
Abstract
The present study aimed to describe registered nurses’ experiences of change in attitudes and self-efficacy when caring for patients with multidrug-resistant bacteria during a pandemic. This qualitative, longitudinal study used serial focus group interviews. It was conducted in a university hospital in southwestern Norway before and during the COVID-19 pandemic. In total, 62 registered nurses (RNs) participated in 12 focus group interviews at three time points between March 2020 and March 2023. We employed a diachronic analysis approach, finding four themes. The RNs experienced variable confidence in their infection prevention and control knowledge, and the constantly changing pandemic context and guidelines became obstacles to recommended behaviour. The RNs’ emotional responses when caring for patients with multidrug-resistant bacteria changed during the pandemic, and they became more confident in antibiotic stewardship. Despite these changes as a result of the pandemic, the RNs expressed consistent solution orientation, indicating a steady self-efficacy even through change.
Keywords
Introduction
Registered nurses (RNs) with competence in infection prevention and control and antibiotic stewardship are of great value to encounter the growing challenge of antimicrobial resistance. 1 For example, the prevalence of healthcare-associated infections (HAIs) often caused by multidrug-resistant bacteria (MDRD), is closely linked to nursing skills and training.1–3
Infection prevention and control (IPC), a practical, evidence-based approach to preventing avoidable infections, is a cornerstone of health system resiliency and preparedness. 4 Previous studies have suggested that RNs have adequate knowledge and positive attitudes concerning IPC guidelines and measures.5,6 However, Nasiri et al. 6 found that RNs had a poor level of practice regarding controlling HAIs. Lutze et al. 7 found that RNs’ understanding of and belief in hand hygiene as a measure to reduce the risk of transmission was associated with both self-efficacy and behavioural intentions. On the other hand, studies have suggested that RNs lack an understanding of the theory behind antimicrobial resistance and multi-drug resistant bacteria (MDRB). 8 Based on the findings of Lutze et al. 7 , a lack of understanding of antimicrobial resistance can indicate low self-efficacy and negative behavioural intentions towards preventive measures.
To care for patients with MDRB as a RNs entails seeing the patient as a whole and unique person while working under transmission-based precautions, including isolation, as a result of patients’ carrierships or infections with MDRB. 9 When caring for patients with MDRB, knowledge of and skills in both IPC and antibiotic stewardship are important. Antibiotic stewardship is defined as a set of coordinated, multidisciplinary interventions that aim to optimise the use of antimicrobial medicines in human health.10,11 Although RNs are uniquely positioned to positively impact antibiotic use and thus should be an integral part of antibiotic stewardship, 7 studies have shown the opposite7,12 Lacking competence has been reported as a prominent barrier to RNs participating in antibiotic stewardship-related behaviour, along with unclear descriptions of the role that RNs should take.10,12 Still, RNs have been found to agree that they have a responsibility to contribute to correct antibiotic use. 13
According to Nagahvi et al., 14 deaths from MDRB increased by over 80% for adults aged over 70 years from 1990 to 2021. This, together with the aforementioned forecast for 2050, indicates a high number of patients admitted to hospitals colonised with or infectioned by MDRB. Patients carrying MDRB are often isolated in a single room when admitted to hospital to prevent transmission. 8 Consequently, nursing tasks when caring for patients isolated as a result of MDRB are time-consuming and lead to additional workload and work-related stress for the nursing workforce. 15 High self-efficacy has been found to have a mediating effect on stress in RNs.16,17
The present study is based on the tripartite model of attitudes of Breckler 18 and Banduras' concept of self-efficacy. 19 Attitude comprises a knowledge component, a behavioural component and an emotional component. Along with self-efficacy, attitude plays a crucial role when aiming to understand RNs’ preventive behaviour. Despite the rising prevalence of antimicrobial resistance in society and patients colonised with MDRB in healthcare institutions, to our knowledge, no studies have qualitatively and longitudinally explored changes over time in RNs’ attitudes and self-efficacy when caring for patients with MDRB.
During the study period, the COVID-19 pandemic has been a major influential factor in healthcare institutions 4 For example, the pandemic represented a tremendous challenge to the work of hospital RNs worldwide and amplified issues concerning RNs’ roles in IPC and antibiotic stewardship. 20 Therefore, the pandemic context in which this study was conducted plays a pivotal role in the understanding of the data material and is thus described in the methods section. The study aimed to explore hospital RNs’ experiences of change in attitudes and self-efficacy when caring for patients with MDRB before and during the COVID-19 pandemic.
Methods
A qualitative, longitudinal research design using serial focus group interviews was applied. This study design is particularly useful for investigating change over time and collecting in-depth qualitative data. 21 Serial focus groups are defined as “a research design wherein the same groups are reconvened multiple times over an extended period, periodically revisiting the same focal issue through interactive discussions”. 22 Because we aimed to describe the change in the attitudes and self-efficacy of hospital RNs, focus group interviews were a useful method of collecting longitudinal data. The consolidated criteria for reporting qualitative research (COREQ) were followed to evaluate the quality of qualitative methods and reporting. 23
Context and study setting
The study was conducted in a university hospital in southwestern Norway before and during the COVID-19 pandemic (March 2020 to March 2023). The COVID-19 pandemic differed in severity from country to country, and Norway had low numbers of detected cases compared to other countries in the early phases of the pandemic. 24 Nevertheless, several extraordinary IPC measures were implemented in Norwegian hospitals to combat the pandemic, such as digital classes in infection prevention and increased frequency of visits from the Department of Infection Prevention and Control. 24
Norway is a country with a low prevalence of MDRB. 14 No significant changes in the numbers of admitted patients as a result of MDRB were observed in the current hospital during the study period. Furthermore, evidence shows that high-income countries reduced the use of antibiotics in 2020. This trend has also been found in national numbers.25–27
Participants and recriutment
RNs in clinical practice on five surgical wards and two oncology and haematology wards were invited to participate in the study. The focus group sample was drawn from the participating wards by use of convenience sampling. 28 Four RNs from each of the seven wards were invited to participate in one of the four semi-structured focus-group interviews at each of the three time points. The invitation to participate was distributed by the ward managers, who forwarded the invitation to RNs who met the eligibility criteria, as presented in Table 1. The RNs who agreed to participate gave their informed and written consent to the researcher before the interview.
Inclusion and exclusion criteria.

Data collection
We conducted three rounds of interviews: in March 2020 (T1), March 2021 (T2) and March 2023 (T3) (Figure 1). In each round, we performed four focus group interviews convenient meeting space at the hospital. The interview started with the participants answering a short survey to map demographic characteristics. The interview guide was developed by the current investigators, based on Breckler's 18 conceptualisation of attitudes and Banduras's 19 self-efficacy theory.
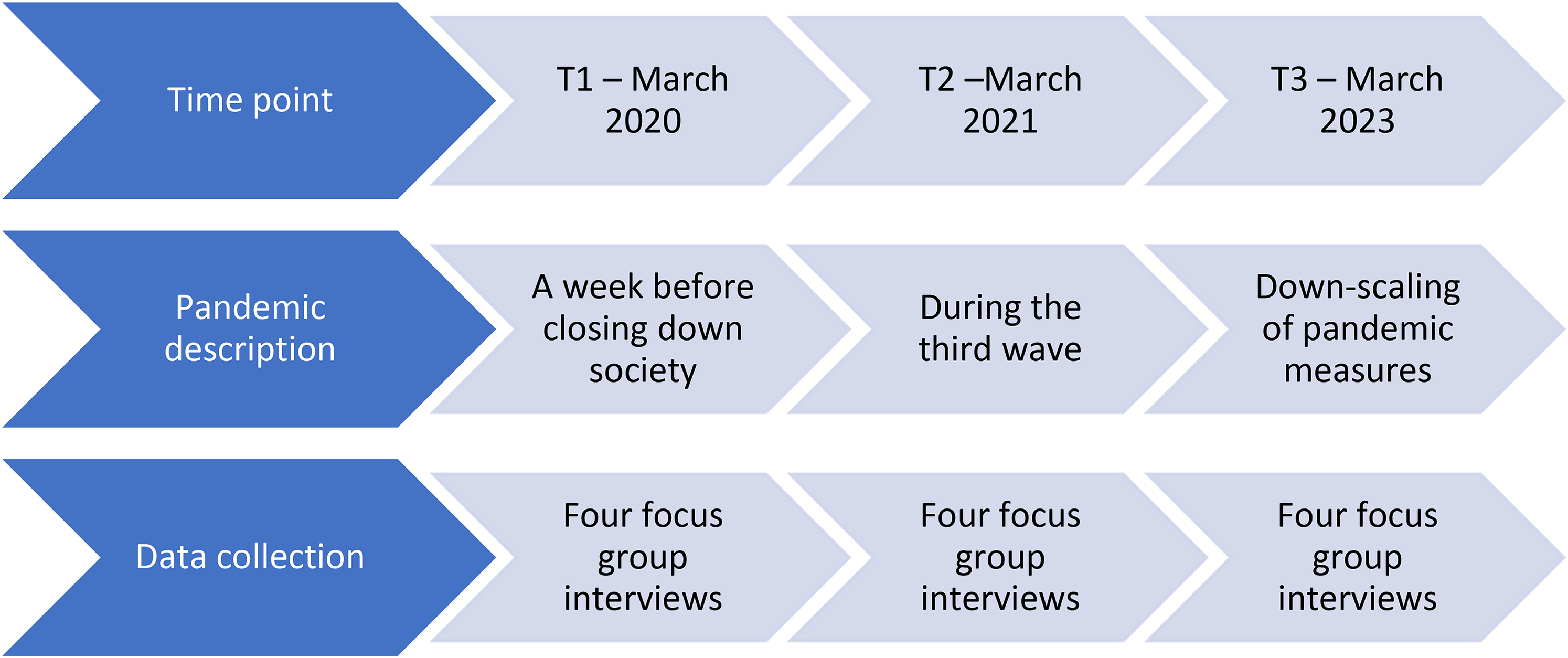
Timepoints for data collection in the COVID-19 pandemic context.
The foci for the interviews performed at T1 (Figure 1) were RNs’ narratives of their experiences of caring for patients with MDRB and their thoughts and motivation concerning engagement in antibiotic stewardship. At T2 and T3, the interviews were based on the same interview guide as T1 but updated in congruence with recent developments in the pandemic setting. We employed a through-time perspective in the interviews, meaning that we attempted to capture sequences of time rather than snapshots. 21 To manifest changes in T2 and T3, the participants were asked in retrospect to describe how their work situation had changed since the last interview. T2 was conducted during the third wave of the COVID-19 pandemic, and strict measures were implemented at the hospital to reduce the risk of spread. The interviews were all conducted face-to-face, but all participants wore masks and maintained distance from each other. Figure 1 illustrates the time points for the data collection during the pandemic.
All interviews were conducted by the first investigator, and all investigators were present at least at one interview at each time point. All of the investigators are female; three are registered RNs and academics, experienced with moderating and observing focus group interviews. The fourth investigator is a hospital physician specialised in medical microbiology. The interviews were audio-recorded and transcribed by the first investigator.
Data analysis
We applied a diachronic analysis approach, meaning that the analysis was conducted after all data had been collected. 29 We divided the analysis process into two phases (Figure 2). In phase one, we concentrated on analysing the transcripts from the various time points separately. The focus group transcripts were analysed by reflexive thematic analysis.30,31 The investigators read and reread the interviews, becoming familiarised with the data. As proposed by Tuthill et al., 32 we analysed the data deductively, using the theoretical frameworks (attitudes and self-efficacy; see interim themes in Table 2) that scaffolded our interview guide as a guide for coding and thematisation.

Schematic illustration of the analysis process.
Example from thematic matrix with summary of content of interim subthemes.

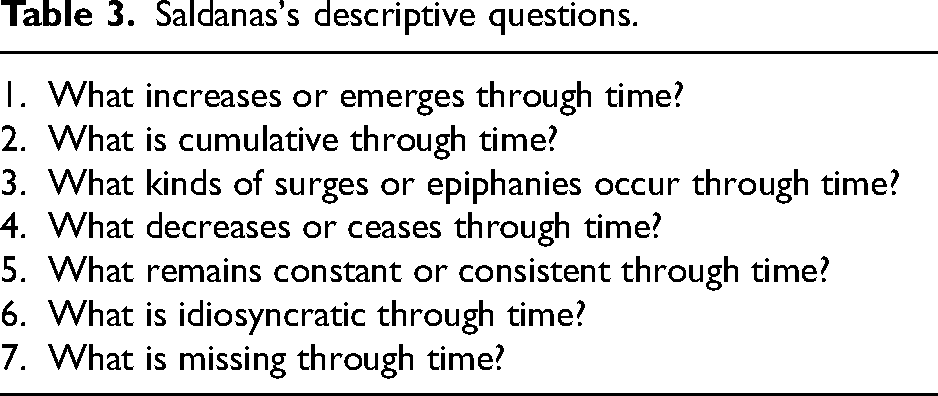
In the second phase of the analysis process, we sought changes in the data across the time points (Figure 2; see also example in Table 2). This phase started after all interviews were analysed separately, timepoint by timepoint. We inserted the analysed data into a thematic matrix, allowing for systematically comparing the content of the themes across the time points (Table 2). 29 In this phase, we strived for openness towards the data and used Saldanas's 33 descriptive questions to catalyse the analysis process of change through time (Table 3). We employed a more inductive approach to the data analysis. This process, actively using Saldana 33 descriptive questions, led to the development of four new themes. All investigators participated in the analysis, discussing the content of the different codes and themes.
Saldanas's descriptive questions.
Ethical considerations
This project followed the National Research Ethical Committee's 34 general ethical guidelines and the Declaration of Helsinki. It involved the retention of personal data (demographics), and the project description has been assessed and approved by the hospitals privacy commissioner (ID 807, 1515 and 1658). Participation was voluntary, and participants were assured that they could withdraw from the study at any time. All information about the participants has been treated with confidentiality, and the data are non-identifiable. Information that could identify the participants has at all times been kept separate from other data material; consent forms and questionnaires have thus been kept separately.
Results
The findings reported in the present reflect the analytical process of change through time, and each theme is presented longitudinally. The analysis resulted in four themes: (1) variable confidence towards IPC measures; (2) work environment and guidelines as consistent obstacles to correct behaviour; (3) altered feelings when caring for patients with MDRB; and (4) more confident in their role in antibiotic stewardship. Participant quotes and dialogue from the focus group interviews are included to give meaning to the text.
Participant characteristics
In total, 62 RNs participated in this focus group interview study (Table 4). Twenty-two (T1), 23 (T2) and 24 (T3) RNs participated in the four focus group interviews at each time point. Most (59%) were aged 30 years old or younger, female (91%) and had 5–14 years of nursing experience. One RN participated in a focus group interview at each time point (T1–T3), three RNs participated at both T1 and T2, two RNs participated at T1 and T3, and one RN participated at T2 and T3.
Participant characteristics in serial focus group interviews.

Theme 1: Variable confidence towards infection prevention and control measures
During the first round of interviews (T1, 2020), performed in the week before shutting down society because of the pandemic, the RNs displayed a hesitant yet confident mindset when asked about IPC. They expressed having faith in their own knowledge and judgement. For example, they felt that they had to teach other professions about both standard and transmission-based precautions. This confidence changed in the second round of interviews (T2, 2021) when most of the RNs expressed insecurities towards basic IPC measures. These insecurities were also underlined in the third round of interviews (T3, 2023). Instead of talking about themselves as the primary source of IPC knowledge in the wards, they enhanced the role of the nursing assistant. Furthermore, the RNs expressed a lack of confidence in their own knowledge and ability to assess the general risk of transmission, and they felt somewhat defenceless. During T3, the RNs frequently expressed a lack of confidence in their knowledge, as exemplified in this citation: Before COVID, we felt we knew everything, this is how it is. But now, the measures change all the time, and I no longer know if I’m doing it right. You just have to follow what is decided. (RN 4) (Interview 3, 2023)
The sources of knowledge on IPC varied throughout the study period. In T1, one of the RNs described the standard precautions as part of her reflexes. Still, RNs reported using the hospital's internal quality system, or phoning the department of infectious diseases, when in doubt. In T2, emails from leaders with new instructions and guidelines were described as the main source of new, updated knowledge. In T3, the RNs expressed frustration because they felt that new and important knowledge came through informal channels and was picked up by coincidence. Furthermore, they reported using the internal quality system more actively in the third round of interviews than in the second round.
Theme 2: Work environment and guidelines as consistent obstacles to correct behaviour
The RNs in all interviews across time reported high intentions to comply with the IPC guidelines. However, they described many obstacles to following the guidelines as intended. These obstacles were described similarly at all time points and did not appear to be influenced by the pandemic setting. The patient rooms were either too-small single rooms or overcrowded five-person rooms, the sinks in the patient rooms were placed illogically based on their patient care routines, the disinfectant was placed far away from the clinical workspace and the wards lacked written routines for environmental disinfection. These obstacles affected them in all patient care, including caring for patients isolated as a result of MDRB. Lack of time and personnel resources were also mentioned as challenges at all time points. Hand hygiene and environmental disinfection were mentioned as especially time-consuming during busy shifts, and understaffing was given as a reason for deprioritising IPC measures.
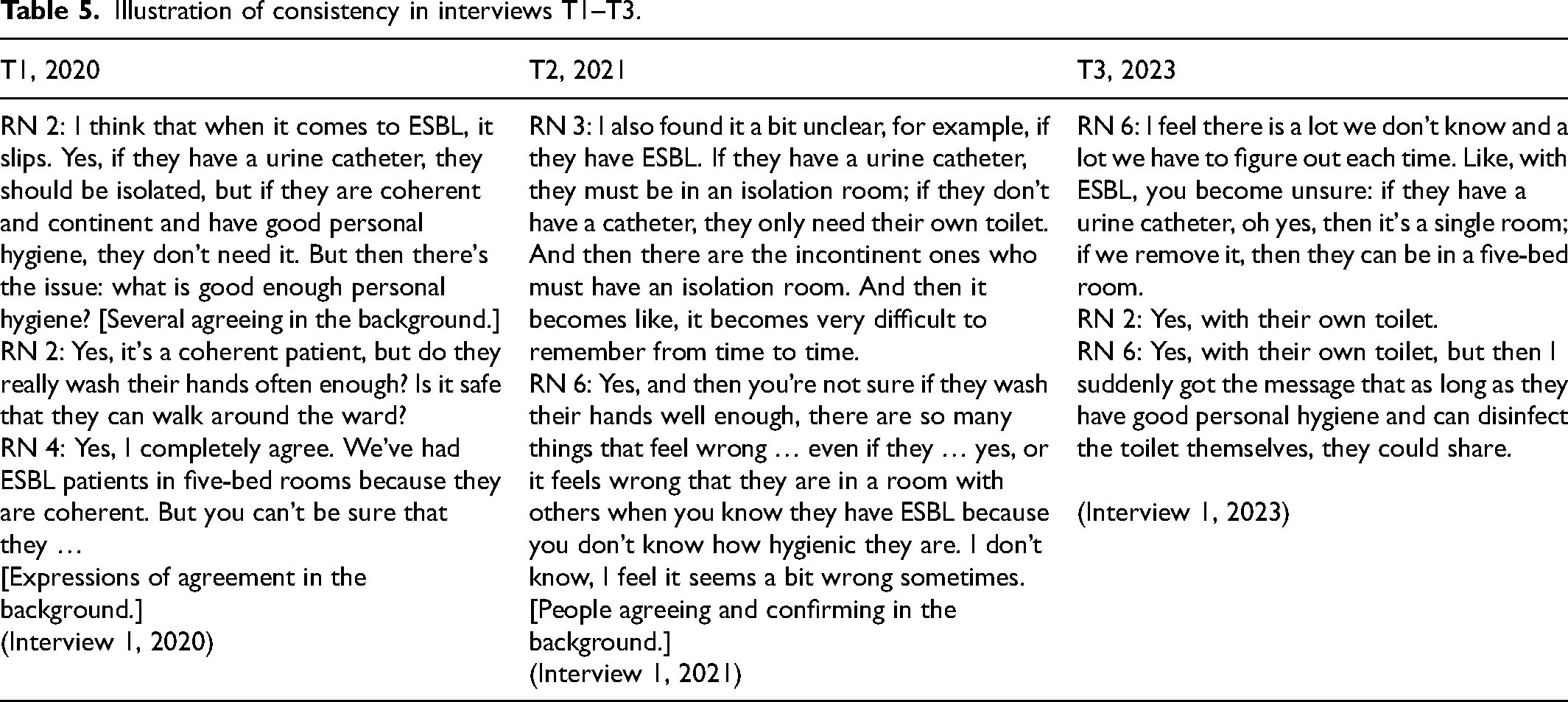
The IPC guidelines that apply to isolation care were a major topic in all the interview rounds. The RNs described the current guidelines as too long, illogical and difficult to use in the clinical context. They also found the guidelines open to too much interpretation, which made them practise the guidelines differently. For example, many of the RNs described it as confusing that patients colonised with bacteria producing extended-spectrum beta-lactamase in their urinary tract had to be isolated if they had poor personal hygiene and not if the personal hygiene was deemed adequate, as illustrated in Table 5.
Illustration of consistency in interviews T1–T3.
The RNs also reported many solutions to the described obstacles during the interviews and expressed general confidence both in present challenges and for meeting future challenges (T1–T3). This optimism was less prominent in the second round of interviews (T2) than before (T1) and at the end of the pandemic (T3). In one of the interviews from the second round (T2), a RN mentioned that sometimes guessing and reasoning, rather than knowing, was part of the solution.
Theme 3: Altered feelings when caring for patients with MDRB
At all time points, the RNs described having to rush when caring for patients isolated because of MDRB. Caring for isolated patients was laborious and time-consuming. The RNs expressed that this was not considered when leaders assessed the RNs’ workload. Caring for isolated patients took a great toll on the RNs. Words such as uncomfortable, demanding, frustrating, time-consuming and constraining personal protective equipment were used in all interviews to describe isolation nursing. They expressed wanting to take better care of the isolated patients but acknowledged that they planned every visit to the patient's room carefully to be as efficient as possible and reduce the number of times having to don and doff during a shift.
In T2, the RNs expressed a feeling of unsafety that was not mentioned in T1. They mainly blamed this on the sudden changes in IPC guidelines because of the developing pandemic. Moreover, having to use different personal protective equipment was a source of doubt. One example that was mentioned in many of the interviews in both T2 and T3 was the gowns used when caring for isolated patients. Before the pandemic, the gown was made of thin plastic, but, suddenly in the spring of 2020, the plastic gowns were reserved for RNs caring for patients isolated as a result of COVID-19. RNs caring for patients isolated as a result of other infections or colonisation, including MDRB, had to wear gowns made of cotton. This RN expressed fear of not being protected: But I almost think it's scarier to go into an isolation room to someone with ESBL with that cotton gown. It's too short on the sleeves and slide up while changing on bedbound patients. This, compared to going into someone suspected of having COVID-19, or with confirmed COVID-19 for that matter, but in full protective gear, with eye protection, mask and disposable gown. They, at least, were well-protected. (RN 3) (Interview 4, 2021)
During the interviews in 2020 and 2023, the RNs expressed positive feelings by sharing a laugh, often while describing difficult and demanding situations. For example, in many of the interviews, the RNs joked about the probability of unknowingly carrying all kinds of different MDRB. In the following dialogue, two RNs talk about not only how challenging, but also how contradictory the situation could be: And yes, you wonder if it's good enough sometimes. Again, if it's a coherent patient I’m going to, I don’t feel so unsafe, but if it's someone who touches surfaces here and there and you have to avoid getting the patient's hands in your hair, then it's a bit like, yes, I’ll probably bring this home with me. (RN 2) But if we start thinking like that, we won’t be able to work here, hehe … [Several chuckling in the background.] (RN 3) (Interview 1, 2020)
Theme 4: More confident in their role in antibiotic stewardship
At all three time points, the participants were unfamiliar with the term antibiotic stewardship. When an explanation was given, participants in all the interview rounds stated vital tasks in antibiotic stewardship independently performed by RNs. Examples were antibiotic administration, handling antibiotic waste responsibly, systematic observations of patients at post-administration and taking microbiological samples. Additionally, the RNs exhibited much knowledge of antibiotics. For example, they discussed challenges such as kidney failure, narrow- versus broad-spectrum antibiotics, postoperative spikes in c-reactive protein versus infections, and the length and route of antibiotic administration. These types of discussions were more explicit in the third round of interviews: They [physicians] often focus more on CRP [c-reactive protein] than the clinical state of the patient. (RN 1) I agree, it's very common. Even a slight increase in CRP and they start antibiotics. (RN 4) They can have cancer-related CRP, yeah, but does he have a fever or something? They can have a CRP of 100 and still be completely fine. (RN 3) We also have a lot of postoperative patients with small spikes in CRP, where I believe it would resolve on its own, but they still prescribe antibiotics anyway (RN 4) (Interview 3, 2023)
The participating RNs conveyed in all rounds of interviews that antibiotics were a significant part of their day. They noted that they had an important role in securing the quality of the physicians’ prescribing practices, especially if the physician was inexperienced or during weekends when physicians were less available. Some of the RNs expressed scepticism about contributing to the correct use of antibiotics, arguing that prescribing according to guidelines is the physician's responsibility. Still, most expressed interest in the prescribing practices of the physicians.
Focus group interactions
The focus group interactions were mainly positive and supportive across the interviews. The participants used confirmative expressions (e.g. nodding, words of agreement, laughing). 35 Sometimes the participating RNs disagreed, but mostly over minor subjects, such as negligible differences in understanding of guidelines.
Discussion
In the present study, we aimed to explore hospital RNs’ experiences of change in attitudes and self-efficacy when caring for patients with MDRB in a pandemic context. Our pre-assumption was that, because MDRB isolation practices are similar to COVID-19 isolation practices, the knowledge and experience that the RNs gained through the pandemic would positively affect their attitudes and self-efficacy concerning IPC and antibiotic stewardship in MDRB care.
When caring for patients with MDRB, IPC knowledge and skills and antibiotic stewardship are important. Our findings indicated that RNs, before the pandemic, were confident in their IPC knowledge and skills. Interestingly, during the second and third round of interviews, they frequently expressed a lack of confidence in their own competence rather than more confidence, which was our assumption. Our data suggested that the RNs’ confidence in their skills and knowledge of IPC was challenged during the pandemic. Constantly changing guidelines, together with changes in the personal protective equipment used when caring for patients with MDRB, made the NRs question both their understanding of IPC and their personal safety. Many studies have found that the COVID-19 pandemic represented a tremendous challenge to the work of hospital RNs and that the pandemic amplified insecurities concerning IPC.20,36 Gebreheat and Teame 36 noted several of the ethical challenges that RNs faced during the pandemic, including being asked to work under circumstances that put their overall health and well-being at risk, partly because of the lack of adequate personal protective equipment. Gebreheat and Teame 36 postulated that the overall consequences of such challenges may have left permanent scars on the modern nursing profession. Luckily, the insecurities we found in T2 (2021) were less prominent in the interviews of 2023 – but not all gone. We also found that the RNs participating in the study had consistently high self-efficacy, which earlier studies have shown positive effect on stress and burnout in RNs during crises. 16
We found consistent frustration through time among the participating RNs towards the practical usability of the IPC guidelines, including those that apply to isolation care. The preference for detailed recipes rather than general guidelines that allow for situation-based professional assessments can be interpreted as a sign of insufficient understanding of practical IPC. Recent studies show that, when RNs lack basic knowledge of MDRB, patients receive inadequate information, resulting in confusion about, for example, the necessity of isolation.8,37 Some patients in the study by Watson et al. 8 reported receiving contradictory information and explanations from staff. Research has shown that RNs caring for patients with MDRB highly value their ability to apply theoretical knowledge to their clinical practice, and they report experiencing negative feelings when they cannot provide isolated patients with adequate information. 38 An understanding of the rationale behind different IPC measures and how microbes spread, as well as being able to explain to a patient what antibiotic resistance means and different ways to prevent further development and spread, might both positively impact RNs’ and patients’ attitudes.
Our findings suggested that the physical work environment, lack of time and personnel resources, and inconsistent guidelines hindered RNs from complying with IPC guidelines. This did not change during the pandemic. The hospital building stayed the same, and as far as the we are informed, the level of RN staffing has remained unchanged. Other studies have also found that RNs’ work environments affect their IPC behaviour. A lack of access to hand disinfection and personal protective equipment, heavy workload, crowded wards and patient rooms not designed for isolation have been shown to complicate compliance with both standard and transmission-based precautions.39,40 Nonetheless, in the interviews, the RNs spoke with optimism for the future. The participating hospital is about to move into new, highly modern buildings, including single rooms with ensuite baths. Studying whether and how the attitudes and self-efficacy of RNs change in a new environment is thus an exciting opportunity for further research.
Regarding caring for patients with MDRB, the findings through time converged. Negative consequences of adhering to the IPC guidelines, such as simple tasks being extra time-consuming and uncomfortable, were mentioned at all time points. The RNs also talked about feeling guilty because they were not always able to provide the care that they wanted to patients isolated as a result of MDRB. Unfortunately, isolated patients not receiving the same amount of care as other patients is not a new phenomenon.41,42 Studies that have examined patients’ experiences with being isolated find them feeling lonely, segregated and stigmatised. 37 This finding underlines a need for hospital managers to accept that isolation nursing is time-consuming and complex and thus provide RNs with the resources needed to care adequately for these patients.
Despite reporting negative reactions to caring for patients with MDRB, the RNs consistently demonstrated a high level of self-efficacy, reflecting their confidence in managing challenging situations. For example, even when discussing their fear of contracting MDRB, the RNs described caring for these patients as safe and familiar, particularly compared to caring for patients isolated as a result of COVID-19. High self-efficacy is positively correlated with adherence to correct IPC practices.7,43 The manifestation of high self-efficacy among the RNs, even amid a healthcare crisis, underscores its significance as a vital resource for hospitals during such times and warrants recognition.
When caring for patients with MDRB, knowledge and skills in antibiotic stewardship are important. According to the World Health Organization, 4 IPC interventions, optimal diagnostics and antibiotic stewardship play significant roles in reducing the development and spread of MDRB. That RNs are integral to securing optimal antibiotic stewardship practices is no longer controversial. 10 Still, studies show that RNs must enhance their knowledge and skills in both ICP and antibiotic stewardship.10,44 We found a change in the RNs’ confidence in their role in antibiotic stewardship as time passed. In the interviews conducted in 2023, conversations concerning antibiotic use in the hospital among the RNs may be perceived as more professionally grounded than in 2020. This finding may indicate that RNs progressively recognised and embraced their roles as antibiotic stewards during the pandemic.
Strengths and limitations
In serial focus groups, the same groups are resumed several times over an extended period, periodically revisiting the same focal issue through interactive discussions. 22 Because we aimed to describe changes in hospital RNs’ attitudes and self-efficacy when caring for patients with MDRB, ‘RNs’ were the group of interest. As a result of sickness leave, logistics and turnover, we had to have a pragmatic way of defining ‘same groups’ as RNs from the same contexts with similar backgrounds and experiences. The fact that few of the RNs participated at all timepoints may have affected the essence of serial group interviews. Still, we argue that, by changing the groups, we prevented some of the known pitfalls of multiple focus group interviews, such as cognitive transformation, where the participants change their knowledge and thoughts based on the information exchanged in the group. 22
The data were analysed deductively in the first phase of the analysis process. This may have hindered us from openly searching for codes and themes, which may have led to overlooking the depth, nuance and complex nature of qualitative data. 31 Longitudinal work is meant to examine change. 45 Because we used the same interview guide at all time points, we may have overlooked prominent changes in the RNs’ attitudes and self-efficacy. However, the data collection and analysis process was conducted by all investigators, allowing for discussions to secure reflections on our preunderstandings during the process.
The pandemic situation differed in severity from country to country. Norway implemented early intrusive measures, such as closing workplaces, schools and kindergartens, and has a highly functioning health-related infrastructure; it had low numbers of detected cases compared to other countries. 24 Moreover, Norway is considered a low-prevalence antimicrobial resistance country. 27 These factors may impact the study's transferability.
Implications for policy and practice
Our findings indicate that frequent modifications to IPC guidelines during a crisis decrease RNs’ confidence in their ability to safely care for isolated patients. This underscores the necessity for a deeper comprehension of the principles underlying IPC measures among RNs. Enhanced understanding can facilitate more context-specific professional judgements, thereby reducing the reliance on detailed procedures. Our results suggest that hospital management should consider the time-intensive nature of isolation nursing when planning personnel resources. Furthermore, our findings reveal that RNs are increasingly recognising and assuming their roles as antibiotic stewards. The high levels of self-efficacy demonstrated by clinical RNs can be regarded as a crucial resource for hospitals during crises.
Conclusions
We aimed to explore hospital RNs’ experiences and changes in attitudes and self-efficacy when caring for patients with MDRB. The results from the focus group interviews, covering 3 years through the COVID-19 pandemic, revealed that the participating RNs’ experienced changes impacting their attitudes to caring for patients with MDRB. However, they expressed consistent solution orientation, indicating a steady self-efficacy even through times of change. The physical environment in which RNs work was presented as an obstacle hindering adequate IPC behaviour. Future research should explore how physical surroundings can enhance RNs’ adherence to IPC guidelines in hospitals.
Supplemental Material
sj-docx-1-njn-10.1177_20571585251335871 - Supplemental material for Caring for patients with multidrug-resistant bacteria in a pandemic: A qualitative, longitudinal focus group study of nurses’ experiences
Supplemental material, sj-docx-1-njn-10.1177_20571585251335871 for Caring for patients with multidrug-resistant bacteria in a pandemic: A qualitative, longitudinal focus group study of nurses’ experiences by Marte Johanne Tangeraas Hansen, Heidi Syre, Marianne Storm and Anne Marie Lunde Husebø in Nordic Journal of Nursing Research
Supplemental Material
sj-docx-2-njn-10.1177_20571585251335871 - Supplemental material for Caring for patients with multidrug-resistant bacteria in a pandemic: A qualitative, longitudinal focus group study of nurses’ experiences
Supplemental material, sj-docx-2-njn-10.1177_20571585251335871 for Caring for patients with multidrug-resistant bacteria in a pandemic: A qualitative, longitudinal focus group study of nurses’ experiences by Marte Johanne Tangeraas Hansen, Heidi Syre, Marianne Storm and Anne Marie Lunde Husebø in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We thank all of the nurses who participated in the study and all the helpful nursing leaders for their identification of eligible interviewees.
Data availability statement
Data sharing is not applicable to this journal as the subject matter covered by the aims & scope does not necessitate the need for the use of empirical data, software or code. As such, no datasets, software or code may be generated or analysed by the articles published in the journal.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
This project followed the National Research Ethical Committee's general ethical guidelines and the Declaration of Helsinki. It involved the retention of personal data (demographics), and the project description has been assessed and approved by Stavanger University Hospitals’ privacy commissioner (ID 807, 1515 and 1658). Participation was voluntary, and participants were assured that they could withdraw from the study at any time. All participants signed a written informed consent for participation and publication. All information about the participants has been treated with confidentiality, and the data are non-identifiable. Information that could identify the participants has at all times been kept separate from other data material; consent forms and questionnaires have thus been kept separately.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.