
Abstract
Background:
The UK 5-year antimicrobial resistance (AMR) National Action Plan highlights the need to prevent community infections through education of children. Activities around infection prevention (IP) and antibiotics were piloted by UK youth groups in 2016–2018, prompting Public Health England (PHE) to develop a standardised programme. The aim of the study was to develop and pilot an educational programme on IP and antibiotics for use by community youth groups in the UK.
Methods:
A working group, including youth group volunteers interested in IP and AMR, agreed on the programme content through consensus, informed by the Capability, Opportunity, Motivation, Behaviour model (COM-B). The Antibiotic Guardian Youth Badge (AGYB) included learning through interactive e-Bug activities on IP and prudent antibiotic use, action setting through Antibiotic Guardian pledges and consolidation through poster development. The programme was piloted and evaluated with conveniently recruited youth groups in 2019, including quantitative and qualitative questionnaire feedback from community leaders and children.
Results:
Fourteen youth group leaders and 232 children from uniformed Girlguiding/Scout groups in England and Scotland participated in the pilot evaluation, as well as two primary schools. Leaders reported alignment to the themes of their youth organisation, but struggled to teach antibiotics and antibiotic resistance. Children reported enjoyment and intentions to improve hygiene behaviour.
Conclusion:
Community youth groups are a suitable setting for IP and antibiotics education. The AGYB was officially launched in March 2020 and promoted for use with home-schooling children and remote youth group meetings to educate about IP during the coronavirus disease 2019 (COVID-19) pandemic.
Background
The UK five-year National Action Plan and 20-year vision on antimicrobial resistance (AMR) highlights the importance of promoting infection prevention (IP) to children and young people (HM Government, 2019a; HM Government, 2019b). Young people are commonly prescribed antibiotics, but lack knowledge of their appropriate use (Eley et al, 2019b) and IP interventions can improve behaviour and reduce infections in educational settings (Ernestina et al, 2016; Lecky et al, 2010; Willmott et al, 2015). Lack of time and relevant topics in the school national curriculum can mean IP topics are not covered (Eley et al, 2019a); therefore, community IP and antibiotics education could help improve awareness (Eley et al, 2018).
The Youth United Foundation estimates that 1.5 million young people aged 4–24 years in the UK attend youth groups such as Cadets, Scouts, Girlguiding, Brigades and St. John Ambulance (Youth United Foundation, 2019). These groups focus on youth development, community action and health and wellbeing, which complement the topics of IP and AMR.
Activities using Public Health England (PHE) materials, e-Bug and Antibiotic Guardian, were piloted in 2016–2018 by English and Scottish Girlguiding and Scouts groups, which prompted the development of a programme to provide any youth-based community group with the opportunity to cover IP and antibiotic topics. e-Bug resources are interactive and can improve antibiotic knowledge and IP skills of young people in school and community settings (Eley et al, 2018; Lecky et al, 2010). Implementation intentions, including the Antibiotic Guardian campaign, can motivate behaviour change in adults around antibiotics and hygiene (Kesten et al, 2017; Little et al, 2015). Pledging is a common practice in youth groups; an example is the Girlguiding ‘promise’ to help others and to be an active citizen in the community (Girlguiding, 2019). The coronavirus disease 2019 (COVID-19) pandemic makes IP an essential component of youth behaviour, and such a resource could be used to help reduce the spread of the infection.
Behavioural models can help to understand and target interventions to determinants of behaviour. Antimicrobial stewardship (AMS), the discipline which seeks to optimise antibiotic prescribing and use in society and health care, does not have a specific behaviour theory and therefore broader models such as COM-B are often used (Public Health England, 2015). COM-B describes three conditions that interact to initiate behaviour: capability (the physical or psychological ability to engage in behaviour), opportunity (environmental or social factors that support the behaviour) and motivation (beliefs that direct behaviour) (Michie et al, 2011).
This study aimed to develop an IP and antibiotics educational programme informed by existing strategies, the COM-B behavioural framework and a pilot evaluation with youth groups based in the UK.
Methods
Programme development
PHE developed a working group, including youth group leaders, educators and healthcare professionals, to agree the content of an educational programme around IP and antibiotics. A consensus process via teleconferencing facilities was used to modify e-Bug, Antibiotic Guardian and previous pilot materials. The programme was also informed by the COM-B behavioural framework, common themes between youth groups, and the findings of the pilot evaluation.
The ‘Antibiotic Guardian Youth Badge’ (AGYB) included three stages which aimed to improve children’s capability, opportunity and motivation to improve their own and promote appropriate IP and antibiotic use behaviours with their families. Figure 1 shows how the different stages of the programme aligned with the COM-B model. Key feedback from youth leaders in the working group was that groups differ in size, available resources, the age and ability of children, and time available. The intervention therefore needed to be flexible so that leaders could tailor it and deliver over multiple sessions if needed. To support this, a range of activities were included with accompanying information on age group, difficulty, timing, resources and learning outcomes.
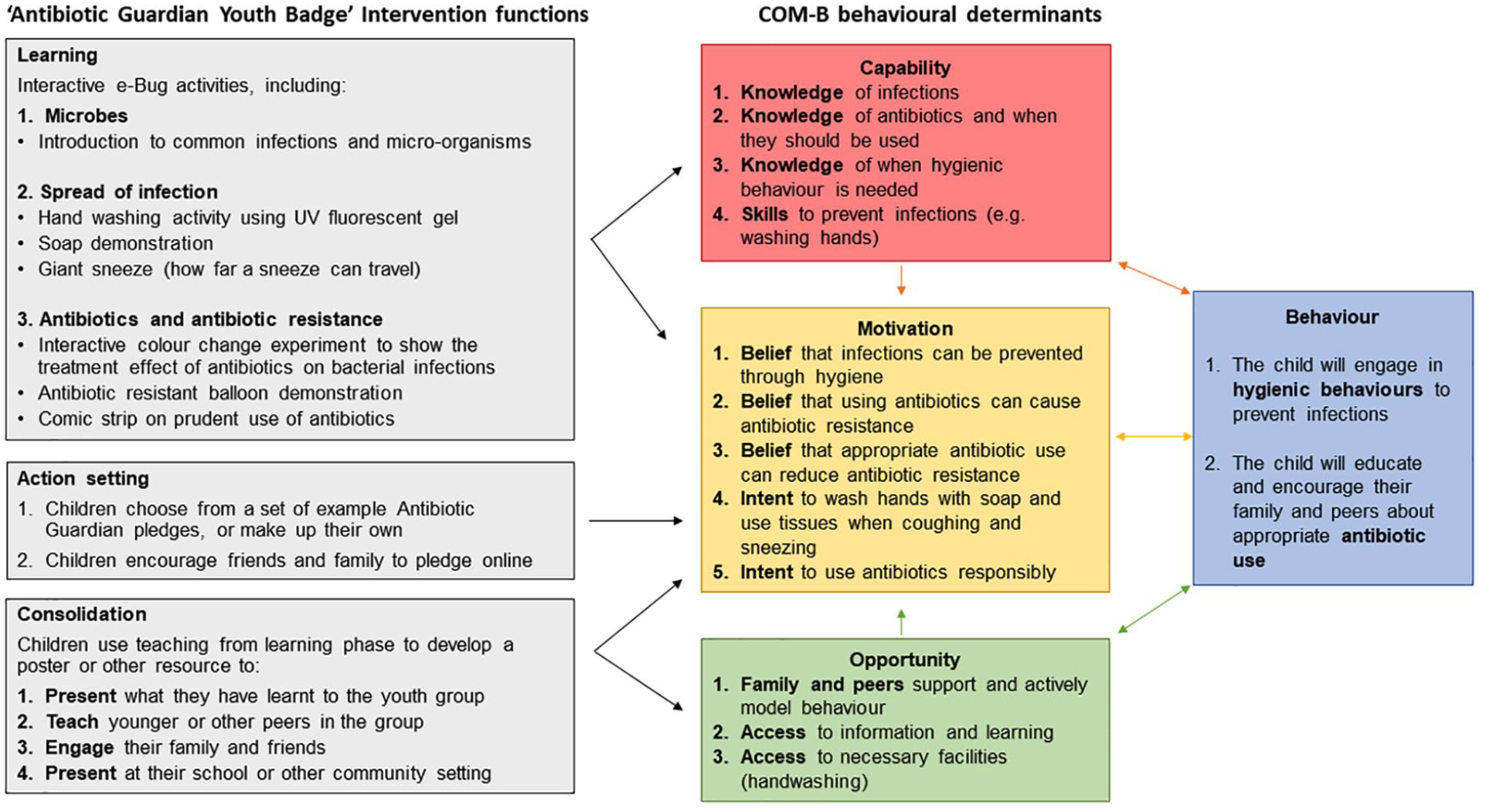
Antibiotic Guardian Youth Badge linked to the COM-B behavioural model.
Pilot evaluation
Recruitment
An initial trial of the AGYB and questionnaires was done by the research team with two conveniently recruited schools. These data are included in this paper as no changes were made as a result.
Youth groups were recruited through convenience sampling. Youth group leaders in the working group cascaded information to local networks via email and social media (six groups recruited). The opportunity to trial the AGYB was also advertised on the e-Bug twitter and facebook accounts to an audience of 2000 (three groups recruited) and newsletters sent to the e-Bug mailing list of 1900 school nurses, teachers and health professionals (no recruitment).
Questionnaire development
Leader and children’s questionnaires (Supplementary files 1–3) including closed and open questions were developed by experienced PHE researchers with a background in questionnaire design and reviewed by the working group.
Leader feedback: 18 questions to collect feedback on the delivery and content of the programme.
Child feedback (written): 11 pictorial questions around enjoyment and behavioural intentions.
Child feedback (verbal): version of questionnaire 2 to be facilitated by leaders to tally verbal feedback directly from children.
The leader questionnaire was based on one previously piloted with youth group leaders in the working group and the children’s questionnaires were based on those validated in previous evaluations of the e-Bug resources (Eley et al, 2018; Eley et al, 2019b; Young et al, 2017). The verbal method was requested by youth group leaders for children of younger age and less capability.
Delivery of intervention and data collection
Community leaders delivered the intervention flexibly to their usual groups, with core requirements to cover all three stages of the intervention, and include at least four e-Bug activities. Resource constraints meant it was not possible to observe sessions for fidelity or provide materials to youth groups; however, youth leaders were provided with a £20 high street voucher. Data collection took place between February 2019 and September 2019 inclusive. Leaders returned completed questionnaires to PHE for analysis.
Data analysis
Quantitative data were inputted into Microsoft excel and analysed with descriptive statistics. The open-ended qualitative responses were inputted into NVivo 11 software and this was used to organise, code and analyse feedback. Two researchers (CH and MH) independently coded themes and resolved any minor discrepancies through discussion. A descriptive analysis report was developed and discussed with the working group; quotes were chosen from a range of participants which reflected the agreed themes.
Ethics
This study did not require National Research Ethics Service (NRES) approval as it was outside the National Health Service and classed as a service evaluation. Data were collected by youth leaders who provided consent for its use in development of the educational materials. No identifying information was collected on questionnaires and data were stored in line with the Data Protection Act 2018 and Caldicott 1999 regulations on handling and distributing sensitive participant information.
Results
Nine Girlguiding and Scout youth groups and two primary school groups from England and Scotland took part in the pilot evaluation. Of these, 232/252 children and 14 leaders completed questionnaires (Table 1). At least one leader from each group gave feedback and children from eight of the groups completed either the written or verbal questionnaire.
Adult and child participants in the pilot evaluation.
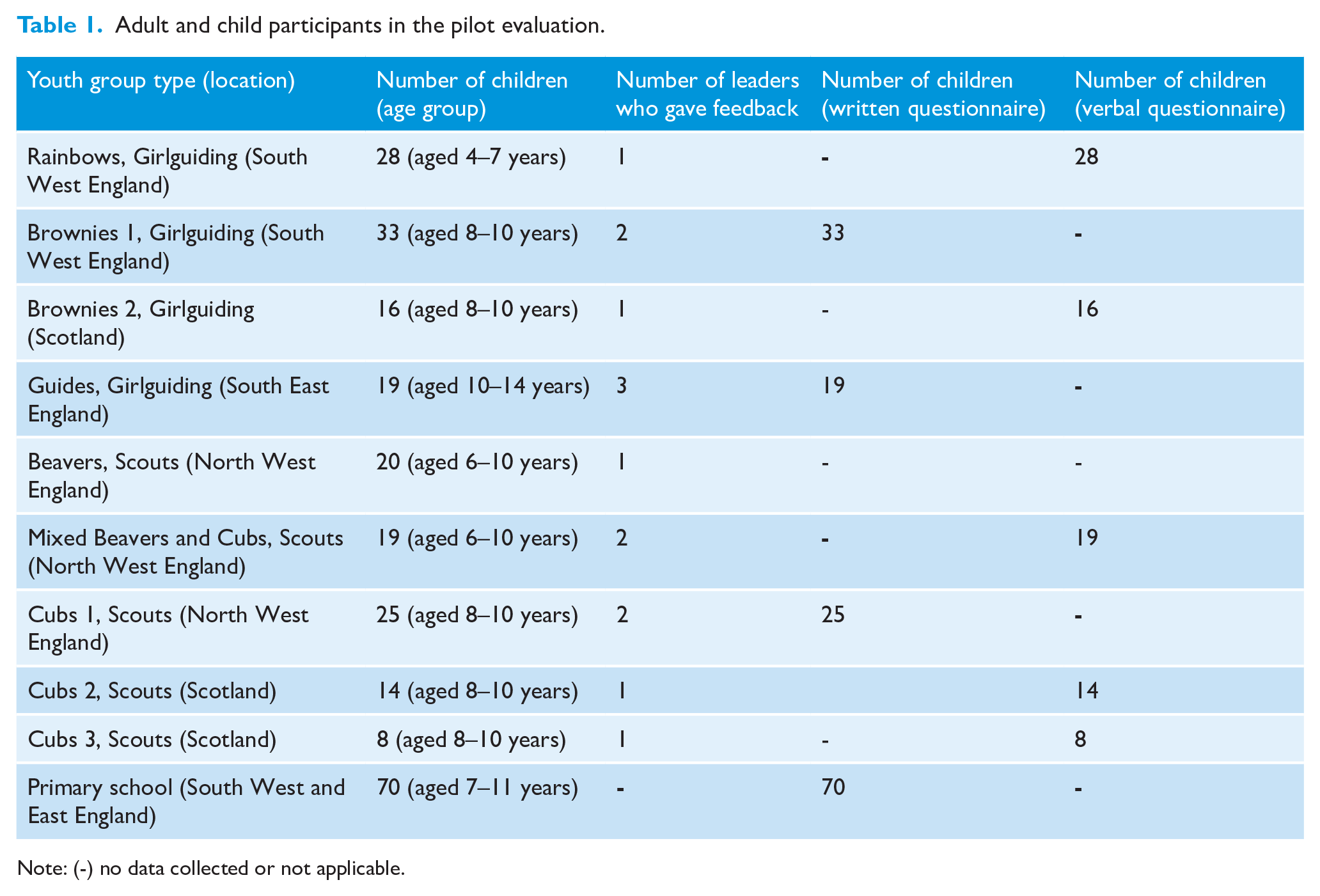
Note: (-) no data collected or not applicable.
Leader feedback (n=14)
Five of the nine groups completed the AGYB over two sessions and four completed it in one session. All leaders agreed or mostly agreed: the topics covered in the programme were important for children to understand; the activities were age appropriate; they felt confident to deliver the programme; and they would run it again or recommend to others. All leaders agreed or mostly agreed that the children in their group understood the concepts taught and that the activity pack provided sufficient information. Overall, 22% of leaders reported that some changes could be made to the programme.
Leaders reported that the programme filled a niche and that children enjoyed the creative activities. They reported that the activities were easy to organise, and most used inexpensive materials.
The idea of the badge is superb as it makes kids aware of microbes and antibiotic use on a wider, yet relevant scale. Brownie leader 3, England
Leaders liked that the programme aligned with existing themes of their youth organisations and could fulfil other challenge badges around science or health. One leader reported that some of the activities could be delivered by adolescents to peers.
It meets part of the Beaver experiment badge and cub scientist badge but need more experiments to fill the badge criteria. Beaver and cub leader 1, England
Let the older guides run the game activities, they did a fab job. Guide leader 3, England
Leaders reported difficulty in teaching children about antibiotic resistance and requested descriptions suitable for children. One leader reported using stories of superheroes and villains to explain concepts of antibiotic resistance to younger children.
Age appropriate description of antibiotic resistance could be included in the resource pack. Cub leader 2, Scotland
Some leaders felt confident to deliver the programme due to an existing knowledge of the topic. Other leaders who lacked a background in science required more information or links to further information.
I am a scientist who works in this area and so it was no problem for me but some others needed more information. Rainbow leader 1, England
Child feedback (n=232)
Eighty-five out of 232 children in the younger age bracket (4–10 years) provided verbal feedback via their leader. Figure 2 shows children reported high enjoyment of the session and intentions to wash hands with soap.
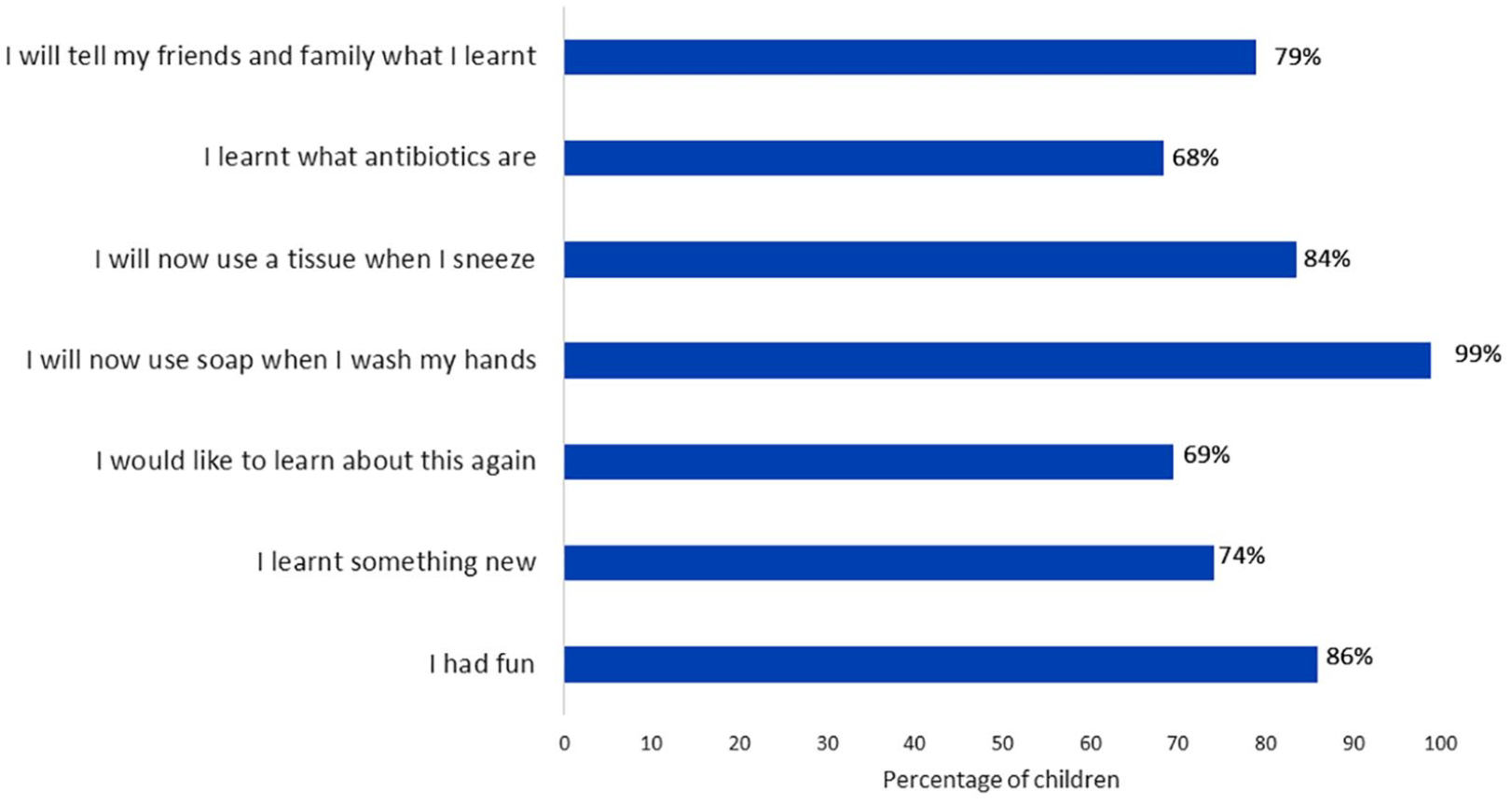
Verbal opinions of children aged 4–10 years (n=85) taking part in session, collected by leaders.
Of the 147 out of 232 children in the older age bracket (8–14 years) who provided written feedback, 96% reported enjoyment of the session and learnt something new; 85% agreed they would share information with family and friends. Handwashing was reported as the most important information to share (53 children, 41%) and 46 children (36%) stated that they would encourage their family and friends to pledge to become an antibiotic guardian online.
The most important thing I will share with my family is to always use soap to wash their hands. Primary school child 9, England
Antibiotics don’t work with viruses. Brownie 16, England
Children made Antibiotic Guardian pledges to engage in hygienic behaviour and educate others about antibiotics (Figure 3). Children reported behavioural intentions after completing the AGYB (Figure 4), with the majority (69%) intending to always wash their hands with soap. Less children reported intentions to use antibiotics only when they are needed in the future.
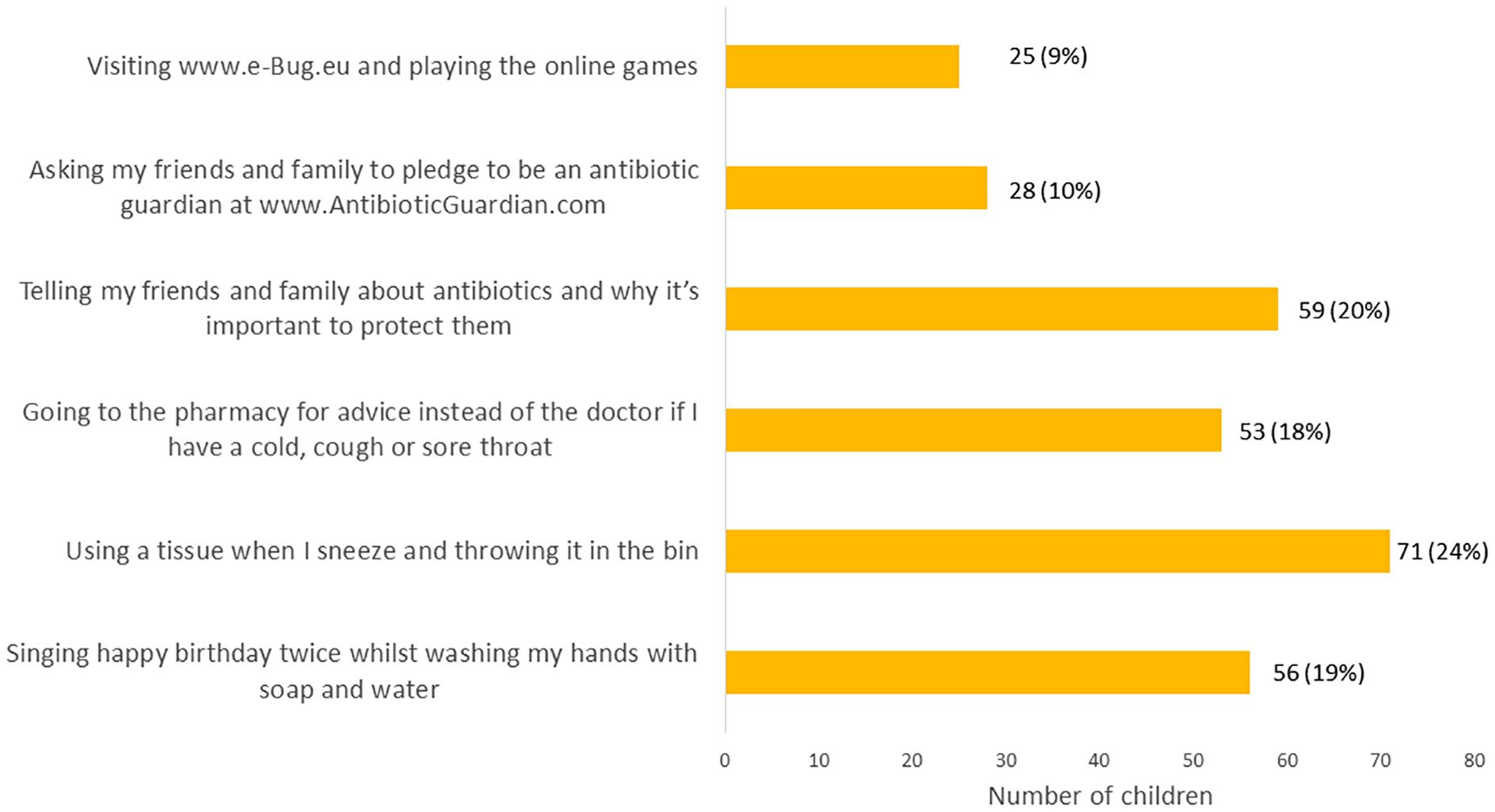
Antibiotic Guardian pledges chosen by children aged 8–14 years (n = 147).
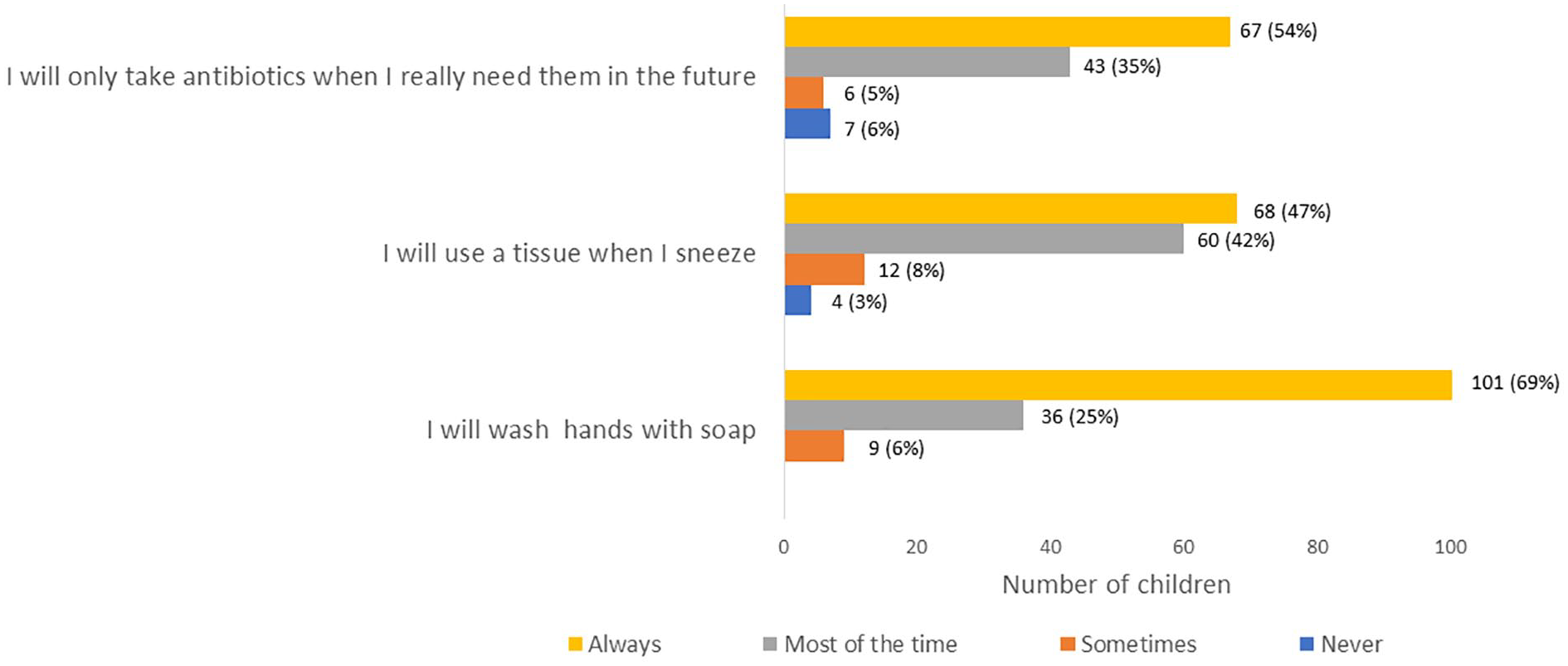
Self-reported behavioural intentions of children aged 8–14 years (n = 147) after completing Antibiotic Guardian Youth Badge.
Discussion
Main findings
Pilot evaluation of the AGYB led to a high number of children reporting intentions to always use soap when washing hands and to encourage this behaviour with friends and family. Children may not have understood information on antibiotics as a lower number expressed intentions to ‘use antibiotics only when needed in the future’. Yet, children reported intentions to educate their families about antibiotics and encourage them to pledge to be antibiotic guardians. Many leaders reported difficulty in teaching about antibiotics, which may have led to lack of understanding by children. Leaders reported positive views of the AGYB, believed the topics were important for children to understand and valued that the programme aligned with existing themes of their youth organisations.
Strengths and limitations
The AGYB intervention is based on existing evidence-based strategies, behavioural science and the input of youth group leaders. A flexible approach allows leaders to tailor sessions based on capability and resources, including budget. The pilot evaluation included a large sample of children from England and Scotland, aged between 4 and 14 years; however, other areas of the UK and children older than 14 were not represented. There was a lack of children from other youth groups, such as Cadets, however the shared themes of youth groups and the flexible nature of the programme mean it is likely to be suitable for a range of group types.
The convenience sampling strategy meant it was not possible to select groups based on characteristics such as socioeconomic status and as a self-selected sample, there may have been groups led by leaders with an interest in IP and AMS. The inclusion of school children in the sample from the initial trial may bias results; however, it suggests the AGYB may be suitable for school-based clubs. Written questionnaires may not be feasible for younger children and the verbal approach is open to acquiescence bias. Other interactive methods of data collection should be explored for children such as concept meaning maps (Wheeldon and Faubert, 2009). For this pilot evaluation it was not feasible to observe sessions or collect outcome data.
Comparison with existing literature
e-Bug resources significantly improve young people’s knowledge and attitudes towards hygiene and antibiotics in a variety of settings, including schools (Eley et al, 2019a; Eley et al, 2019b; Lecky et al, 2010; Young et al, 2017), the community (Eley et al, 2018) and family science shows (Lecky et al, 2014). This work further supports the value of e-Bug and community-based IP and antibiotics education. The authors have previously reported that knowledge of and confidence to teach about IP and antibiotics varies significantly between school and community educators (Hayes et al, 2020). Community educators are often volunteers and come from a range of backgrounds, not necessarily education or science, and therefore training or further support is needed to lead sessions on scientific topics.
Antibiotic Guardian pledging improved adults’ knowledge and behaviour around antibiotics (Chaintarli et al, 2016; Kesten et al, 2017), and the online ‘Germ defence’ tool improved hand hygiene behaviour and infections rates within families (Little et al, 2015). Our study suggests that action planning around antibiotics and hygiene may also improve behavioural intentions of children; however, further follow up studies are needed to explore integration with families and explore long-term effects on behaviour.
This is the first study, known to the authors, to report an educational IP and antibiotics intervention with community youth groups. Previous health interventions in the USA have reported improvements in scouts’ attitudes and behaviours towards nutrition and physical activity (Cullen et al, 1998; Gallaway et al, 2007; Guagliano and Rosenkranz, 2012; Rosenkranz et al, 2010; Sotgiu et al, 2009). A common theme is the benefit of including family in interventions (Guagliano and Rosenkranz, 2012; Rosenkranz et al, 2010); therefore, a family-centred approach to the AGYB may help maximise any behaviour change around IP and antibiotics.
Implications for local authorities, public health and youth groups
In March 2020, during the COVID-19 pandemic the AGYB was promoted to parents and youth leaders for home-schooling and remote learning. The AGYB could be promoted to community groups as part of antibiotic-related improvement action plans, and other public campaigns to minimise transmission of infections.
Community youth groups are a suitable setting to deliver health education to influence the behaviour of young people. The AGYB fulfils a niche and supports youth group themes around health and wellbeing and community action, and is suitable for peer-to-peer teaching, which the e-Bug activities can support (Young et al, 2017). Children demonstrated intentions to share learning with family, and therefore should be encouraged to replicate activities at home, or take home written material including leaflets.
Implications for the AGYB and future work
Following the pilot evaluation, more activities around antibiotics, including experiments and storyboards, as well as alternative activities with cheaper and readily available materials were included in the AGYB resource. Further support for teaching antibiotics was provided via online e-Bug training (Future Learn, 2020) which is being promoted to local authorities and community leaders. Future evaluation of the AGYB could include collection of data to inform changes in capability, opportunity and motivation around IP and antibiotic use before and after the activities, measured through increased handwashing indicated by soap use, and reductions in rates of infection.
Conclusion
The AGYB is a valuable resource to engage young people with IP and antibiotics and is transferable to a range of settings, including community groups, educational settings and home learning. Community youth groups are a suitable setting to provide young people with the opportunity, motivation and capability to prevent infections and spread awareness of antimicrobial stewardship in their communities and families. The Antibiotic Guardian Youth Badge pack and information is freely available on the e-Bug website.
Supplemental Material
sj-docx-1-bji-10.1177_17571774211012463 – Supplemental material for Development and pilot evaluation of an educational programme on infection prevention and antibiotics with English and Scottish youth groups, informed by COM-B
Supplemental material, sj-docx-1-bji-10.1177_17571774211012463 for Development and pilot evaluation of an educational programme on infection prevention and antibiotics with English and Scottish youth groups, informed by COM-B by Catherine V Hayes, Charlotte V Eley, Diane Ashiru-Oredope, Magda Hann and Cliodna AM McNulty in Journal of Infection Prevention
Supplemental Material
sj-docx-2-bji-10.1177_17571774211012463 – Supplemental material for Development and pilot evaluation of an educational programme on infection prevention and antibiotics with English and Scottish youth groups, informed by COM-B
Supplemental material, sj-docx-2-bji-10.1177_17571774211012463 for Development and pilot evaluation of an educational programme on infection prevention and antibiotics with English and Scottish youth groups, informed by COM-B by Catherine V Hayes, Charlotte V Eley, Diane Ashiru-Oredope, Magda Hann and Cliodna AM McNulty in Journal of Infection Prevention
Supplemental Material
sj-docx-3-bji-10.1177_17571774211012463 – Supplemental material for Development and pilot evaluation of an educational programme on infection prevention and antibiotics with English and Scottish youth groups, informed by COM-B
Supplemental material, sj-docx-3-bji-10.1177_17571774211012463 for Development and pilot evaluation of an educational programme on infection prevention and antibiotics with English and Scottish youth groups, informed by COM-B by Catherine V Hayes, Charlotte V Eley, Diane Ashiru-Oredope, Magda Hann and Cliodna AM McNulty in Journal of Infection Prevention
Footnotes
Acknowledgements
Thank you to members of the Antibiotic Guardian Youth Badge working group for their support in the development and piloting of this resource: Dr Ryan Hamilton (Antimicrobial Pharmacist, Leicestershire); Steve Morton (Public Health England and West Lancashire Scouts); Clare Liptrott (University of Salford); Faustina Montsho-Hammond (Public Health England); Charlotte Makanga; Neil Mawby (Primary School Teacher, Leicestershire); Lyn Rowe; Amy John; Jodie Sabin; Catriona Innes (formerly NHS Orkney/Girlguiding Orkney); Saba Tyson (Team Leader Science, Greenshaw High School and Akela, 9th Cheam (St Andrews) Scout Group GLSW); Dr Lisa Coulthwaite (Manchester Metropolitan University); Emily Christopher; Karen McKessack; Dr Alicia Demirjian (Public Health England). Thank you to Julie Brooke for her support in survey development and administration. Finally, a big thank you to all volunteer groups, Shaftesbury Junior School and leaders for piloting the programme.
Declaration of conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have worked on development of e-Bug resources and/or the Antibiotic Guardian campaign. The AGYB is not officially affiliated with any youth organisation mentioned in this paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Approval obtained for reproduction or modification of material published elsewhere
Not applicable.
Commercial affiliations
Not applicable
Peer review
Not commissioned; blind peer-reviewed.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.