
Abstract
There is a lack of clinical placements for bachelor nursing students (BNS). Due to this, stringent educational models for clinical practice need to be developed. The aim was to describe bachelor nursing students’ and main preceptors’ experiences of the clinical learning environment during peer learning. This mixed method study was based on a joint project between the Karlstad University and the Region Värmland, Sweden, where peer learning was launched in two geriatric clinical education wards. A total of 23 bachelor nursing student and four main preceptors participated. The data were collected in parallel, qualitative data through focus group interviews and reflective journals, and quantitative data with the CLES + T scale between November 2017 and February 2018. A directed content analysis of all results was performed. The COREQ Checklist was used. The student–patient and the student–main preceptor relationships were important for the students’ development. The students described the educational atmosphere as comfortable and safe and that the staff were knowledgeable about them. Peer learning with close interaction between patients and all staff can create authenticity, which in turn drives the BNSs’ professional development. All staff should be involved in the supervision of the students and include them as members of the nursing team.
Introduction
Competent nurses are associated with more satisfied patients, safer care, and increased patient survival, 1 all of which in turn are associated with the mission of higher education to educate bachelor nursing students (BNS). Clinical education is an essential part of the students’ education to achieve professional nursing competence and their learning must include both practical activities and theoretical reflection, 2 which puts high demands on the clinical learning environment. This poses a challenge, for both the universities and healthcare organizations, since there is a deficit in clinical education placements in many countries due to an increased number of students and new healthcare models leading to a decreased number of hospital beds. 3 To ensure that the BNSs receive a clinical education of high quality while increasing the number of students in clinical education placements, stringent educational models need to be developed and evaluated. In this paper, we present experiences of the learning environment by incorporating two models already in use: peer learning and person-centered supervision. 4
The traditional one-to-one educational model with preceptor-directed teaching has dominated clinical education in healthcare. During recent decades, other models have been developed focusing on student learning, such as the peer learning model including collaboration, reflection, communication, self- and peer assessment, which are described as cornerstones.5,6 In nursing, peer learning can mean that two students at the same (or different) academic level, plan, carry out and evaluate nursing care together, under supervision. 7 This model places more of the responsibility to achieve a successful clinical learning on the students than on the preceptors, 6 since students are expected to actively participate as equals in reasoning about nursing and clinical learning. 8 The accumulated knowledge suggests that students in peer learning gain greater confidence and independence in learning, acquire a higher level of personal and professional skills including empathy, communication, organization, leadership, decision-making, and teamwork skills compared with students supervised along traditional lines. A meta-analysis showed that peer learning is an effective supervision model which enables students to learn collaboratively, sharing learning content, and develop clinical skills such as assessing patients as well as decreasing students’ anxiety during clinical placements. 9 Peer learning can invoke a strong sense of friendship and trust between peers 6 but there are also results showing negative outcomes of peer learning, such as a sense of competition,7,10 and fear of acquiring the wrong knowledge and the BNS not feeling safe with the peer. 7 Although peer learning has its benefits for the students, there is a need of thorough planning and education for the preceptors for a successful result.9,11
Another educational model based on person-centered care implies that the BNS follows the patients rather than the preceptor. 4 Under supervision, BNSs care for their patients, within their scope of practice, including clinical documentation and patient handover. A MScN main preceptor (MP) has an overall responsibility in cooperation with a clinical nurse lecturer (university employed). The MP is supported by a ‘daily preceptor’ in day-to-day bedside nursing, including reflection and feedback with the BNSs. The MP’s role includes bedside supervision at least once a week in accordance with the curriculum learning outcomes, as well as taking part in assessments of BNSs’ achievements. The clinical nurse lecturer is responsible for induction of new students and supporting BNSs to integrate theoretical and practical knowledge in clinical education, for example in clinical seminars, and assessing and grading the BNSs’ achievements. 4 This educational model is the model used for supervision of BNSs in the present study.
One important factor to support the BNSs’ clinical education is a good clinical learning environment, 12 which involves areas where BNSs apply theory to practice by conducting actual patient care to gain experiential knowledge about skills, attitudes, and decision-making abilities necessary to become a professional nurse. This environment includes the physical space, psychosocial and interactional factors, and teaching effectiveness of the preceptor, student engagement, and organizational culture, all of which have an impact on BNSs’ abilities to meet the desired learning outcomes. 13 In a study by Sellberg et al., 14 nursing students rated their clinical learning environment higher than medical students but lower than physiotherapy and speech language pathology students did. One measure of the clinical learning environment is the five sub-dimension Clinical Learning Environment, Supervision and Nurse Teacher scale (CLES + T) developed by Saarikoski et al., 15 which has been used throughout the world, mainly in surgical and medical hospital contexts.
To our knowledge there is no research exploring the clinical learning environment during peer learning although it is an important aspect of the BNSs’ whole experience of clinical education. Therefore, we decided to describe BNS’s and MPs’ experiences of the clinical learning environment in a project where we incorporated peer learning in the existing educational model of person-centered care in a geriatric ward in Sweden.
Methods
The study had a mixed method design to triangulate complementary results. 16 All data were collected in parallel; quantitative data were collected with the CLES + T15,17 and qualitative data were collected through focus group interviews and reflective journals and then were analyzed deductively using a directed content analysis method 18 in accordance with the predetermined sub-dimensions of the CLES + T. Finally, a synthesis of quantitative and qualitative results was presented in the five sub-dimensions. Throughout the process we followed the COnsolidated criteria for REporting Qualitative research (COREQ) Checklist. 19
Setting and participants
During late 2017 and early 2018, a joint project between Karlstad University and the Region Värmland, Sweden , was launched on two educational wards in a geriatric hospital setting using the educational model peer learning to increase the number of students. 20 Supervision on the ward follows a long established person-centered educational model (described above) 4 and for the project we also incorporated peer learning. Thus, two students as peers followed a limited number of patients supervised by a daily preceptor who in turn were supported by an overall responsible MP. Before the start of the project, all staff participated in a one-day launch to become acquainted with peer learning and the organization of the project. 20
A total of 24 BNSs were invited, both orally and in writing by the third and last author, to participate in the study in the beginning of their clinical placement. The information stated that participation was voluntary and that whether the student decided to participate or not, their grades would not be affected. Of them, 23 chose to answer a questionnaire, and 13 participated in focus groups interviews. Four MPs (two on each ward), who kept reflective journals, were also invited and chose to participate in the project. We did not ask for reasons to not participate out of privacy reasons.
Data collection
Quantitative data collection
The Swedish version of CLES + T 17 was used to measure factors important to the learning environment from the BNSs’ perspective. The CLES + T five sub-dimensions—‘Pedagogical atmosphere on the ward’, ‘Leadership style of the ward manager’, ‘Premises of nursing in the ward’, ‘Supervisory relationship’ and ‘Role of nurse teacher’—comprised 34 items. The items regarding ‘Supervisory relationship’ were, with permission from the original authors, 17 adjusted to measure the BNSs’ experience of the relationship with the MP. The scale was as follows: 1, fully disagree; 2, disagree to some extent; 3, neither agree nor disagree; 4, agree to some extent; and 5, fully agree. In this study, we decided that a median value of 4 and 5 indicated that the BNSs were satisfied with circumstances regarding the respective item. Demographics regarding age, the number of daily preceptors, the number of days with the main preceptor and earlier experience in healthcare were collected.
Qualitative data collection
Focus group interviews were used to deepen the understanding of the BNS experiences of the clinical learning environment 21 and were conducted with BNSs (N = 13) divided into two groups of eight and five students, respectively. Before starting the interviews, the moderator (first and second authors) explained the purpose of them. To ensure that all aspects of the subject were discussed, the moderator used support questions regarding positive and negative experiences and areas of improvement. An assistant moderator (last author) took notes, asked clarifying questions and summarized the discussions at the end of the interviews. 21 The interviews (with a duration of 60–70 min), which took place at the university, were recorded and transcribed in verbatim. Since the second author was experienced in the method, she guided the first and last authors throughout the data collection.
Reflective journals 22 were kept by the MPs (n = 4). They reflected upon factors of importance for the clinical learning environment, obstacles and opportunities, their actions and the interaction between the students and with other staff.
Data analysis
The quantitative data (demographics and CLES + T) were analyzed with descriptive statistics: frequencies, mean (SD), and due to the low number of participants median and range values as well, using IBM SPSS Statistics version 25.
The qualitative data were analyzed deductively according to directed content analysis. 18 First, all authors read the transcripts from interviews and reflective journals and then identified and coded data (the participants’ experiences of the learning environment during peer learning). Thereafter, data were categorized in to the five predetermined sub-dimensions of CLES + T. Finally, all findings were synthesized in the sub-dimensions to triangulate complementary results. 16 The whole process of analysis was performed in close collaboration between the researchers until consensus about the results was reached.
Ethics
The study was approved by the local ethical review board (registration no. C2017/831) and permission to conduct the study was obtained from the heads of Department of Medicine, Centralsjukhuset, Karlstad and The Institution for Health Sciences, Karlstad University, Sweden. All participants were informed about the aim of the study, voluntariness and that whether they decided to participate or not, their studies would not be affected in any way. All participants gave written informed consent. The authors who collected data were not involved in grading the students’ clinical placement.
Results
Demographics
The BNS’ mean age was 24.4 (SD = 3.7) years with an range of 21–35 years. They had been supervised by 4–12 daily preceptors (M = 7.2, SD = 2.0) and by the MPs 2–11 times (M = 6.2, SD = 2.9) during 20 days of clinical placement. None of them had earlier experience of peer learning. The MPs were aged 25–35 years and they had experience as MPs for 0.5–7 years.
Experiences about the pedagogical atmosphere on the ward
In the CLES + T, the BNSs scored high on the items about pedagogical atmosphere on the ward, with the highest median score for item nine, with an overall character, indicating that the students in general were satisfied with the learning environment (see Table 1). In the interviews, the BNSs described the educational atmosphere as comfortable and that they felt secure sooner and adapted to the ward routines more quickly because they had a peer. They found that the staff became acquainted with them faster when compared with staff in ordinary clinical education placements and the BNSs perceived them as being knowledgeable about the organization of the clinical education. A possible reason for this was described in the reflective journals by MPs. They provided the staff ahead, with information about the BNS’ names, the current learning objectives, and the students’ schedules. From an overall perspective, the MPs perceived the educational atmosphere as accommodating. One of the MPs expressed it like this: The students need to feel safe. Not only as peers but also on the ward. This can be achieved through a warm reception, showing that they are welcome, involving them in the team and being open to questions. I experience that when the students enter the work group and the work quickly, they can focus more on what they are actually here to learn. (Main preceptor 2)
Pedagogical atmosphere on the ward (CLES-T measurements a ).
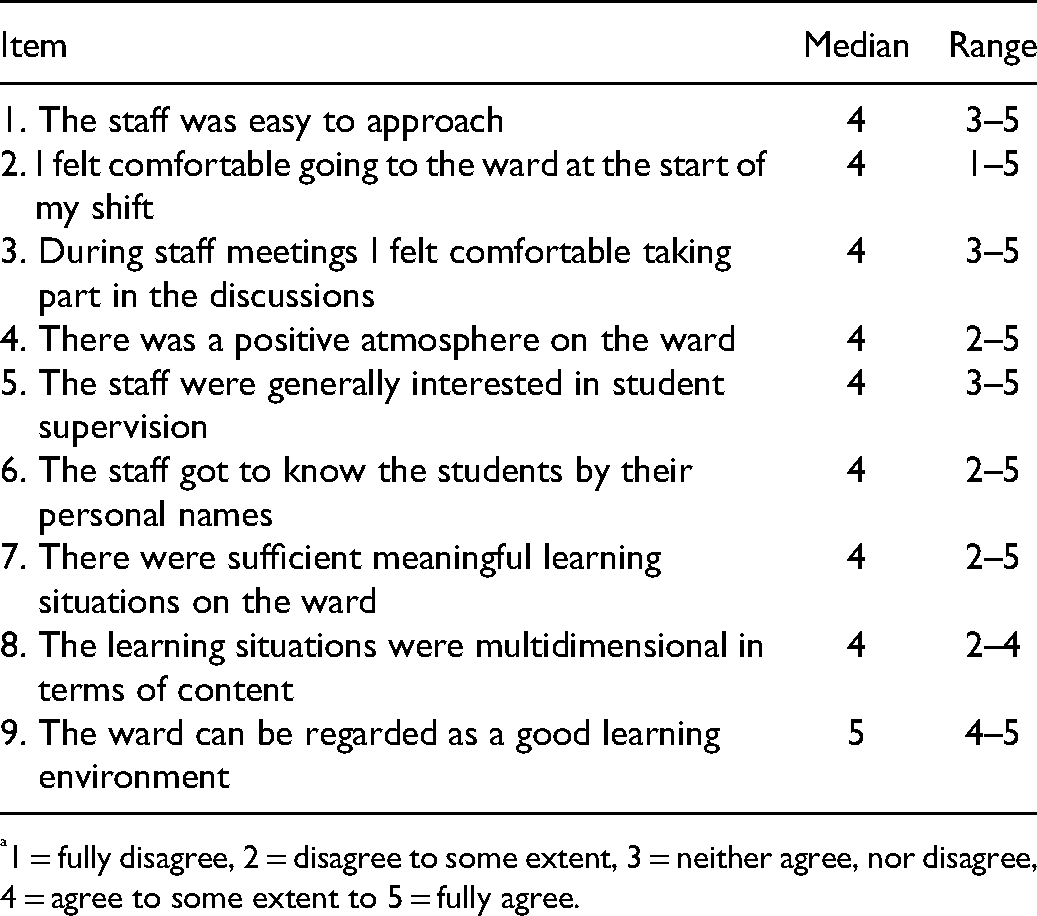
1 = fully disagree, 2 = disagree to some extent, 3 = neither agree, nor disagree, 4 = agree to some extent to 5 = fully agree.
Although the BNSs rated the item regarding staff interest in student supervision high in the CLES + T, the MPs noted that they had to clarify to the enrolled nurses that they had responsibilities towards the patients even though the BNS were appointed to care for them, since the BNS sometimes felt abandoned by the MPs. On the other hand, the MPs also expressed that the students were so comfortable with each other that they sometimes forgot to interact with the staff.
Experiences of the leadership style of the ward manager
The scores about leadership of the ward manager were the lowest (see Table 2) in the study, which corresponds with the sparse results from the interviews and journals. The BNSs conveyed that they did not interact directly with the ward managers and they perceived them as barely present, as one student expressed: Sometimes I saw her, but I did not understand that she was there every day, because sometimes she was… there, and then she was gone. I had no idea. Well, I had no need to talk to her either. (Student in focus group 1)
Leadership style of the ward manager (CLES-T measurements a ).

1 = fully disagree, 2 = disagree to some extent, 3 = neither agree, nor disagree, 4 = agree to some extent to 5 = fully agree.
The MPs described that the ward managers followed up the BNSs’ experiences of the clinical education placements with the MPs regularly and after the project was completed, and tied together the process with the entire staff group at workplace meetings.
Experiences of premises of nursing on the ward
Regarding the premises of nursing on the ward, the BNSs were satisfied (MD = 4) with a slightly lower value (MD = 3.5) about the wards nursing philosophy being clearly defined (see Table 3).
Premises of nursing on the ward (CLES-T measurements a ).

1 = fully disagree, 2 = disagree to some extent, 3 = neither agree, nor disagree, 4 = agree to some extent to 5 = fully agree.
The BNSs described nursing care as being based on the patients’ needs and preferences, which corresponds to the results from the CLES + T, that patients received individual care. The BNSs contributed to this by the extensive time the peers spent with the patients, getting to know and becoming close to them, which also facilitated the patients participating in their own care. Moreover, the BNSs described that the patients had a positive attitude towards sharing their experiences and thus be part of the students learning. One student said: [The patient] really cared that we would learn, and it was nice that he was very accommodating in that he said: ‘What fun that I get to be a part of your learning,’ he kind of gave us feedback on what we were doing and thought we were moving forward in… like… that we evolved. (Student in focus group 1)
Both the BNSs and the MPs perceived that the students had difficulties using their knowledge and skills in documenting nursing care. This was mainly because the nursing record system did not correspond to the nursing process, making it harder for the BNS to understand and use. However, the students used each other as critical peers providing feedback on the documentation.
The BNSs’ peers preferred to take their time to plan and reflect upon nursing care, which was enabled by the peer learning model. The BNS experienced that when they asked the enrolled nurses for guidance, they took over the task and performed it without involving the students. Due to the students’ inexperience and that they were expected to prioritize and perform the nursing care on their own, sometimes the patients had to wait for attendance. The MPs described that despite the wait, the patients were satisfied and felt secure with care given by the BNSs and this was also experienced by students themselves: I think that the patients also get more comfortable… because they get the same students [carers]. (Student in focus group 2)
Experiences of the supervisory relationship (between students and main preceptors)
In this dimension, the students scored the most favorably in the study (MD = 5 for all items) (see Table 4). This shows that the students were very satisfied with the relationship with the MPs, a result that also appeared clearly in the interviews. The students regarded the MPs as nursing experts and were very knowledgeable about the objective with the clinical placement. They agreed that: The main preceptors are the best I have ever met (student 1)
Supervisory relationship (between students and main preceptors) (CLES-T measurements a ).
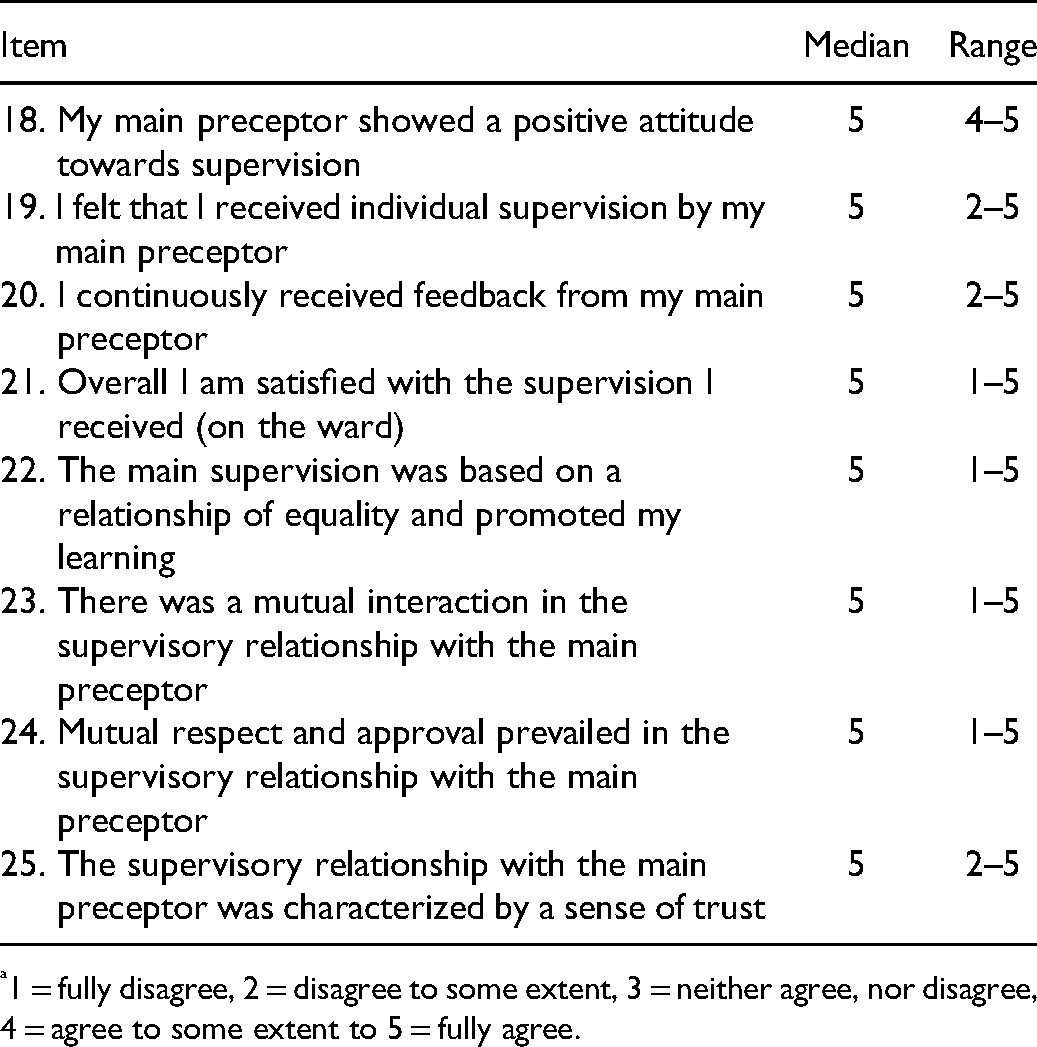
1 = fully disagree, 2 = disagree to some extent, 3 = neither agree, nor disagree, 4 = agree to some extent to 5 = fully agree.
They were so amazingly good, familiar with our learning (student 2)
They cared so much that we should learn during the time at the ward (student 3) (Students in focus group 1)
The BNSs acknowledged that it could be a challenge for the MPs to discern and meet the individual needs from two students paired in a peer group. However, they accepted that the MPs had the ability to see each student and assess the individual achievements. When there are two BNSs in a pair, then maybe it will not be as easy for a preceptor to see a clear development or a clear picture of how you are as an individual, or how you work and stuff, it may not be the same clarity, because they have to keep track of two students. I can imagine it’s problematic, but I thought our preceptor was very good, she noticed things that you did not think of yourself. She was awesome to see, I was an individual even though we were a pair. (Student in focus group 2)
The students described a continuous movement between peer interaction and interaction with the MPs permeated by trust. This was established, for example, by the BNSs receiving timely oral and written feedback and the MPs maintaining an open climate for all types of questions and ‘hovering’ in the background, being available as a back-up. BNSs perceived that the MPs also acted as gatekeepers towards the rest of the staff by protecting them from bad collegial behavior.
Experiences of the nurse teacher’s role
The quantitative results regarding the nurse teacher’s role, in this case the clinical nurse lecturer’s responsibility, for integrating theory with clinical education and collaboration with the staff showed that the BNSs disagreed that the lecturer gave educational expertise to the clinical team (MD = 2.5). Nevertheless, they were satisfied with the assessment meetings (MD = 5) and perceived that focus was on their learning needs (MD = 5) (see Table 5). In the interviews though, students expressed that they did not especially need the support from the clinical nurse lecturer on the ward as they had the support they needed from the main preceptor. We have had great main preceptors, who have really seen us and helped us very, very much, so that I have not felt any need to take help from someone else. (Student in focus group 1)
Role of nurse teacher (CLES-T measurements a ).

1 = fully disagree, 2 = disagree to some extent, 3 = neither agree, nor disagree, 4 = agree to some extent to 5 = fully agree.
On the other hand, the MPs described that they themselves sometimes needed support and guidance from the clinical nurse lecturer in solving collaboration problems among the peers. Various problems that could arise were when students in a pair were on different levels of knowledge so that one student had to have more hands-on supervision while the other needed proper challenges to develop. Students could also compete in approaching nursing tasks or feel insecure in the peer group. The MPs explained in their journals how they, together with the clinical lecturer, solved the problems, e.g. having the students taking more individual responsibilities within the peer or by letting the students change their peer.
Discussion
Overall, the BNSs’ experiences of the clinical learning environment were positive. Both students and MPs described the pedagogical environment on the wards as mainly good and accommodating. The geriatric hospital setting was perhaps an especially well-suited context for clinical education placements since the patients extensive nursing care needs and co-morbidity requires complex nursing care and provides the BNSs with ample opportunities to exercise their skills throughout the nursing process. This aligns with the results in the study by Carlson and Idvall, 23 where first-year nursing students perceived the clinical learning environment in nursing homes as positive.
The MPs experienced some challenges, which they handled on an ongoing basis, probably often without the BNSs noticing it since they did not mention this in the interviews. Based on the current findings, we stress the importance of a structured induction directed at all staff as one identified challenge was that the students sometimes felt as if they were left on their own with the patients. Staff need to be co-actors in the supervision and to make BNSs feel as one of the team, which has been shown as valuable in other studies as well. 5 Staff inductions need to emphasize the importance of short and frequent reconciliations between the BNS, the enrolled nurses, and the MPs to avoid misunderstandings and keep up the pace.
There are low CLES + T values for leadership even though the students were engaged in a project where the managers were involved. The reason for this could lie in the process of the person-centered educational model, where managers assign large parts of the responsibility for the operational work of supervision to the MPs. The effect was perhaps that the students did not notice the managers’ work, which aligns with the reasoning from Bisholt et al. 24 It suggests that managers need show interest in the students and be more visible with the work they do behind the scenes so that students get a sense of the complexity of assignments on a ward.
Earlier research on learning environments shows that a lack of support and trust from patients discourages students. 25 In this study, we found that patients came strongly in focus during peer learning and patients seemed to like the fact that they got more time with caregivers (the students), and even though these were inexperienced, they were committed to and interested in the patients. Patients became co-actors in the students’ development since the relationships between them and the students created authentic situations where students took on responsibility and followed up the patients’ nursing process with a certain degree of independence. Authenticity contributes to the development of professional identity and creates a feeling of belonging within the professional community. 26 The patient–student relationship may have encouraged the patients to take part in the decision-making relating to their own care, an essential element of person-centered care. 27
The fact that the students took on a high degree of responsibility when making sure that ‘their’ patients were taken care of properly when they themselves were on leave, shows that they crossed the threshold 28 into becoming a professional nurse and started to identify themselves as accountable nurses. An authentic learning experience from a geriatric ward can perhaps also create an interest in working in the care of elderly in the future and thus contribute to filling the need for nurses in this field of nursing. 29
The students rated the relationship with the MPs higher than the sub-dimensions of educational atmosphere and nursing care. This possibly has to do with the fact that the students are preoccupied by patient care and cannot see outside their own situation and perhaps even idolize the MPs. This may be a useful aspect of supervision since a competent nurse is a good role model for BNSs in helping them to understand all aspects of the nursing profession. 30 We also know that an experienced clinician associated with the university, for example an MP, is often preferred by the students and improves learning outcomes compared to the traditional preceptor–student model. 2
Even though the students learn as peers, the MPs were able to connect to, supervise, and assess both the pair and each individual. This is important since students can perceive that they do not have the opportunities to show their individual skills in peer learning. 7 However, it is not only the preceptors’ responsibility to give feedback. Peer assessment is an inherent aspect of peer learning, so students need the ability to give and receive constructive feedback to and from each other. 10 To recognize each other’s strengths and weaknesses improves the students’ possibilities of developing professional skills. 5
Methodological considerations
First, data were collected in 2017–2018, which can be regarded as a limitation to the study’s trustworthiness. We started the analyses of data in 2019 but due to the COVID-19 pandemic, the writing of the manuscript was interrupted and therefore delayed. However, the results of this study are still relevant since neither the BNSs’ education nor the conditions on the wards changed during this period. We acknowledge that there were rather few participants, but since the conditions of the study with peer learning in combination with patient-centered supervision are new, we considered the data important enough to report.
The CLES + T 15 is well documented in terms of reliability and validity. Although it may be that the CLES + T reflects the master–apprentice model cooperating with hospital clinical teachers, an additional dimension reflecting peer learning (e.g. items regarding cooperation between peers) could be a valuable addition to the instrument
The BNSs participated in interviews and answered the questionnaire at the end of the clinical placement, after assessments, to exclude memory bias. Focus group interviews were suitable since they take place through group interaction and the collected material can be more fully compared with individual interviews since the conversations have a different dynamic, where what is said by one is followed by another and nuanced by a third person. 21 However, we had to balance the discussions to avoid both the halo effect, that one participant is looked upon as having a higher status thus taking precedence over the others, and groupthink. 31
Since reflective journals are a method to share co-actors’ experiences, they were appropriate for collecting the MPs’ reflective experiences about the learning environment. 22
The strength of using a mixed method 16 was that the statistics showed a strong positive result while the qualitative data gave a more nuanced picture, adding some negative aspects of peer learning.
Conclusion
The clinical learning environment in this study was overall experienced as positive by the students and MPs. Peer learning with a close interaction between patients and all staff, especially with the MPs, in a geriatric ward can create authenticity, which in turn drives the BNSs’ professional development. All staff should be involved in the supervision of the students, consider all students as everyone’s students, and include them as members of the nursing team. In this study, the interaction with nurse managers seemed to be limited. We recommend that nurse managers should be visible to BNSs to show interest in their professional development.
Footnotes
Acknowledgments
The authors would like to thank all the BNSs, preceptors, and staff in the participating wards. The Region Värmland is also appreciated for cooperation and the opportunity to carry out the project.
Author contributions
Anna Josse-Eklund: conceptualization, methodology, data collection, analysis, main writer, and editor. Elisabeth Carlson: conceptualization, methodology, data collection, analysis, and review. Christina Sundin-Andersson: conceptualization, methodology, analysis, and review. Cecilia Olsson: conceptualization, methodology, data collection, analysis, writing, and editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Alice Lindström scholarship, Swedish Society of Nursing.