
Abstract
Peer learning supports bachelor nursing students’ professional development, yet its usefulness across clinical contexts and educational levels remains underexplored. This cross-sectional survey study used quantitative and qualitative data (n = 1264; 50.3% response rate) collected between May 2020 and June 2022 to examine bachelor nursing students’ perceptions of their learning environment and professional development, during different clinical placements and educational levels, when supervised within peer learning. Reporting followed STROBE and COREQ guidelines. Most students reported that peer learning significantly enhanced learning (67.7%), professional development (65.7%), autonomy (59.1%) and understanding of the nursing process (57.5%). Students favoured regular changes of peers. Peer learning environments were scored significantly higher than traditional one-to-one supervision. However, peer learning benefits appear to decline in later semesters and at certain clinical settings. Structured reflection based on the profession's role and function, as well as context-sensitive implementation, may enhance the relevance of peer learning for more advanced students.
Keywords
Introduction
The global imbalance between the supply of and the demand for healthcare professionals presents a significant challenge. 1 The need to educate more healthcare professionals adds a further strain to already overburdened healthcare systems, as well as to higher education institutions. 2 Teaching and learning strategies must therefore support the transition from bachelor nursing student (BNS) to professional nurse, ensuring that theoretical knowledge is effectively linked in clinical placement. This connection is essential to help BNSs draw meaningful links between theory and practice. Whether learning occurs at the university or during clinical placements, a recent review has identified both facilitators and barriers to the transfer from theoretical knowledge into clinical practice. 3 This transition can be particularly difficult for BNSs because transforming theoretical knowledge into practical skills remains a complex process. 4
In recent decades, international review studies have demonstrated that peer learning benefits BNSs’ clinical education5–8 in terms of their academic, cognitive and social development. Peer learning contributes personal and professional growth by strengthening self-confidence, socialisation9,10 and communication skills. 6 It also promotes development of professionalism, as BNSs engage in teamwork, practice leadership 6 and take responsibility for their own learning, such as collaborating throughout all phases of the nursing process.11,12 Reflective practice and mutual feedback further encourage the construction of new knowledge. 11
Bachelor nursing students often report positive experiences due to the close involvement with patients and staff, which is also considered a prerequisite for professional development. 12 Moreover, peer learning appears to reduce anxiety,5,9 which is also beneficial for learning. From the supervisor's perspective, peer learning involves stepping back and allowing BNSs to assume greater responsibility for their own learning. 13 Overall, the learning process is influenced by the clinical placement learning environment and the pedagogical atmosphere, as well as by the relationship with the supervisor.12,14 Although previous research has highlighted several advantages of peer learning in clinical placements, few studies have explored BNSs’ perceptions of peer learning across different clinical contexts and educational levels. 15 Therefore, the present study aimed to examine bachelor nursing students’ perceptions of their learning environment and professional development, during different clinical placements and educational levels, when supervised within peer learning.
Methods
This study employed a non-experimental, cross-sectional design integrating both quantitative and qualitative approaches. Data were collected through convenience sampling using a web-based questionnaire, which was distributed to all BNS following each clinical placement over a 3-year period. Quantitative data were analysed using descriptive and inferential statistics, 16 whereas qualitative data were examined through qualitative content analysis.17,18 The researchers utilised the checklist for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 16 and the Consolidated Criteria for Reporting Qualitative Research (COREQ). 17
Setting and participants
The participants were BNSs enrolled in semesters two through six at a Swedish university. The nursing programme consists of six semesters in total. Each year, two cohorts of approximately 110 BNSs begins their studies: one cohort starts in January, and the other in August. The programme contains clinical placements in semester two (4 weeks in municipality), in semesters three and four (5 weeks each in surgical, medical and psychiatric wards), in semester five (2 weeks in primary care and five weeks in municipality health care) and in the sixth semester (6 weeks in medical or surgical wards). After every clinical placement, the BNSs complete a web-based questionnaire that evaluates their learning and acts as clinical education quality assurance. The number of BNSs in each clinical placement every semester is shown in Table 1. In total, 2511 questionnaires were sent out and 1264 responses were returned (50.3% response rate).
Number of BNSs by semester and clinical placement, spring 2020 to spring 2022.
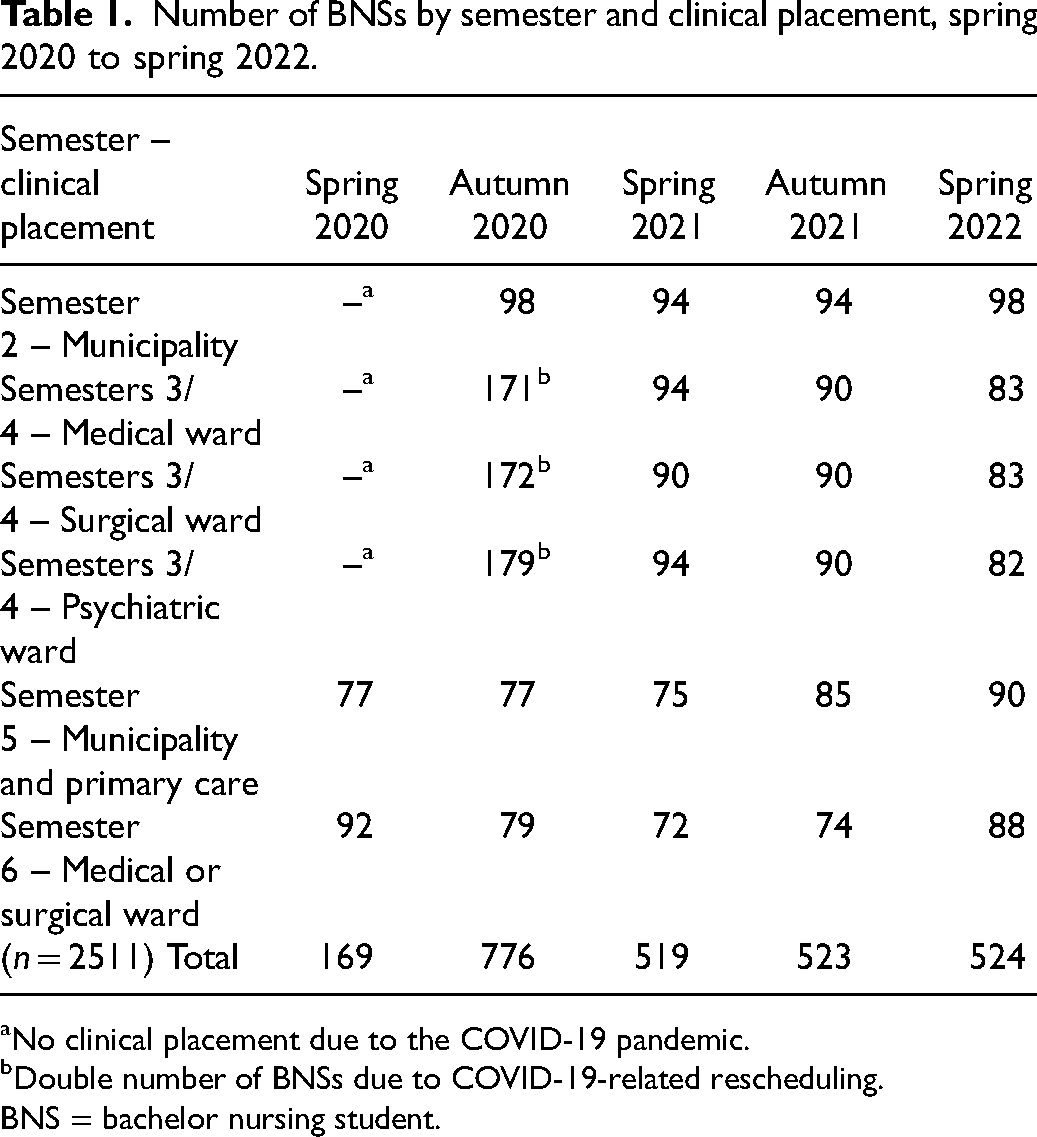
No clinical placement due to the COVID-19 pandemic.
Double number of BNSs due to COVID-19-related rescheduling.
BNS = bachelor nursing student.
Questionnaire
The questionnaire used in this study was developed by the authors, based on a review of relevant literature, our previous research, earlier evaluations of clinical practice and the national learning outcomes for the Bachelor of Nursing Science Program in Sweden. The questionnaire consisted of 23 items and six open-ended questions, focusing on BNSs’ experiences during their clinical placements. Demographic variables included age, gender, type of clinical placement, semester, peer learning supervision (yes/no), patient-focused supervision (yes/no), type of feedback from supervisors (oral, written) and frequency of feedback (daily, weekly or less frequently). Four items measured to what degree peer learning contributed to the BNS’ learning, enhanced their understanding of the nursing process, supported the development of autonomy and contributed professional development. An additional six items measured the BNS’ perceptions of the clinical placement, including the quality of the introduction, feeling safe with the staff, the quality of the learning environment, achievement of learning outcomes and satisfaction with the clinical placement. These 10 items were all answered on a four-point Likert scale, ranging from not at all 1 to a very high degree. 4 For the purposes of this study, analysis focused on the four items about peer learning, the items about feeling safe with the staff and the learning environment, and the six open-ended questions.
Due to time constraints at the onset of the study, related to the COVID-19 pandemic, extensive pilot testing of the questionnaire was not feasible. However, the web-based questionnaire was reviewed by a small group of colleagues and the program director, who provided feedback on its content and linguistic clarity. Minor linguistic revisions were made, whereas the content remained unchanged.
Data collection
Data were collected between May 2020 and June 2022. After each clinical placement, a web-based questionnaire was distributed via a link on the BNS’ learning platform. On the first page of the questionnaire, BNSs received written information about the study, including its aim and design, that participation was voluntary, and that all responses would be treated confidentially. The information also included contact details for a designated person in case of questions. All prospective participants were informed that their data would be handled only by those with authorised access. Informed consent was obtained by asking BNSs to tick a box before proceeding with the questionnaire.
Data analysis
Descriptive statistics, percent and mean ± SD were used to analyse the collected quantitative data. Analysis of variance 18 was conducted to compare the mean score of the BNSs’ (third or fourth semester) perceptions of feeling safe and having a good learning environment across three types of clinical placements: medical, surgical or psychiatric wards. An independent samples t-test was conducted to compare the means of the BNSs’ perceptions of feeling safe and of having a good learning environment between those who were supervised in peer learning and one-to-one supervision. 18 All statistical analyses used IBM, version 27 (IBM Corp., Armonk, NY, USA). p < 0.05 (two-sided) was considered statistically significant.
The qualitative data (i.e., answers from the six open-ended questions, with a total of 1256 comments, of which 746 specifically addressed perceptions of peer learning) were analysed using qualitative content analysis according to Graneheim and Lundman. 19 An inductive approach was applied to identify pattern and groupings of similarities within the data. 20 Following the steps outlined by Graneheim and Lundman, 18 meaning units were first identified from the text, condensed into codes, which were subsequently organised into categories. The written responses varied in length, ranging from single words to extended narratives composed of multiple sentences. Two of the investigators (JS and KE) thoroughly read the answers several times, and analysed the text based on meaning units. The meaning units were coded, and the investigators collaboratively created the categories. The analysis was supervised and continuously discussed, and refined in consensus with the first (IA) and last investigator (CO), ensuring analytical rigor and credibility.
Ethical considerations and data management
The study was approved by the research ethical adviser at the university (HNT 2020/302). The primary data were securely uploaded to the cloud service of the university, after which they were accessible only by authorised staff. The data will be archived and then destroyed after 10 years, per European and Swedish regulations.
Results
Bachelor nursing students from semesters two through six participated in the study. Most of the BNSs were women with a mean age of 27.2 years (range 19–54 years). Of the 1264 BNSs, 881 reporting having been supervised within a peer learning model, primarily semesters three and four, and most commonly in the medical, surgical and psychiatric care settings. Four BNSs who were supervised within peer learning did not report their semester. By contrast, BNSs who were supervised in a traditional one-to-one model were predominantly in the municipal and primary care settings during semester five (Table 2).
Number of BNSs by clinical placement context and type of supervision (peer learning vs. one-to-one).

BNS = bachelor nursing student.
Quantitative results
Among the total group of BNSs, 86.8% rated their perception of feeling safe during clinical practice as high or very high (mean ± SD = 3.40 ± 0.767). Regarding perception of the learning environment, 78.8% rated high or very high (mean ± SD = 3.22 ± 0.854). Among those supervised within peer learning, 67.7% reported that peer learning contributed to their learning to a high or very high degree and 65.7% stated that it contributed to their professional development (65.7%). Furthermore, 57.5% described that peer learning made the nursing process more visible and 59.1% perceived that it supported the development of their autonomy (Table 3).
BNSs’ perceptions of feeling safe, having a good learning environment, and the impact of peer learning on own learning, nursing process, autonomy and professional development.

Scale from 1 = “Not at all” to 4 = “To a very high degree”; higher mean indicates more positive perceptions of peer learning's impact.
BNS = bachelor nursing student.
When comparing BNSs’ perceptions of feeling safe during the BNS programme (semesters two to six), supervised within peer learning or one-to-one, no statistically significant difference was identified (p = 0.108). However, BNSs supervised within peer learning rated the learning environment significantly higher than those in one-to-one supervision (p = 0.000). Further analysis of BNSs’ in semesters three and four revealed additional statistically significant differences: those supervised within peer learning perceived a safer (p = 0.047) and better (p = 0.006) learning environment compared to BNS in one-to-one supervision (Table 4).
Differences in BNSs’ perceptions of feeling safe and learning environment by type of supervision (peer learning vs. one-to-one).

Independent-samples t-test: *p ≤ 0.05 indicates statistical significance.
BNS = bachelor nursing student.
(n = all semesters/third and fourth semester).
When comparing perceptions of feeling safe and of having a good learning environment among BNSs supervised within peer learning across three different clinical placements, a statistically significant difference was found in feeling safe between the psychiatric and surgical clinical placements (p = 0.010), with the BNSs in psychiatric placement reporting feeling less safe. Additionally, BNSs in medical placement rated learning environment as statistically significantly higher than those in psychiatric clinical placement (p = 0.000). A statistically significant differences was also found between surgical and psychiatric clinical placement regarding perceptions of the learning environment (p = 0.001) (Table 5).
Differences in third and fourth semester BNSs’ perceptions of feeling safe and learning environment by clinical placement context (supervised within peer learning).

Analysis of variance: *p ≤ 0.05 indicates statistical significance.
BNS = bachelor nursing student.
When comparing BNSs’ perceptions of feeling safe and of having a good learning environment during their sixth and last semester, no statistically significant differences were observed related to feeling safe (p = 0.690) or having a good learning environment (p = 0.306) between BNSs supervised within peer learning and those supervised one-to-one.
Qualitative results
The responses to the open-ended questions related to BNSs’ perceptions of peer learning can be summarised into three categories: “Being two brings synergies”, “At the expense of own learning and development” and “The planning and organisation are crucial”.
Being two brings synergies
The BNSs expressed that peer learning catalyses synergies; for example, sharing responsibility for patient care encouraged discussions on how to organise and prioritise the care, which in turn deepened their understanding. The BNSs described that “being two” meant that always having someone to share thoughts and emotions with, to reflect on clinical situations, and to receive support from without necessarily involving the supervisor. Peer learning was perceived to create favorable conditions for learning because BNSs felt more confident when working together. This was especially important when one of them felt uncertain or insecure. As one BNS expressed it, “The opportunity to discuss issues with peer when the supervisor does not have time leads to increased independence”.
At the expense of own learning and development
Some of the BNSs expressed that peer learning could impede their individual learning and professional development. This was particularly evident in situations where differences in knowledge levels or competition between peers emerged. In some cases, BNSs described how peers competed to perform as many patient-related tasks as possible, which sometimes led to unequal learning opportunities. Sharing practical tasks was often perceived as limiting because it reduced the number of hands-on experiences for each BNS. Observing a peer, rather than actively participating, was also described as less beneficial for professional development. As one BNS expressed, “It's harder to practice if there are two of you. You do not learn by just standing and watching the other person do it. You develop more if you get the chance to do practical skills several times”.
When a BNS perceived that there were large differences in levels of knowledge, one had to take a step back and let the other peer practice more. This became more obvious when one BNS had previous experience from working in health care; the more experienced BNS often assumed a role similar to that of a second supervisor. This imbalance was perceived as limiting opportunities for equal participation and growth. BNSs also emphasised that effective communication and collaboration within the peer group were essential; when these aspects were lacking, their professional development could be adversely affected.
BNSs in their sixth and final semester perceived that being supervised through peer learning could negatively affect their professional development. Sharing responsibility for a group of patients with a peer was perceived as limiting opportunities to independently plan, prioritise and manage nursing care. Several BNSs emphasised that taking personal responsibility for patient care was essential for developing autonomy and preparing for the role of a registered nurse. For some, this was best achieved through one-to-one supervision.
The planning and organisation are crucial
BNSs highlighted that the effectiveness of peer learning was strongly influenced by how it was planned and organised. They emphasised the need for structured supervision, including pre-planned peer constellations and regular changes of peers. Such planning was seen as essential for promoting varied collaboration, exposing BNSs to different perspectives, and preventing potential long-term negative effects on learning and professional development. One BNS expressed it as: “For example, it should be a requirement that you change peers every 2 weeks. There is a risk that you end up with a person who, instead of promoting learning with reflections, inhibits your learning in various way”.
Depending on level of education, the BNSs expressed that being supervised with peer learning contributed differently to learning and professional development. Some BNS described peer learning particularly beneficial in earlier semesters, whereas others appreciated it more in the later clinical placements. However, some BNSs expressed that in the sixth and final semester, peer learning should be limited to the initial weeks of clinical placement, after which one-to-one supervision was preferred. Others suggested a blended model, alternating between peer learning and one-to-one supervision. One-to-one supervision was seen as offering greater opportunities for independence, self-reflection, and the ability to prioritise the day and tasks on their own. One BNS commented that it is “Nice to sometimes feel that ‘I can’ instead of ‘we can’”.
Discussion
The present study aimed to examine bachelor nursing students’ perceptions of their learning environment and professional development, during different clinical placements and educational levels, when supervised within peer learning. The results showed that a majority of the BNSs, regardless of semester, experienced educational benefits and perceived that peer learning fostered synergies that supported their development. Overall, the BNSs in semesters three and four responded that being supervised within peer learning made them feeling safer in a surgical context than in a psychiatric context. The learning environment was perceived as more positive in peer learning than in traditional one-to-one supervision. However, in the sixth and final semester, BNS did not perceive any differences in feeling safer or quality of learning environment when being supervised within peer learning. Importantly, BNSs emphasised that the planning and organisation of peer learning were crucial; otherwise, peer learning could hinder rather than support induvial learning and development.
The BNSs in the present study perceived that peer learning enhanced their professional development, provided it was well-planned and organised. This aligns with previous research indicating that peer learning fosters professional competence and independence.6,15,21,22 However, the findings suggest that peer learning has certain prerequisites, particularly the need for careful planning and structure, without which learning and professional growth may be compromised. BNSs also favoured regular peer changes to encourage collaborative variety, gain exposure to diverse perspectives, and avoid potential long-term negative impacts on learning and professional development. Some BNSs also reported feeling uncomfortable or pressured to defer to their peer, underscoring the importance of regularly rotating peer partners. According to Jassim et al. 21 and Markowski et al., 5 effective planning by both nursing students and staff is essential for successful peer learning.
The findings showed that BNSs generally perceived peer learning as beneficial for their professional development, particularly in semesters three and four. This aligns with the study by Ädel et al., 23 where nursing students in semester two reported increased self-confidence and emotional support through peer learning, effects considered to be health-promoting. By contrast, perceptions in the present study were more varied in the final semester, where many nursing students expressed a preference for one-to-one supervision. This contrasts with the findings of Sandvik et al. 24 who found that BNSs, in their sixth semester, placed in home care settings, perceived peer learning, such as conducting home visits without a supervisor, as a way to strengthen their independence and self-esteem by encouraging greater responsibility. This indicates that peer learning needs to be planned and organised differently in later semesters of BNS education. Antonsen et al. 10 further support this by demonstrating that planned group reflections integrated into peer learning helped BNSs learn from one another and highlighted the value of reflection in clinical practice, potentially a prerequisite for enhancing the pedagogical strength of peer learning.
BNSs in semesters three and four reported feeling safer and experiencing a more positive learning environment when supervised through peer learning. However, in semester six, the BNSs perceived no difference in feeling safe or the learning environment, regardless of whether clinical placement included peer learning or one-to-one supervision. A notable contrast emerged between clinical contexts: psychiatric wards were perceived as less safe compared to medical and surgical wards. These findings contradict previous research indicating that peer learning in psychiatric settings can enhance learning and professional development. In those studies, students reported feeling safer when working alongside a peer, with whom they could exchange experiences and knowledge before consulting their supervisor. This was an approach that fostered teamwork as well as problem-solving skills.11,22 Similar benefits have also been reported in geriatric wards, where BNSs supervised within peer learning expressed satisfaction with the learning environment. 12
The present study also showed that some BNSs perceived peer learning as a hinderance to their learning and professional development, particularly due to the need to share tasks, which limited opportunities to practice clinical skills. Similar concerns have been reported in previous research, where nursing students described task sharing as both stressful and frustrating, 23 and noted that it could lead to competition over nursing tasks. 12 Effective peer learning requires a well-functioning peer relationship; otherwise, the exchange of knowledge may be compromised. 11 Unequal levels of knowledge between peers were also seen to contribute to feelings of insecurity and competition. In psychiatric settings, BNSs perceived that peer learning reduced their opportunities for hands-on practice, while simultaneously enabling cooperative reflection and learning. 22 This means that critical thinking and structured reflection deserve more sustained focus early in BNS education, both in pre-clinical studies and in clinical placements, because peer assessment and feedback are integral to peer learning and can significantly support BNSs’ learning and professional development.
Methodological considerations
The study was conducted partly during the COVID-19 pandemic, a period marked by extreme challenges in healthcare systems that also impacted BNSs’ clinical placements. These circumstances may have influenced the BNS students’ clinical experiences. However, peer learning was already an established pedagogical method and well-known among clinical staff prior to the pandemic, which strengthens the trustworthiness of the findings. 20
The questionnaire was developed by the investigators based on relevant literature, previous research and national learning outcomes. Although it was not psychometrically validated, parts of it had previously been used for quality assurance in clinical education, which supports face and content validity. 25 Due to time constraints during the pandemic, extensive pilot testing was not feasible. However, the questionnaire was reviewed by colleagues and the program director and minor linguistic adjustments were made. This pragmatic approach reflects a balance between methodological rigor and feasibility under exceptional circumstances.
The questionnaire was distributed after each clinical placement, allowing BNS students to respond multiple times across different clinical contexts. This design enhanced the dependability of the data by capturing a broad range of experiences over time. Anonymity was maintained throughout, which likely encouraged honest and reflective responses, contributing to the authenticity of the data. 26
A key strength of the study is the inclusion of qualitative data. The open-ended responses provided rich, contextual insights into the BNSs’ perceptions and were used to deepen the interpretation of the quantitative findings. The qualitative data were analysed using inductive content analysis, 20 and the process was conducted collaboratively by multiple investigators to enhance confirmability. Quotations from the BNSs are included to illustrate the categories and support transferability of the findings.
Conclusions
The majority of the BNSs perceived that peer learning contributed positively to their learning and professional development, enhanced their understanding of the nursing process, and supported the development of autonomy. A notable finding was the BNSs’ preference for regular changes of peers, an aspect that has received limited attention in previous research. At the same time, the clinical context, played a significant role in shaping BNSs’ experiences; for example, placements in psychiatric wards were associated with lower perceptions of safety and learning environment quality. In later semesters, BNS’ views on the benefits of peer learning became more varied, indicating a need for further pedagogical development. To ensure that peer learning remains effective across all clinical contexts and level of education, greater attention must be given to its structure and implementation. Incorporating structured reflection based on the profession's role and function, peer learning can be adjusted to better support BNS in the final stages of their education and prepare them for independent practice.
Footnotes
Acknowledgements
We express our gratitude to the bachelor nursing students who participated in this study.
Author contributions
CO was responsible for the study's design and conceptualisation. IA: methodology, formal analysis, investigation and writing the original draft; JS: methodology, formal analysis, and reviewing and editing; KE: methodology, formal analysis, and reviewing and editing; AW: methodology, formal analysis, and reviewing and editing; CO: investigations, methodology, supervision of the analysis, writing, and reviewing and editing. All authors read and approved the final version of the manuscript submitted for publication.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
The study was approved by the research ethical adviser at the university (HNT 2020/302). The primary data were securely uploaded to the cloud service of the university, after which they are accessible only by authorised staff. The data will be archived and then destroyed after 10 years, per European and Swedish regulations.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.