
Abstract
The operating theatre nurse is responsible for advanced perioperative care in complex environments requiring both technical and non-technical skills. Non-technical skills training can improve teamwork and reduce the risk of adverse events. The Scrub Practitioners' List of Intraoperative Non-Technical Skills (SPLINTS) is a behavioural assessment tool for scrub practitioners not yet translated into Swedish. A Swedish version would provide a common conceptual base and strengthen non-technical skills for Swedish operating theatre nurses. The present study therefore aimed to translate the SPLINTS into Swedish, making it useable in a Swedish perioperative context. A three-round Delphi study was conducted to reach consensus for a Swedish translation. A mean rating of eight or higher on a 10-point scale, assessed as agreement among the experts, was reached in the third round. Although consensus level of agreement was not reached for all elements, three rounds resulted in agreement by a majority. Guidance on Conducting and Reporting Delphi Studies (CREDES) was used as reporting guideline. This Delphi study conducted an important first version of a Swedish translation of the SPLINTS, which, however, needs to be followed by validation and psychometrical testing.
Introduction
The operating theatre nurse (OTN) is a crucial member of the interdisciplinary team responsible for the patient during surgery. In international literature, the term scrub nurse often refers to the person working in the sterile field, whereas the circulating nurse assists outside the sterile area. 1 In Sweden, OTN is a protected professional title for registered nurses with a bachelor's degree and a specialist OT nursing postgraduate diploma. 2 OTNs are responsible for perioperative care and patient safety before, during and after surgical procedures. 3 This requires unique competences not only in, for example, infection prevention and asepsis, instrumentation, and surgical counts, but also in communication and teamwork.3,4 The OTN in the sterile field interacts with the surgeon for the best possible outcome for the patient, but must also rely on an effective teamwork with the circulating nurse, who in Sweden is often a nurse assistant (NA). 4
OTNs view their role as constantly managing risk and preventing harm and attentively navigating the patient through the perioperative process. 5 Preoperative preparation is considered essential for OTNs’ ability to perform safe care. 6 The OTN is expected to use available protocols and checklists to ensure safe care at the same time as working according to evidence-based perioperative practice and knowledge in the professional field.3,5
The technological development in health care is growing, and nurses must combine technological proficiency and caring in their everyday work. 7 OTNs must possess advanced technical skills in the operating theatre and be resilient in challenging situations. 5 However, to ensure patient safety, technical skills have to be complemented with non-technical skills (NTS). 5 NTS consist of cognitive and interpersonal skills, and good non-technical behaviour can enhance safety by reducing the risk of adverse events and patient safety breakdown. 8 OTNs use an extensive number of NTS. 9 Situation awareness is gained through all senses and maintained and shared with the team through preparation, communication and attentiveness. OTNs must co-ordinate teamwork, and thereby reduce communication barriers when solving problems and unexpected situations. 9 For safe and efficient perioperative care, OTNs are consciously using advanced knowledge of the patient, technical equipment and surgical procedure, and stay professionally accountable in the surgical team. 10
The ability of the surgical team to perform NTS is known to affect the teamwork and therefore the safety of the patient. 11 Less team behaviour in surgical care increases the risk of complications and death for patients undergoing surgery. 12 Disrespectful and inaccurate communication patterns are considered a risk to patient safety because they may have a considerable impact on the surgical team. 13 Communication failures can also have other effects, such as inefficiency, tensions in the operation team, waste of resources, delay and inconveniences for the patients. 14
Studies show positive results from training NTS in surgical teams. 15 The Scrub Practitioners' List of Intraoperative Non-Technical Skills (SPLINTS) is an evaluated behavioural assessment tool that contributes to a formative framework for assessment for scrub practitioners. 16 The instrument is designed with a three-level hierarchy with three non-technical skill categories and nine underlying elements. The elements are illustrated with a total of 84 example behaviours for good and poor practices of the NTS to be evaluated (Table 1). 17
The structure of the SPLINTS system. 17

In a Norwegian study, the SPLINTS was shown to facilitate for OTNs when precepting OTN students because consistency with regard to both supervision and observation was promoted by the instrument, making feedback of NTS more systematic and less vague. 18 Reflecting on NTS enhanced awareness of these skills and strengthened team communication, as the SPLINTS became a common vocabulary. 18 The SPLINTS has also been shown to be a useful tool for evaluating the NTS of registered scrub nurses during clinical practice. 19 A significant improvement in NTS, such as situation awareness, management of communication and coping with pressure, has additionally been found for circulating nurses working in operating rooms, after an educational intervention based on the Circulating Practitioner's List of Non-Technical Skills (CPLINTS). 20
The SPLINTS has been translated into Danish and Norwegian, but as yet there is no Swedish version. A Swedish version of the SPLINTS would provide a common conceptual base and constitute a tool for Swedish OTNs and OTN students to strengthen NTS awareness and competences, in accordance with evidence-based practice. A Swedish version of the SPLINTS (SPLINTS-se) would highlight the importance of NTS and their possible impact on the operating teams’ ability to perform safe perioperative care. The present study therefore aimed to translate the SPLINTS into Swedish, making it useable in a Swedish perioperative care context.
Methods
Guidance on Conducting and Reporting Delphi Studies (CREDES) in palliative care was used as a reporting guideline for this study. 21
The translation of the SPLINTS from English to Swedish was made in several steps. The intention of the translation was to reach equivalence between the original version of the SPLINTS and the Swedish version as to semantics, concepts, techniques, criteria and content in both languages. 22 Two bilingual translators were asked by the study authors to conduct a preliminary translation of the original version of the SPLINTS from English to Swedish. This translation draft was then back translated by a bilingual OTN and reviewed by the authors. The back-translated version contained differences in wording and semantics, but there were no major content discrepancies.
To further review the SPLINTS and translate it so it can be used in a Swedish perioperative care context (i.e., to construct a contextualised version of the existing instrument), a Delphi study was performed. The aim of a Delphi study is to reach consensus among the experts involved, through an iterative process of several rounds of surveys. Delphi studies have been used to build systematic consensus in research questions where knowledge is still limited and when expert agreement is of value.21,23 For this study, a traditional Delphi study was performed because it included an expert group with preserved anonymity and consisted of three Delphi rounds with surveys (one for each round) containing both standardised and open-ended questions. As recommended in Delphi studies, feedback to the experts on previous answers and opinions was included from the second survey, and the statistical analysis was descriptive. 24 This study aimed for a response rate of 70% in each survey to enable consensus, as recommended by Sumsion. 25
Together, the first and second authors conceptualised and planned the design. Data collection and analysis was performed via collaboration of the first and second authors.
Sample
The Swedish Association of Operating Room Nursing (in Swedish RFop) is a national association whose aim is to monitor and benefit the professional interests of OTNs, at the same time as also promoting the development of perioperative nursing. 26 The RFop has different councils with elected experienced OTNs committed to the knowledge development in different areas of perioperative nursing. The council members also represent different regions of Swedish perioperative health care, which allowed for capturing regional differences in the translation process. Inclusion criteria for participation in the study were therefore OTN members of the RFop councils for quality, science and teaching. These three councils had a total of 16 council members, and they were all invited through email to participate. One reminder letter was sent out and a total of 10 members accepted to participate. Because participation was voluntary, participants who did not wish to participate were not required to provide a reason. We therefore have no information about why six council members did not agree to participate. To preserve anonymity throughout the Delphi process, the experts were not informed of which other council members chose to participate.
Data collection
All three digital surveys that were part of this Delphi study were designed and constructed by the authors, using Sunet Survey™. A flow chart of the Delphi process and the three digital surveys is presented in Figure 1. The questions in the surveys were based on the original version of the SPLINTS, the Swedish preliminary translation and the translation suggestions emerging from the experts along the process. As a knowledge base, the original SPLINTS was sent to the experts together with survey one. When receiving survey two and three, the experts were sent summary tables containing the English version, the preliminary Swedish translation and all the translation suggestions from previous rounds. No actual pilot study was performed, although the questions of the first survey was reviewed by a specialist nurse with experience from perioperative care and minor revisions were made. The second and third survey was completely based on the answers from previous surveys and therefore not piloted.

Flow chart of the Delphi process.
The first survey was sent out in October 2022, with one reminder letter. The second survey was sent out in December 2022 and required two reminder letters to reach a response rate of 70%. The last survey was sent out in February 2023, with one reminder letter.
In the first survey, the participants were asked to rate the congruity between the Swedish translation of the categories and elements in the SPLINTS and the language used in a Swedish perioperative context, using a 10-point scale. A higher point on the scale indicated a higher congruity. The experts were also asked to freely suggest improvements in the translations. In the second survey, the experts were asked to choose the two most congruent translations from the list of translation suggestions that the experts created in survey one, using the summary table as an aid. The second survey also contained the SPLINTS examples of good and poor behaviour practice for each element, presented in English next to the preliminary Swedish translation. The experts were asked to rate each translation of the 84 examples using a 10-point scale and to freely suggest improvements. In the last survey, the experts were presented with the translation of each category and element chosen by the majority of the expert group in survey two and asked to make a new rating for the chosen translation suggestions, using the ten-point scale. They were also presented with all the translation suggestions for examples of good and poor behaviour practice emerging from survey two and asked to choose the suggestions most congruent with the language used in a Swedish perioperative context.
Every wording and punctuation from the expert groups was included in each following round. Therefore, any indirect or direct influence from the authors on the material or on the experts’ judgement was avoided. Translation suggestions were only excluded when most of the experts agreed on other suggestions.
Data analysis
The consensus definition for the ratings of the translations in this study was set a priori and the threshold was defined as a mean of eight or more on a ten-point scale. The consensus level of agreement (CLA) was set at 80% or more, as suggested by Green et al. 27 CLA was calculated as the percentage of participants who rated each translation at eight or higher of a maximum of 10 points. Consensus for choosing translation suggestions was considered based on an expert majority voting. The ratings of translations of categories, elements and example behaviours were analysed with descriptive statistics.
Missing data in survey one and two were replaced by a plausible value based on multiple imputation (MI) values. 28 Means were calculated on the imputed dataset for rating elements and example behaviour practices in survey one and two. The standard deviation (SD) was calculated computing the average of the standard deviations from the imputed ratings. SD was used as a supplementary measure of the spread of the responses, with a lower SD indicating a higher certainty of consensus. MI was not used in the CLA calculation and not in survey three, as a result of only two missing variables in the rating of categories. Here, missing data were instead replaced by the mean of the other ratings and rounded down. There were no missing data in the ratings of elements in survey three. One participant did not rate any of the example behaviour practices in survey two and the missing data were excluded from the analysis. Numerical rating was analysed using SPSS, version 28 (IBM Corp., Armonk, NY, USA).
Ethical considerations
According to the Swedish Ethical Review Act, ethical approval for studies within the framework of higher education is not mandatory29,30 However, the recommendations regarding information and consent were applied in this study. Permission to send out invitations to the RFop council members to participate in this study was obtained from the president of the RFop. Permission to translate the original SPLINTS version was obtained from one of its original authors (Professor Rhona Flin). All Delphi participants signed a written consent form and were informed of the right to withdraw their participation at any time without giving a reason. A written consent for storing personal data according to the European Union directives of the GDPR act was also applied for all Delphi participants.
Results
The demographic data of the expert group confirms a long clinical experience with a median of 16 years in clinical practice. The majority of the experts were also currently involved in precepting OTN students or colleagues (five of 10), OTN education (seven of 10) and development work in perioperative care (eight of 10). The experts had a large regional representation. Six of the ten experts had heard of the SPLINTS prior to this study.
Round one
The first Delphi survey had a response rate of 100%. The means and the CLA for the experts’ ratings of the translation of categories and elements in the surveys of rounds one and three are presented in Table 2. Missing variable value (i.e., no rating) were replaced by MI data for five missing ratings of elements in survey one.
Ratings of translations in the surveys in round 1 and round 3.

*In round 2, the expert group replaced the element co-ordinating with others by teamwork.
**The rating and the CLA for Task Management in round 3 are based on the number of participants whose translation suggestion was chosen by the majority
Abbreviation: CLA = consensus level of agreement.
The expert group presented 14 alternative translations for the three categories and 43 alternatives for the nine elements (Table 3). The translation suggestions were evenly divided between the three categories. Nonetheless, most of the translation suggestions for elements emerged in the Situation Awareness category (37%) and in Communication and Teamwork (42%). The elements gathering information and acting assertively both had eight suggestions, indicating a disagreement with the first translation. Acting assertively also had the lowest mean rating with 5.7. Anticipation and providing and maintaining standards only generated two alternative translations each, and this correlated with a high mean rating. Many translation suggestions were recurrent; for example, whether it should be called operating room or operating theatre. Other suggestions focused on verbs such as “recognise” or “perceive”. For acting assertively, suggestions involved the translations “being safe enough” or “being confident enough to ask for clarification”. The first preliminary translation did not meet the CLA of 80% for any category or element, indicating a disagreement with the first translation among the experts.
Number of translation suggestions for categories and elements from the survey in round 1.

In survey one, the experts were asked if any NTS were missing in the English version of the SPLINTS that would be suitable for Swedish perioperative care. One participant wanted to add “Stress Management”, “Managing Fatigue” and “Leadership” as categories. Regarding elements, one participant suggested “non-verbal communication” under the category Communication and Teamwork. No further suggestions were added by the participants.
Round two
Round two had a response rate of 80%. The survey in round two was a two-step process. First, the experts chose the most congruent translations among the 57 translation suggestions from round one for categories and elements. Majority agreement was reached in all nine elements and two of three categories (i.e., all except Task Management). Because majority agreement was not reached for Task Management, the two most chosen translations were placed in the third survey for further evaluation. Most of the experts ranked the translation suggestion that proposed a change of name for the element co-ordinating with others into “teamwork” highest and the name was therefore changed.
The second step in round two was not only to rate the translations of the 84 example behaviours for good and poor practice, but also to suggest translation improvements. The means and the CLA of the ratings are presented in Table 4. Missing data (i.e., no rating) were replaced by MI data for seven missing ratings of example behaviour practices in survey two. The experts gave 111 translation suggestions in 58 out of 84 example behaviours for practice (Table 4). Even though the experts had many suggestions, the suggestions often concerned the change of single words, whereas the content was left intact. For the example behaviour listening to instructions, the translation suggestions covered different wordings, such as: “does not understand”, “does not absorb” or “cannot listen to instructions”. For the example behaviour fails to listen to conversations between other members of the team, suggestions involved: “does not understand conversations”, “is not paying attention to conversations” and “does not pay attention to information exchange”. A mean rating between 6.0 and 7.89 indicates some agreement with the translation of the examples of behaviour practices although not at the set consensus level of eight or more. The combined average (mean) rating of all example behaviours for good and bad practice was 6.94. A CLA of 80% was not reached for any translation of example behaviours for good and poor practice.
Ratings of example behaviours for good and poor practice from the survey in round 2.
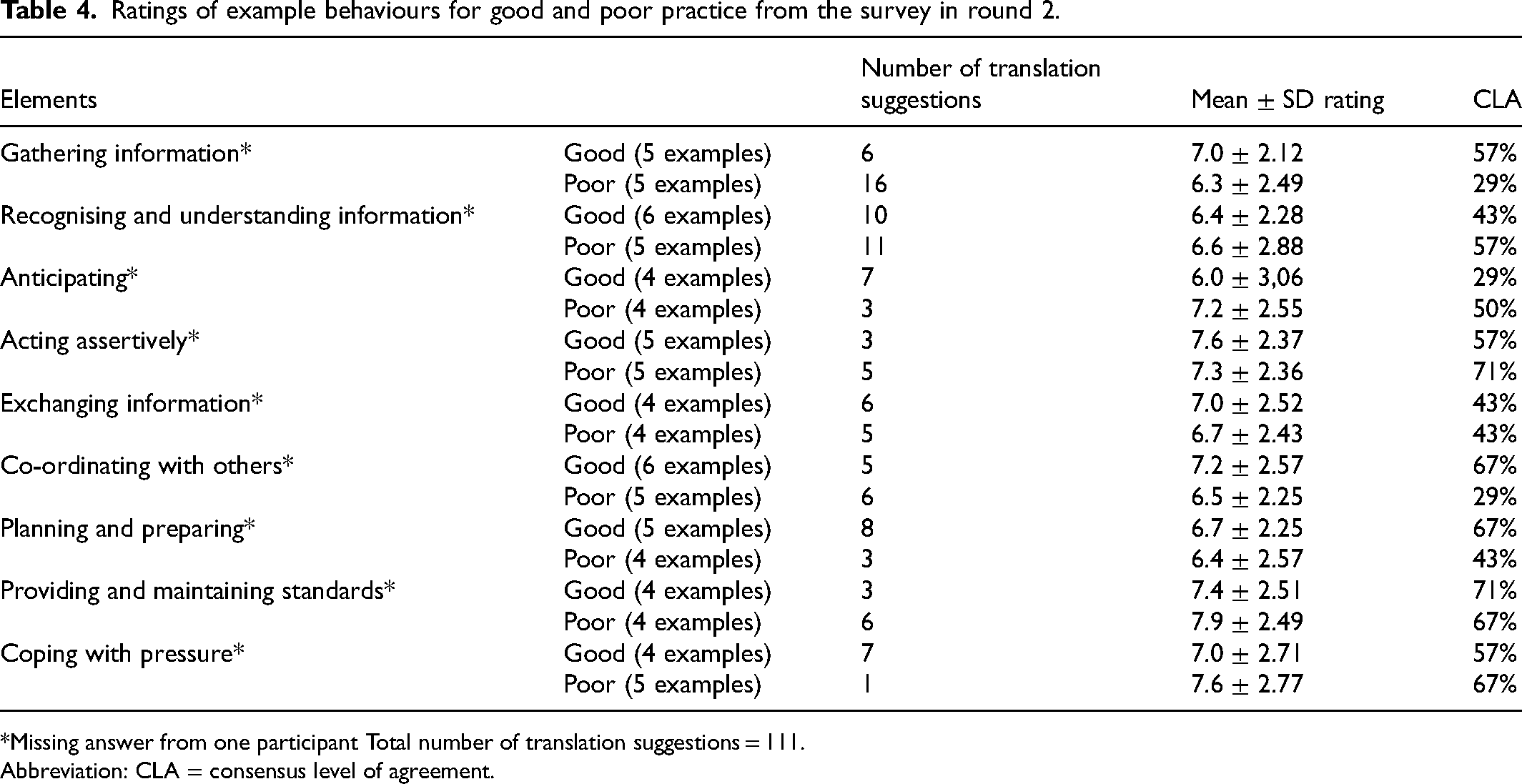
*Missing answer from one participant Total number of translation suggestions = 111.
Abbreviation: CLA = consensus level of agreement.
Round three
Round three had a response rate of 70%. Majority agreement for the translation of Task Management was reached in survey three, since five experts chose translation one (mean rating 8.4) and two experts chose translation two (mean rating 9.0). The mean rating for categories and elements in the third survey is compared to the rating in the first survey (Table 2). The CLA of 80% can be seen in all categories and in three of nine elements. A mean rating of eight or more can be seen in all categories and elements, and the results in the third survey show that the experts strongly agree with the translated version of the SPLINTS for categories and elements. Teamwork had a lower CLA, but all experts rated the translation ≥7, indicating high agreement despite not reaching the CLA of this study.
The mean ratings for the translations increased for all categories and elements when comparing to the ratings in survey 3. The most substantial increase was seen in the Communication and Teamwork category, with the element acting assertively increasing 2.9 in mean rating between the first and the third survey. The element planning and preparing had the second biggest increase with 2.6 in mean rating. In the third Delphi round, CLA was reached for all categories but only for three of nine elements. A CLA of 80% was not reached at all for any translation of example behaviours for practice. A mean rating between 6.0 and 7.89 was seen after the first rating for the example behaviours for practice. The experts agreed on the translation of 82 of 84 example behaviours for good and poor practice. Consensus for a Swedish translation of the example behaviours of fixates on one task and organises equipment could not be determined based on the three-round Delphi technique.
Discussion
The Delphi process resulted in numerous translation suggestions from the experts, indicating a strong commitment to the Delphi process but also a disagreement with the first Swedish translation draft. Most translation suggestions emerged for the elements and for the examples of good and poor behaviour practices regarding gathering, recognising and understanding information. That result is in line with other studies of OTNs’ use of NTS. OTNs find it essential to secure accurate preoperative information about the patient and the surgical procedure, to be prepared for the work. 13 Interdisciplinary discussions perioperatively and a shared understanding in the team are also described as fundamental. 13 This might explain the experts’ thoroughness when it came to the translation of the elements and the example behaviours regarding information being correct. The importance of preparation for OTNs is further shown in that the examples of good practices for planning and preparing received eight translation suggestions. Enhancing skills in Situation Awareness, using a Swedish version of the SPLINTS, could improve safer information transfer and organised pre-operative planning.
In the category Communication and Teamwork, the element of acting assertively received the most translation suggestions. A study shows that OTNs’ confidence in their personal skills is necessary for effective collaboration with the surgeon and that high standards of professional skills are important for promoting patient safety. 31 Experience enhances OTNs’ ability to speak up, make decisions and solve problems. 6 A structured use of the SPLINTS could contribute to building NTS experience and confidence for OTNs, thereby strengthening safety for the patient in perioperative care.
Education, training, responsibilities and task assignments for OTNs vary between countries and work settings 32 and can affect the compatibility between a behavioural tool for English OTNs and the role of the Swedish OTN. The Swedish OTN is responsible for the entire perioperative period and not just the intraoperative phase, as is the case of the scrub nurse.1,4 Sirevåg et al. 10 suggest a new and expanded behavioural marker system for evaluating the NTS of OTNs that also includes, for example, ethical competence and professional accountability. A Swedish version of the SPLINTS, however, can be a valuable tool to evaluate and strengthen NTS during the intraoperative period for Swedish OTNs. The translation can contribute to a common terminology and be adapted to future behavioural marker systems that cover the entire perioperative period.
The expert group consisted of dedicated OTNs with clinical experience of being involved in precepting, clinical development and education of OTNs. This makes the expert group well representative of the profession. Moreover, the broad regional representation of the experts made it possible to capture language and wording used in all parts of Sweden. The expert group was purposely sampled based on inclusion criteria, which is standard in Delphi studies. 33 When interpreting the results, it is necessary to be aware of the risk inherent in the Delphi method, namely that experts move towards consensus because they want to agree with the majority of the panel. 34 The feedback from other panellists, on the other hand, can also encourage members of the expert group to see other more relevant issues and opinions and therefore change the experts’ minds. This must be taken into consideration and be seen as a potential threat to validity and reliability within the Delphi method. 34 External validation of the final version is recommended 21 and would be the next step to validate the SPLINTS-se.
Methodological considerations
The use of expert consensus in the Delphi process is important when generating guidance for good healthcare practice, but the quality is dependent on the rigour of the application and reporting. The transparency of the reporting of this study was enhanced due to the use of the CREDES reporting guidelines. 21
When comparing this Delphi study to the quality assessment of Delphi studies according to Jünger et al., 21 the present study had a defined purpose and a clear rationale for the use of the Delphi technique. The selection of experts was justified since the expert group consisted of OTNs with long clinical experience and a clear commitment to improve perioperative care. However, the reliability in this study could be considered limited due to the small expert group (n = 10). A larger response group could have reduced the risk of judgements being affected by personal bias and could have enhanced transferability. The preserved anonymity and the feedback of data from previous surveys did, however, help maintain reliability. The method description in this study included a flow chart with a presentation of the surveys. 21
Due to the small number of participants in this study, each missing variable could constitute a large percentage that could reduce the precision of the ratings. By using MI values, uncertainty in missing data was replaced by a plausible value. 28
The surveys for rounds one and two were extensive. The number of translation suggestions to rank and decide about could have impaired the quality of data because the experts might have had difficulties completing surveys in time or experienced response fatigue. However, the dropouts in this study were few and the response rate of 70% or more in all rounds strengthens the validity and reduces the risk of response bias affecting the result.25,33
The result of a Delphi study must be carefully considered because consensus is a measure of agreement and agreement does not automatically mean that the most correct answer has been found. 34 An additional fourth round could have increased the quality of the translation because the experts were only able to rate the example behaviours for practice once. The translation of the instrument has been rigorous, through a three-round Delphi study. However, it was not enough to determine consensus on the last level, namely translations of 84 examples of good and poor practice.
According to the CREDES guidelines, it is recommended to review the final version of the results by external validation. 21 The first Swedish version of the SPLINTS-se could be followed by psychometric testing and revisions before full implementation in clinical practice. To further strengthen the translation of the SPLINTS-se, a survey identifying non-technical skills for Swedish OTNs, could establish that the suggested version covers all necessary skills in the Swedish perioperative context.
Conclusions
This Delphi study was a first step towards translating the SPLINTS as correctly as possible into Swedish and make the instrument usable in a Swedish perioperative context. The experts did not reach consensus for the translation of all parts of the SPLINTS system. The translation process through a Delphi process was thorough and rigid, however, with increasing consensus levels of agreement and mean ratings of the translation throughout the Delphi rounds. There is much to suggest that the SPLINTS-se will be a useful tool in the effort to develop NTS for Swedish OTNs and that it could be part of the curricula in OTN education, thus making it likely to strengthen safer perioperative care. However, the translated Swedish version needs further validation.
Supplemental Material
sj-pub-1-njn-10.1177_20571585251335631 - Supplemental material for A three-round Delphi study to translate the scrub practitioners’ list of intraoperative non-technical skills (SPLINTS), for use in a Swedish perioperative context
Supplemental material, sj-pub-1-njn-10.1177_20571585251335631 for A three-round Delphi study to translate the scrub practitioners’ list of intraoperative non-technical skills (SPLINTS), for use in a Swedish perioperative context by Katarina Göransson and Anne-Marie Wangel in Nordic Journal of Nursing Research
Supplemental Material
sj-docx-2-njn-10.1177_20571585251335631 - Supplemental material for A three-round Delphi study to translate the scrub practitioners’ list of intraoperative non-technical skills (SPLINTS), for use in a Swedish perioperative context
Supplemental material, sj-docx-2-njn-10.1177_20571585251335631 for A three-round Delphi study to translate the scrub practitioners’ list of intraoperative non-technical skills (SPLINTS), for use in a Swedish perioperative context by Katarina Göransson and Anne-Marie Wangel in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We sincerely thank the experts of the RFop for their generous contribution and dedication to the Delphi process of translating the SPLINTS, for use in a Swedish perioperative context. We also thank Katarina Graah-Hagelbäck for excellent language review.
Author contributions
KG and AMW were responsible for the study design, data collection, data analysis and preparing the manuscript.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
According to The Swedish Ethical Review Act (SFS 2003:460; SFS 2024:232) ethical approval for studies within the framework of higher education is not mandatory and not performed in this study. Respondents gave their written consent for review and signature before starting survey participation. A written consent for storing personal data according to the European Union directives of GDPR-act was also applied for all Delphi participants.
Funding
No financial support was received for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.