
Abstract
The aim of this study was to describe operating theatre nurses’ experiences of teamwork within the surgical team in regard to achieving patient safety. Safe surgery for patients is based on teamwork in a safe modus between the members in the surgical team. Operating theatre nurses contribute to safe surgery by professional perioperative nursing activities and by participation in teamwork in the surgical team. A qualitative descriptive design using narrative interviews with 16 operating theatre nurses in Sweden was chosen for increased understanding of their experiences of teamwork in regard to achieving patient safety. The findings are presented in three themes, illustrating teamwork in regard to achieving patient safety between the operating theatre nurses’ and other professionals in everyday situations. From the operating theatre nurses’ narrated experiences of teamwork, person-centred nursing care, interdependent collaboration and familiarity of the professionals’ skills contributed to safe surgery. A brief meeting, unfamiliarity of professionals’ skills, uncontrolled tantrums and experiences of exclusion were experienced as counteractive to patient safety. The operating theatre nurses managed demanding situations by diverse strategies to restore patient safety.
Introduction
Team-members’ perceptions of teamwork are related to the quality and safety of patient care.1–3 Surgical team-members strive to achieve a successful perioperative care, in absence of preventable and unnecessary harm to patients. 4 Surgical team members possess the required professional competence for a safely-performed surgical intervention, they collaborate and strive for an environment of patient safety. 5 Every surgical patient has the right to the highest quality of perioperative nursing care for achieving the expected outcome of the care given. 6 Operating theatre nurses (OTNs) in the surgical team contribute to patient safety during surgery by professional perioperative nursing activities as caring for patients’ wellbeing and infection control and by participation in teamwork in the surgical team. 7 Hence, teamwork involves professional competence regarding both technical and non-technical skills.8,9 Still, research illustrates that flaws in teamwork within surgical teams occurs,10,11 despite the fact that teamwork has been improved after the implementation of the surgical safety checklist. 12
Members in the surgical team
Professionals in a surgical team may vary according to the healthcare system in different countries. The professionals in a surgical team in Sweden are the operating theatre nurse (OTN), the nurse anaesthetist, the surgeon, the anaesthetist and the nurse assistant (NA). They all have different levels of educational backgrounds.13,14 However, the role of the instrument and the circulating nurse is always needed, and the circulating nurse role is mostly performed by a nurse assistant. All team-members are responsible for the patient’s care and each member is competent within their own specific area of expertise. The patients are also regarded as team members as they have expertise of their own health situation and requests. 15 While working with each other, all team-members contribute to the outcome of the operation. Yet, surgical teams may be seen as a multiprofessional team, that is, a team where members are working in parallel and with a low degree of integration and relatively independent of each other, but have coordination of actions. 16
Patients in perioperative care
Patients meet various professional caregivers in diverse care units for preparation, treatment, recovery and rehabilitation in regard to the operation. This may cause inconsistencies and lack of information between the different caregivers.17,18 Consequently, patients may not be appropriately prepared for their operation. It is vital that patients understand the information given beforehand in order to be physically, mentally and socially well-prepared for surgery. 19 When person-centred care is applied, patients take an active part in their care together with professional caregivers, as in a partnership.20,21 Patients should meet OTNs for perioperative interviews about healthcare aspects, 22 which is not a regular feature today in Swedish health care.
Teamwork in the surgical team
Teamwork has been defined by Xyrichis and Ream 23 as a dynamic process where health care personnel have complementary backgrounds and skills. The members are sharing common health goals and coordinates patient care, from assessing to evaluating. To accomplish teamwork, the members have to have interdependent collaboration, open communication and shared decision-making. 23 According to Sandberg,24,25 teamwork consists of essential qualities, structural qualities and process qualities, where synergy and goal-orientation is important for efficient teamwork and to achieve a mutual understanding of the goal.24,25 Different perceptions regarding the goal of patient care may cause disagreements, and an inadequate communication can adversely affect teamwork.26,27 Flaws in communication can be present at all organizational levels of care, 28 and the effects may result in inefficiency, waste of resources and delays, and may even result in operating on the wrong patient or on the wrong part of a patient’s body. Poor communication can also lead to tension within the team, negative experiences and patient discomfort. These shortcomings are often due to communication taking place too late, or that communication is either incomplete or incorrect.11,29 According to Makary et al., 30 members of surgical teams tended to value teamwork in different ways. Surgeons reported high scores for satisfactory teamwork compared to other team-members who were less satisfied, and OTNs reported low scores in teamwork with the surgeons. There is little research found regarding experiences of teamwork in surgical teams from the perspectives of the OTN.
Aim
The aim of the study was to describe operating theatre nurses experiences of teamwork within the surgical team in regard to achieving patient safety.
Method
A qualitative descriptive design with narrative interviews and a content analysis was chosen for increased understanding of OTNs’ experiences of teamwork. The method was chosen to get rich and meaningful information from the interviewees, 31 and aspects of teamwork in regard to achieving patient safety. 32
Participants
A convenient sampling of 16 participants was chosen for the study. The inclusion criteria stated that at least two years of work experience was required as an OTN in a Swedish Operating Theatre (OT) department. 33 Clinical managers and clinical OTNs from four hospitals in central Sweden were informed about the study, both written and orally. Thereafter, 16 OTNs voluntarily contacted the authors for participation. The OTNs represented two hospitals in urban and two hospitals in rural regions. All participants were women aged between 36 and 64 years who had worked with OT nursing for a period of 7 to 34 years. This involved abdominal surgery or/and orthopaedic surgery.
Data collection
The data collection was conducted between September 2011 and January 2012, with the use of narrative interviews, which were digitally recorded by the first author (AS) in a separate room at the participants’ workplace during working hours. The interviews began with the key question: ‘Please, tell me about your experiences of teamwork within the surgical team to achieve patient safety?’ Follow-up questions were asked, for example, ‘What do you mean or can you describe more fully?’ It was important that narratives were concrete and brought up experiences that the OTN faced on a daily basis. 31 The interviews lasted between 53 and 134 minutes. The interviews were transcribed verbatim by the first author (AS).
Data analysis
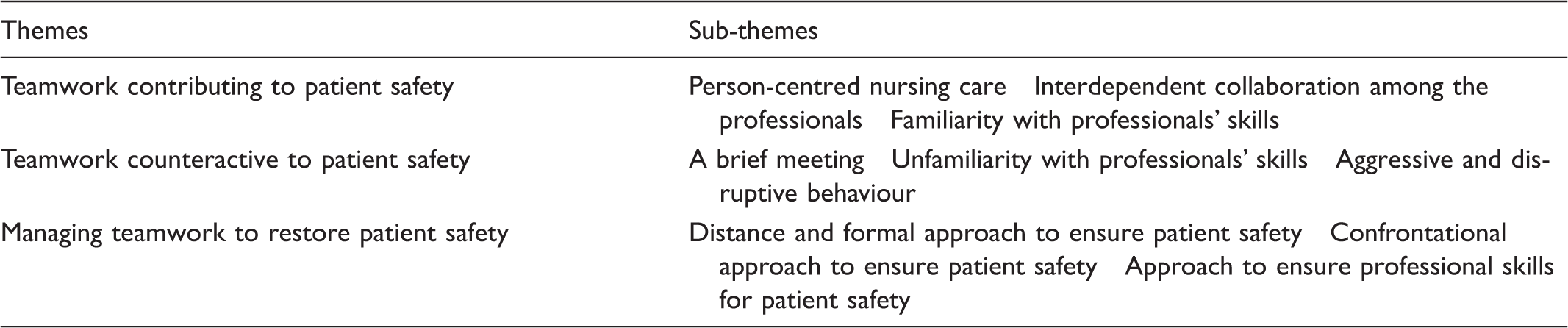
Themes and sub-themes.
Ethical considerations
The study was conducted in accordance with the World Medical Association Declaration of Helsinki, 2008, 34 and approved by the regional ethics committee (Reg. No. 2011/784–31). Documents for informed consent were signed by each participant before the interview was initiated. Confidentiality was secured by identification numbers on the audio recordings and on the documents of the interviews, and no one except AS had access to the list of names and ID numbers. 35
Findings
Teamwork contributing to patient safety
Person-centred nursing care
Operating theatre nurses used a person-centred approach in the preoperative interview with the patient, when there was time and opportunity for a preoperative meeting outside the OT department. This partnership focused on the patient’s perioperative needs, and created a relationship with continuity. The patients were encouraged to describe their situation and their strengths and requests regarding the operation. The nurses explained about aspects having previously been unclear that then became clear, and an adequate care plan could be completed. The experience of deeper understanding of patients’ situation facilitated OTNs to be better prepared for safe nursing care. When the patients met the nurses again in the operating theatre (OT), they expressed feelings of joy, confidence and a sense of calmness. When you have had interaction with the patient before the entrance to the OT: We say hi, … and you notice that the patient is much calmer, it is not like they are meeting an alien, I am somebody familiar to the patient. (P12)
Interdependent collaboration among the professionals
Interdependent collaboration with surgeons was reached when OTNs experienced respect as equal co-workers and were involved and engaged as key partners, and spoken to with respect for their professional skills. OTNs focused on collaboration with surgeons, to facilitate their surgical performance for a good outcome for the patients. The collaboration of the OTNs and the nurse assistants (NA) was characterized by leadership and the NA was perceived as the OTNs’ ‘right hand’. The OTNs were familiar with NAs range of competence in nursing care, as they had been taught at the OT department to conduct the circulating nurses’ duties. Despite NAs’ little formal education, they had learnt to collaborate through work experience. When dressed in sterile clothes, OTNs were totally dependent on NAs willingness to collaborate. This was vital in order for the OTNs to supply surgeons with the correct equipment at the right time. OTNs believed that friendly leadership was necessary in the collaboration as this would generate a willingness to follow OTNs’ instructions efficiently. Interdependent collaboration was met when the OTN and the nurse anaesthetist expressed their goals and nursing care actions for mutual understanding before surgery. OTNs wanted to have a continuous communication with nurse anaesthetists during the intraoperative phase to be aware of any possible critical situation. This was easier met when the nurse anaesthetist was familiar to the OTN. It’s important to have good collaboration with the nurse anaesthetist. It’s something that we always have during the morning meetings in the OT … if there is a high risk of bleeding we have already discussed that …. (P7)
Familiarity with professionals’ skills
Familiarity with team-members’ professional skills created trust and efficient teamwork by nonverbal communication. Such teamwork was experienced as constructive, and this was based on OTNs’ professional competence, experience and understanding of each surgeon’s different surgical techniques. A continuous overview of the surgical site was required in order to follow the surgeons’ technique and to always be supportive and one step ahead. In such situation the operation ran smoothly and efficiently and in consensus. The surgeon communicated his requests through small gestures and movements by a hand or fingers: … the surgeons never have to say anything because the OTN sees and knows what they want or the OTN gives advice, because OTNs must understand what the surgeon is doing and then think one step ahead. (P9)
Teamwork counteractive to patient safety
A brief meeting
In general, however, the nursing care-plan was based on OTNs’ personal experience, general routines and a brief reading of each patient’s medical record. OTNs strived for an interview with the patient immediately before surgery in the operating theatre for a brief data-collection. Even though the OTNs had not met the patient before, they described the importance of showing empathy towards patients and their situation. They tried to establish a reassuring atmosphere, by for example, staying close to an anxious patient or providing physical touch to encourage a sense of calm and confidence.
Unfamiliarity with professionals’ skills
Multiprofessional work in the surgical team was also experienced by the participants, and this occurred for example when OTNs encountered new team constellations and unfamiliar surgeons. This was especially apparent in urban areas, due to high staff turnover and rotations in different surgical specialties. Not being acquainted with surgeons had a negative effect on teamwork, especially surgeons who repeatedly asked for an instrument despite the fact that the nurses knew what was needed. When an OTN was not familiar with a surgeon she judged his professional skills, and future teamwork was based on this knowledge ‘… after all, one operation is enough to see how they work’ (P11). However, teamwork could be extremely demanding when an inexperienced NA joined the team and this resulted in a double workload, both intellectually and emotionally for the OTN. When all team-members were unfamiliar in the team, this was experienced as hazardous and an extremely demanding workload by the skilled OTN.
Aggressive and disruptive behaviour
OTNs experienced feelings of humiliation when surgeons’ behaviour and communication were perceived as disrespectful. The commitment decreased when surgeons were neither reliable nor skilful in their work. Such situations led to feelings of guilt towards the patients, as the OTNs felt they had not protected them well enough. Sometimes surgeons were unable to control their tantrums with consequences of other team-members’ knowledge and skills tended to decrease because of the strained atmosphere.
Feelings of humiliation arose when the surgeon’s failed to listen to the OTNs: A sponge was missing […] I said it’s in the patients’ body. We had searched the waste bags three times. Then he x-rayed very carelessly. I said it is in the patient. NO, he yelled […] but in the end, he just closed the wound […]. (P3)
Managing teamwork to restore patient safety
Distance and formal approach to ensure patient safety
OTNs’ experiences of managing the surgeons’ uncontrolled aggressive outburst were explained as different strategies. They were focused on trying to deal with the on-going situation and to restore patient safety. One strategy was to become silent and formal. Another strategy was to become distanced and to communicate only when spoken to and focus on necessary actions for patient safety.
Confrontational approach to ensure patient safety
When patients were awake, OTNs prevented any forms of argumentation within the team, because of patients’ sensitivity to the atmosphere in this vulnerable situation ‘… and I said we discuss this later … or if I was wearing sterile attire, I just signalled with a hand or with gestures mark to shut down’ (P 15).
The strategy of the OTN in situations of surgeons’ uncontrolled tantrums was sometimes to confront the surgeon and clearly inform that such behaviour was not acceptable. They used such an approach to calm the surgeon down and made co-workers felt more at ease and re-establish patient safety.
Approach to ensure professional skills for patient safety
Furthermore, when OTNs experienced surgeons who were not persuaded to listen to advice when a risk of injury was exposed, or when OTNs were denied to call for a more competent surgeon, a secret quiet signal, for example a hand formed as a telephone was given to the NA to contact another experienced surgeon. This was done to ensure the patient’s right to professional surgery.
In order to be able to trust unfamiliar or inexperienced NAs, OTNs interrogated them about nursing knowledge and skills. This was necessary for the planning and the performance of nursing care, and involved guiding in a polite and friendly way to do the right thing at the right time, in order to maintain patient safety. In urban regions, situations such as these occurred quite often, and OTNs were expected to have total foresight and rigorous planning.
Discussion
Teamwork for patient safety
In this study, the operating theatre nurses regarded person centred preoperative interview as a prerequisite for safe nursing care as contributing to patient safety during surgery. A mutual agreement about the intraoperative care appeared when OTNs had met the patient during the preoperative phase outside the OT, similar to Ekman et al. 20 who explain about person-centred nursing care, but in the whole process of care. OTNs could work more appropriately according to the nursing process and the national guidelines for OT nurses. 22 The participants in this study described teamwork for contributing to patient safety during surgery as based on a deeper personal knowledge about each other’s professional behaviour and skills by regularly working together as a team. They could follow the procedure and therefor anticipate and plan more thoroughly and precise for actions. It may be as Gillespie et al. 36 shows; when working in established, specialized teams, a familiarity is understood between team members’ professional skills and behaviour. Alfredsdottir and Bjørnsdottir 37 pointed out when OTNs were divided into specialist teams, high levels of knowledge and skills were achieved. In such teams, according to descriptions by participants in this study, the communication was open and respectful which led to a mutual understanding of the care planned. This is emphasized by Sandberg, 24 in that teamwork involves synergy and goal orientation.
In this study, the OTNs expressed that patient safety was present even when the teamwork consisted of nonverbal communication such as eye contact, a nod of the head, or when other quiet signs such as hand movements occurred. This harmonizes with findings of other studies concerning teamwork.38,39 The participants in this study described how they often followed the surgeons’ technique with the use of nonverbal communication and by maintaining an overview of the surgical wound, in another study explained as ‘a watchful eye’ and clinical wisdom. 7 Silent teamwork may also demonstrate that team members are familiar and comfortable in their professional roles and relationships, as stressed by Bleakley et al. 10 and Weldon et al. 40 Bleakley et al. 10 further describes that acquainted team members rely on tacit knowledge and habitual routines developed from an understanding of each other’s working styles to maintain situation awareness. Other team members may not be initiated into this silent communication or tacit knowledge, and silent communication must therefore be shared verbally in the team for updating the situation. For that reason, it is important to implement reconciliations regularly in accordance with the surgical safety checklist. 5
Counteractive teamwork and management
In this study, OTNs’ experiences of counteractive teamwork existed since preoperative interviews with patients outside the OT rarely occurred, despite the participants expressions that these meetings with patients resulted in a good caring relationship with continuity for the patient, also depicted by Rudolfsson et al. 41 and Sjöstedt et al. 42 Due to time pressure, the usual routine was based on OTNs’ brief reading the medical record and a brief conversation for data-collection with the patient immediately before surgery, in line with Kelvered et al. 7
The OTNs’ experienced counteractive teamwork when team-members were not acquainted, and risks of misunderstandings increased, in line with Cochran and Elder 43 and Higgins and MacIntosh. 44 According to the participants in this study, such multiprofessional teamwork was often caused by rotations between different surgical units, types of patients, surgeons and varying surgical procedures and techniques, also described in a recent study. 38 This may lead to unorganized teamwork in the surgical team, as the anaesthesia staff and the surgical staff have their own sub-teams’ perspectives on care delivery instead of being united for a common goal. 45 Therefore, team-training including teamwork in OTs for achieved mutual understanding of the goal should be a part in educational programmes for nurses and physicians, as described by Wallin et al. 46
The OTNs in this study assessed the competence of unfamiliar team members, and such knowledge was necessary for the ethical judgement about their professional skills to ensure the patient’s right to safe care. For example, the OTNs called for a more experienced surgeon to assist or to take over the procedure if the surgeons’ skills were assessed as untrustworthy, something also stressed by Kelvered et al. 7 The participants expressed feelings of guilt and shame towards the patient when they had been unable to prevent a surgeon from performing poor surgery. Such statements of ethical character have not been found in earlier studies.
Working together with surgeons who could not control their stress, OTNs described how they considered whether to interrupt or not, since a poorly adapted interruption could start uncontrolled outbursts, this was described already in 1967 by Stein. 47 Surgeons losing their temper and speaks to OTNs in a disrespectful way resulted in ineffective and unsafe teamwork. Surgeons’ emotional outbursts led to tension within the entire surgical team, setting the patient safety at stake, as described by the participants in this study, and in other studies.43,44,48 Mazzocco et al. 3 explains such behaviour as poor teamwork with a higher risk of patient mortality or morbidity. The participants, in this study, strategic responses to this kind of behaviour were to become distanced and quiet, also depicted by Gardezi et al. 27 Another strategy, as they narrate, was to force oneself to cope with the situation and do whatever was necessary, also mentioned by Higgins and MacIntosh 44 and Rogers et al. 48 Probably, according to the OTNs described strategies of aggressive outburst in this study, the best choice to calm down the situation was in a clear and direct manner inform the surgeons of this unacceptable behaviour. A working climate characterized by emotional pressures could be extremely demanding and may affect health and well-being.24,43
This study has limitations, for example male OTNs or less experienced OTNs could have added other aspects to the result. The findings in this study were based on the OTNs’ narrated experiences of teamwork in regard to achieving patient safety from their point of view, and the other team-members were not provided any opportunity to express their experiences. 32 Some aspects may consequently have been lost or not made clear because of the authors’ insider perspective. However, continuous discussions between the two authors led to increased scrutiny and trustworthiness of the study. Findings from the study cannot be generalized and applied to other contexts but may be recognizable to other female OTNs in a similar context. 49 Further studies are needed to explore teamwork from other surgical team-members’ perspective on patient safety and the organizational impact on teamwork.
Concluding comments
From the OTNs’ narrated experiences of teamwork in regard to achieving patient safety, person-centred nursing care, interdependent collaboration and familiarity of the professionals’ skills contributed to patient safety. A brief meeting, unfamiliarity of professionals’ skills, uncontrolled tantrums and experiences of exclusion were experienced as counteractive to patient safety. OTNs managed demanding situations by diverse strategies to restore patient safety.
Footnotes
Acknowledgments
We sincerely thank the operating theatre nurses who shared their experiences of teamwork in the surgical team for new knowledge from their perspective.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.