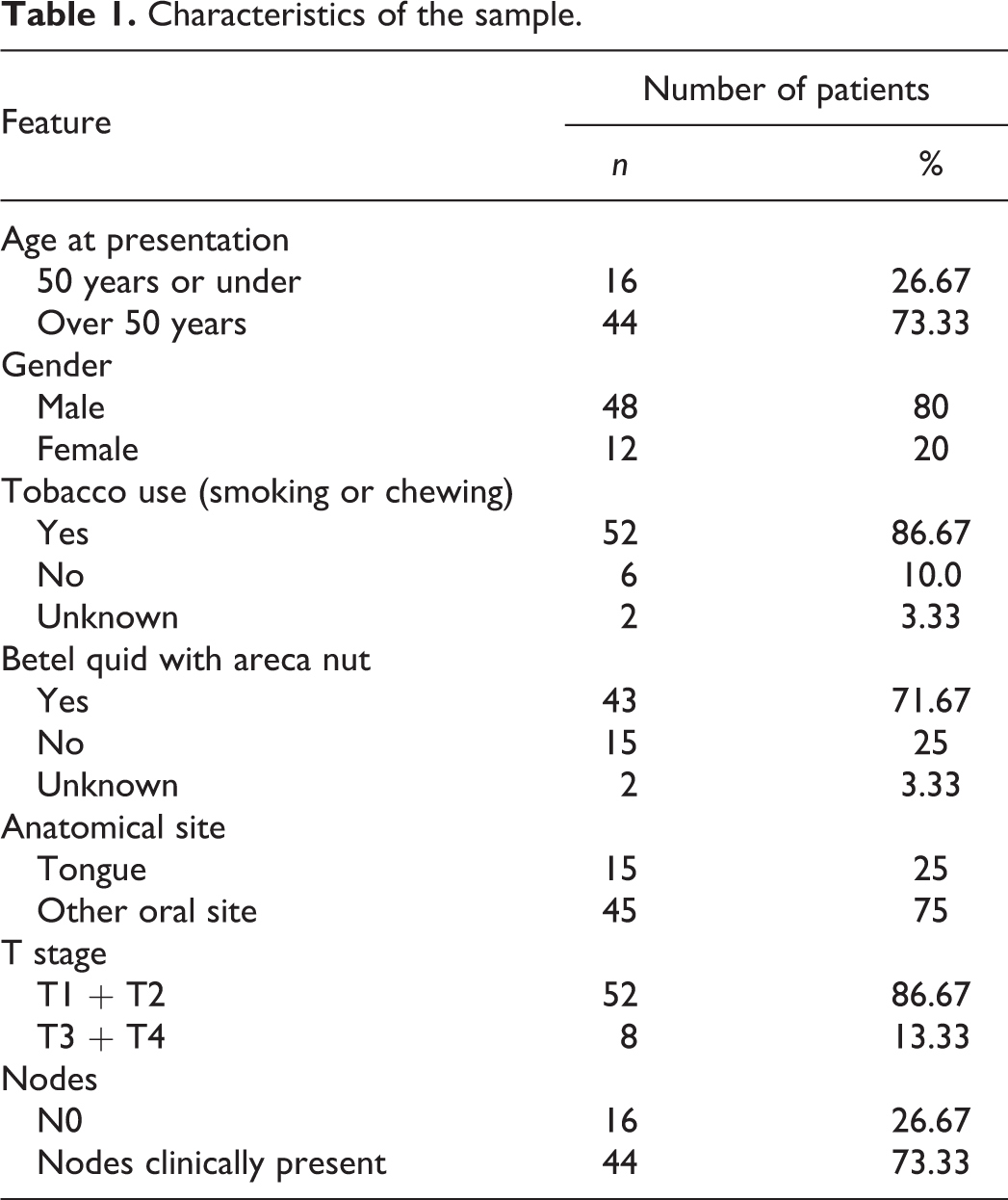
The pathology material for this study was selected from two diagnostic histopathology laboratories in Sri Lanka. Of 305 initial OSCC biopsies received during 1996–1997, diagnostic reports, availability of archival paraffin blocks and case records were reviewed. The case histories were transcribed from patient’s individual clinical records. One hundred and five cases were excluded due to missing or incomplete information. Six-micrometre sections were cut on a rotary microtome from 200 selected tumours, and haematoxylin and eosin (H&E)-stained sections were examined. The tumours that had deep invasive fronts in the cut sections were selected. Sixty cases fulfilled these criteria and were included in the current study. All 60 were primary OSCCs, 16 with pathologically confirmed regional lymph node metastasis. There were 48 males and 12 females and the mean age of the patients was 59.07 ± 11.87 years (Table 1). The study material included both tongue and other intra-oral SCCs.
Characteristics of the sample.
Malignancy grading
Histopathological malignancy grading was performed on 6-μm H&E-stained sections according to the criteria described by Bryne et al. 14,15 with minimal modification. The grading system consists of five light microscopic morphological parameters (Table 2):
degree of keratinization,
extent of nuclear pleomorphism,
number of mitosis per high power microscopic field,
pattern of invasion (POI) and
plasma-lymphocytic cell infiltration in the stroma.
Modified Bryne’s malignancy grading system used in the present study.

POI: pattern of invasion.
aPer high power field.
Only the most anaplastic fields located at the invasive front of the tumours were graded – using at least three fields from each tumour. Each of the morphological parameters was scored on an ordinal scale from 1 to 4 (Table 2). The malignancy grade of each tumour was calculated by adding the five scores for each location and dividing by three. Modifications made to improve the grading system without disturbing its structure included scoring pleomorphism (instead of polymorphism as stated by Bryne) and taking only the severity but not the extent of the pleomorphism. Except for these two minor changes, all the other morphological criteria were used as described by Bryne et al. 14,15
The grader (UD) was trained on a separate set of 15 OSCC sections until the intra-observer and inter-observer agreement (against two other experienced pathologists) reached a κ value of not less than 0.6 (data not shown). Criteria were set for each grade which the scorer often referred to while assigning a score.
Statistical analysis
Both the mean score for each tumour and the worst score from selected three microscopic fields were used for plotting the survival curves using the Kaplan–Meier method. The prognostic significance of selected parameters on survival was determined by stepwise forward Cox regression analysis. Tests were considered significant when the p values were less than 0.05.
Results
Twenty-nine (48.3%) patients of 60 patients had been treated with surgery alone and 19 (31.6%) were treated with both surgery and radiotherapy. Surgery together with radiotherapy and chemotherapy had been employed in 7 (11.6%), and 5 (8.3%) patients had been treated without surgical intervention: two with both radiotherapy and chemotherapy and three by radiotherapy alone.
After 5 years of follow-up, 25 (41.6%) of the 60 patients showed no evidence of recurrent disease. There were nine (15%) patients living with disease, undergoing further treatment. Twenty-four (40%) of 60 patients had died due to the disease within this follow-up period. Two patients had died due to other causes and one of these had oral cancer at the time of death.
Table 3 gives the number and percentage of tumours by the individual grades of our modified Bryne’s method. Ninety-eight percent of tumours in this sample were non-keratinized or minimally keratinized at the invasive fronts. In the case of plasma-lymphocytic infiltration, none of the tumours showed grade 4 (absence of infiltration) of these immune/inflammatory cells. The grades for the other three features, that is, nuclear pleomorphism, number of mitoses and POI in the 60 OSCCs were more uniformly distributed among scores 1–4 (Table 3).
Number and percentage of carcinomas in each grade for the five morphologic parameters scored (based on worst score).

POI: pattern of invasion.
Based on the worst malignancy grade of each tumour, Table 4 gives the number and percentage of tumours, which were gathered into Bryne’s prognostic groups. There were no tumours in the group with a malignancy grade from 5 to 8 in the present sample. All tumours were almost equally distributed in the two groups between 9 and 12 (31 tumours, 51%) and 13 and 20 (29 tumours, 49%).
Distribution of tumours according to the Bryne’s prognostic groups.

Prognostic significance of the modified Bryne’s malignancy grading
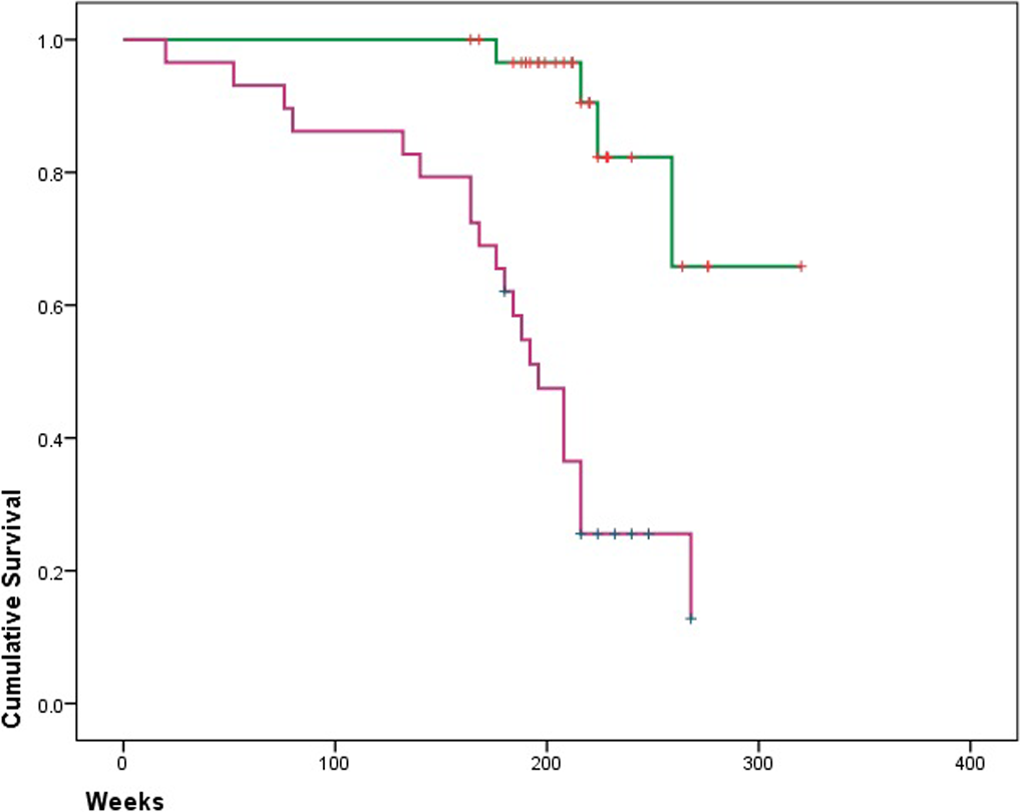
Further analysing the prognostic significance of our modified Bryne’s malignancy grading score, both mean and worst scores were stratified into two groups. The Kaplan–Meier survival curves for scores >12 or ≤ 12 recorded either as the mean score or as the worst score are illustrated in Figures 1 and 2. These illustrate that the higher scores were associated with poorer prognosis.

Kaplan–Meier survival curves showing association of mean Bryne’s scores and probability of survival in 60 OSCC patients. Green = tumours graded 12 or lower; purple: tumours graded over 12. OSCC: oral squamous cell carcinoma.
Kaplan–Meier survival curves showing association of worst Bryne’s scores and probability of survival in 60 OSCC patients. Green = tumours graded 12 or lower; purple: tumours graded over 12. OSCC: oral squamous cell carcinoma.
At 5 years following therapy, the proportion of cases surviving with mean Bryne’s scores lower or equal to 12 was 60% compared to only 20% for those with scores greater than 12. The drop in the survival curve of the patients with a mean Bryne scores greater than 12 was much steeper towards the end of the 5 years (Figure 1). The probability of survival at 5 years for patients who showed worst Bryne’s scores lower or equal to 12 was 25%, whereas the survival rate for patients who exhibited higher values for the worst Bryne’s scores was 65% (Figure 2).
The multivariate Cox regression analyses demonstrate that in our sample, both mean and worst Bryne’s scores are statistically significant prognostic parameters of OSCCs (p = 0.001) (Table 5).
Multivariate analysis, Cox’s proportional hazard test for overall survival.

Discussion
Clinical staging of OSCCs according to TNM status is routinely used for planning of treatment. The TNM classification assumes that the prognosis of small tumours without local or regional spread is better than that of larger tumours with metastasis. Many studies have reported that oral cancers of advanced stages are associated with poor prognosis. 21–35 It has, however, been noted that the rate of growth and pattern of spread of oral cancers can reflect little or no relation to the clinical stage at presentation, 36 and TNM staging alone is insufficient for optimal prognostication. 37
Broders’ conventional histopathological malignancy grading system, which is used routinely by many diagnostic laboratories for the grading of OSCCs, has been criticized due to its poor prognostic value 5,14 and its lack of reproducibility. 4 Broders’ grading of malignancy applied on 334 Italian patients with OSCC was shown to have a statistically significant relationship on histological loco-regional involvement and survival rates. The study indicated the utility of tumour differentiation in predicting the clinical course and outcome of OSCC, underscoring the need for more complex grading systems. 38 A further study in Asia compared Anneroth’s grading system against Broders on 50 SCC samples from Bangladesh. Both were predictive of lymph node metastasis but Anneroth’s grading system showed a higher level of significance. 39
Invasive front malignancy grading system introduced by Bryne et al. is reported to be of prognostic significance both by its originator and in a number of later studies. 14,15,17,18,40 Bryne’s invasive front grading has therefore been used as a research tool in number of Western studies. 18,41–43
By introducing the new grading system, Bryne et al. reported that the cellular differentiation of the whole biopsy was not of prognostic value, in contrast to the significant prognostic value of the characteristics of the cells at the invasive fronts. 14 In their primary study, they scored only 68 cases of 113 biopsies due to the fact that there was not enough tumour material from the invasive front area in the rest of the biopsies. In the present sample, only 60 OSCCs of 200 available tumours were judged to have a usable invasive front in the biopsy for scoring. Thus, the method is of limited application when the submitted diagnostic biopsy does not contain the deep invasive front required for scoring the tumour.
Using the same scoring system, Bryne et al. also introduced three prognostic groups defined by the derived total malignancy grading score (5–8, 9–12 and 13–20). They statistically confirmed the value of these groups as a predictive factor for prognosis. 14,15 Distribution of their 68 cases within the three prognostic groups is shown in Table 4. 14,15 By cross tabulating against patients’ survival data, they showed that tumours with higher malignancy gradings always ended up with a poor prognosis. 14,15 However, the distribution of the cases within the Bryne’s prognostic groups in our study was quite different from the Norwegian series. There were no tumours in the prognostic group 5–8 in the present study. This suggests that in this first study from South Asia using the Bryne’s scoring system, OSCCs with a low malignancy grade are comparatively absent in our sample. However, this finding needs to be reproduced using a larger study sample.
Odell et al. 17 studied 42 lingual squamous cell carcinomas from British subjects, which had adequate invading fronts of 106 available cases using Bryne’s approach. However, they omitted the mitotic count parameter due to difficulties in standardization. Nevertheless, the prognostic significance of the invasive front grading and the close correlation between POI and metastasis as well as any recurrence of the disease were demonstrated in this study. In comparison with the present study, one of the obvious differences in the reporting by Odell et al. was in their keratinization score: 33% of tumours scored grade 1, while only 1.6% were found with this score in the present sample. None of the tumours showed keratinization grade 2, in the present study, which comprised 33% in Odell’s study. This implies that more than 66% of the tumours in Odell’s sample had highly and/or moderately keratinized invasive fronts, whereas more than 98% of tumours in the present sample had non-keratinized and/or minimally keratinized invasive fronts. We note Odell’s results on this morphological feature are divergent to many other studies, including ours. Indeed, the invasive fronts that are used for grading in epithelial malignancies are likely to demonstrate a minimal tendency to keratinization. Therefore, the nature of the representativeness of the invasive front for assessing ‘keratinization’ in a tumour is debatable. However, such a polarized pattern of distribution in grading is unlikely to be observed with the other parameters like nuclear pleomorphism, number of mitosis and the POI. Bankfalvi and Piffko showed a correlation between morphological characteristics and the biological aggressiveness of OSCCs. 44
Various practical problems that are associated with this grading system reduce the potential use of it on a routine basis. The small-sized biopsies submitted for routine diagnostic purposes may not contain the deep invasive front of the tumour. It has been experimentally shown that the assessment of larger surgical specimens has given better prognostic indications than when examining the small diagnostic biopsy samples from the same cases. 45 This grading system is therefore successfully applicable to surgically resected specimens rather than to diagnostic biopsies. The proportion of cases that had to be excluded from available samples due to insufficient biopsy size in most of the above-mentioned studies, including the present one, was highlighted earlier. Such selection bias may well influence the results presented here. We therefore recommend that large incision biopsies, which bear sufficient tissues from the deep invasive front with a core of connective tissue, be provided whenever possible.
Issues of moderate inter-observer agreement and poor reproducibility of the method were discussed by Sawair et al. 19 We experienced during our calibration exercises that one of the important factors related to the reproducibility of the method was field selection for scoring. If all observers did not score exactly the same fields in the invasive front of the tumour, there is a possibility of deriving different scores. Field selection was very sensitive particularly in the case of recording the mitotic count. The slightest variation in the field selected for scoring could contribute to a very different mitotic count. It has been shown that the reproducibility of the total malignancy grading was improved after excluding the mitosis parameter from the grading system. 40 Quinn and Wright also reported the difficulty of standardizing the mitotic count in any recording system. 46 Bryne et al. omitted the estimation of mitotic count from grading system in their later studies due to this factor. 40,47 In our own calibration exercise, mitotic count did not appear to be difficult to standardize and in fact the κ values derived were all above or closer to 0.6, suggesting moderately good agreement. The importance of mitotic count in predicting the prognosis has been pointed out by Gillett et al. 48 We too could not find a need for exclusion of this microscopic feature when applying Bryne’s criteria.
One of the other drawbacks in the system is that there is a possibility of miscoding the respective parameters while assigning a score of 1–4. Even though Bryne’s scale always extends in an ascending order of 1–4, this discrepancy arises because the gradient of severity of individual parameters runs both in the ascending and descending orders. For example, a highly keratinized tumour is expected to be given a score of 1 and a non-keratinized tumours a score of 4. On the other hand, a tumour, which has little nuclear pleomorphism, would be scored as grade 1, while one with extreme pleomorphism gets the score of 4. There is a likely possibility of miscoding when a scoring system is used with several parameters, having a gradient of severity opposite to each other.
As there could be more than one infiltrating front for a tumour, identifying the most appropriate or the worst field without adequate scanning of all fields would be difficult. There is a chance of under scoring, if the invasive front is not properly selected. To reduce the possibility of losing the most appropriate field or the worst field of the tumour in the scoring system, we selected more than one field from several invasive fronts independently and at least three fields were used for grading. The worst out of several readings from all selected fields was taken as the worst tumour score, and we also assessed the mean score for the invasive front.
Data from previous studies support the hypothesis that several characteristics of the invasive front are of considerable value for the prediction of clinical behaviour of oral SCCs. In more recent studies, the POI has proven to be of high prognostic value. 49
Heerema et al. 49 examined the POI – one of the features of Bryne’s malignancy grading system – and reported this to be an independent prognostic factor in low-stage OSCC. However, the authors found it has a moderate reproducibility, and the contributory value compared to other prognostic histopathological factors was minimal. Kuriakose’s group also studied five POIs and reported that POI could serve as an individual prognostic marker irrespective of the histologic differentiation of tumour. 50
In a Finish study, the depth of invasion (DOI), tumour budding and worst POI (WPOI) were found to be significant prognostic markers for early stage (T1 & T2, N0 M0) tongue carcinomas. 51 The authors remarked that these parameters could be easily and rapidly analysed using the routine H&E-stained tumour sections. Tumour thickness (TT) is also a strong predictor for cervical lymph node involvement. In a meta-analysis, the optimal TT cut-off point was determined at 4 mm. 52 It should be noted that measuring DOI is not synonymous with TT. 53
The originator of the Bryne’s score has shown that this system of malignancy grading at the invasive front of the tumour is a significant prognostic factor in multivariate analysis of head and neck cancer in a Scandinavian population. 14,40,47 Several authors have independently confirmed the highly significant prognostic value of the invasive front grading for head and neck SCC from other European populations. 16–19,42
Woolgar and Scott studied 123 patients with OSCCs to evaluate the survival, metastasis and recurrence of the disease. 18 They highlighted the prognostic significance of POI that was directly correlated to the survival of the patients in the study. Statistically significant correlation between the POI and the peritumoral chronic cell infiltrate has been highlighted by Slootweg et al. in a study of 76 patients. 54 Odell et al. 17 studied 40 laryngeal squamous cell carcinomas using parameters described by Anneroth et al. 5 The area selected for scoring by them was the invasive front as defined by Bryne et al. 14,42 They demonstrated a statistically significant correlation between prognosis and the invasive front grading as well as importance of it in predicting the prognosis of the disease. Bankfalvi and Piffko 44 and Kantola et al. 55 also highlighted the importance of the assessment of invasive front in oral SCCs in evaluating the prognosis.
In this study, we assessed the prognostic value of the Bryne’s invasive front grading on OSCCs from Sri Lankan patients whose aetiology of the cancer is different from Western patients. The study showed that the invasive front grading is a significant prognostic indicator in the cohort of patients studied.
From the limited studies undertaken, it is worthwhile to speculate any differences in tumour characteristics observed by this scoring system between Western samples and this group of tumours from Sri Lanka. It was observed that aggressive tumours were more frequent among Sri Lankan OSCCs compared to Bryne’s Scandinavian series in terms of malignancy grading. Almost all the Sri Lankans tumours came under the prognostic groups 9–12 or 13–20, which represent moderate to highly aggressive entities. Even though not equally distributed, Bryne’s samples consisted of OSCCs pertaining to all prognostic groups. The keratinization of cells at the invasive fronts was a common finding in Odell’s study 17 using Western samples compared with the Sri Lankan OSCCs in which keratinization of tumour cells at the invasive front was very rare or completely absent. Tumours without sub-epithelial chronic cell infiltration were absent from Sri Lankan samples, whereas this is not uncommon in Western samples. However, as there are no other reported studies on Bryne’s malignancy grading on Asian carcinomas, more detailed studies are needed to confirm these findings. More recently, other grading systems have been introduced for risk stratification of OSCC, and these need to be tested in further studies. 56,57
Conclusions
Bryne’s malignancy grading system can be performed using adequate sized diagnostic biopsies or resection sections received in any pathology laboratory. No special staining and/or techniques are required, as the grading is performed on routine H&E sections. Bryne’s invasive front grading is therefore economical and a less time-consuming technique compared with currently researched molecular biology techniques. The only requirement is a proper standardization of observers through training and calibration of pathologists undertaking the scoring to reduce the inter-observer and intra-observer variability in order to enhance the reproducibility of the method.
Footnotes
Acknowledgements
I wish to thank Professors Newell W. Johnson and Saman Warnakulasuriya for their expertise and calibrating me in grading tumour samples in their laboratory. Dr Derek Cooper assisted in statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.