
Abstract
Objective:
Although numerous studies have assessed patient satisfaction in diverse settings, in the realm of nursing surgical care, standardization of measurement for patient experience and satisfaction is lacking. Therefore, the aim of this study was to assess the satisfaction of surgical patients with perioperative nursing care.
Method:
A descriptive cross-sectional survey was conducted. Sociodemographic characteristics and clinical data were recorded. Patient satisfaction was measured with a modified version of the La Monica–Oberst Patient Satisfaction Scale (LOPSS-12).
Results:
150 patients (73 women, 49% and 77 men; 51%) completed the survey. The mean age was 63 years (standard deviation, 16 years). The mean overall satisfaction score on the La Monica–Oberst Patient Satisfaction Scale was 3.17 (standard deviation, 0.21). The scale showed adequate content validity (Lawshe’s Content Validity Index was 0.76) and moderate reliability (Cronbach’s alpha = 0.70). Two variables—patient sex and the presence of comorbidities—were significantly associated with overall satisfaction: men and patients with comorbidities were more satisfied with the care received. Patients with university studies were significantly more likely than patients with less education to consider nurses “impatient,” but also considered the nurses’ advice to be “useful.” Patients with hospital-acquired complications were more likely to perceive nurses to be “more interested in completing tasks than in listening,” although they also felt that nurses worked “conscientiously.”
Conclusion:
Overall, patient satisfaction with perioperative nursing care was good. This study identified several areas of nursing care in need of improvement, particularly the need to spend more time with patients and to keep them better informed about the perioperative process. The modified La Monica–Oberst Patient Satisfaction Scale is suitable for measuring surgical patient satisfaction with perioperative nursing care. The findings presented here may be of value to nursing administrators, educators, and nursing care providers to improve patient satisfaction and to develop strategies to prevent patient dissatisfaction.
Keywords
Introduction
In the context of population aging and the attendant rise of complex chronic diseases, it is essential to continue improving the quality of healthcare services. The impact of individual healthcare professionals on the experience of hospitalized patients can be effectively measured by examining the quality of care received, 1 commonly through patient experience surveys. 2 Satisfaction with care is a key component of the patient experience, and numerous accreditation organizations—including the European Foundation for Quality Management (EFQM), the Joint Commission on Accreditation of Hospitals (JCI), the International Organization for Standardization (ISO), and the Magnet Recognition Program®—consider patient experience and satisfaction to be a key indicator of care quality.3,4
Although substantial research has been performed to investigate patient satisfaction with healthcare, few studies have investigated nursing care through the whole perioperative process. Moreover, most of the studies that are available were conducted more than 20 years ago. Given the substantial changes in surgical departments in the past decade, particularly the change in focus from task-centered care toward a more patient-centered care approach with an increased emphasis on outcomes of the quality of care, 1 it is important to assess the current status of perioperative nursing care. In this regard, a review conducted by Heidegger et al. 5 concluded that few studies have been performed to evaluate quality of care from the patients’ perspective in perioperative care environments.
The perioperative period comprised three different time periods: (1) preoperative—the time prior to admission to the presurgical care unit until transfer to the operating room (OR); (2) intraoperative—the time in the OR until transfer to the recovery unit; and (3) postoperative—the time spent in the recovery unit until transfer to the inpatient ward. 6 According to Forsberg et al., 7 the role of perioperative nurses is to provide a setting where patients receive the best support possible during the perioperative procedure. The primary purpose of these nurses is to ensure patient safety: to identify, prevent, and immediately treat early complications, especially surgical-related complications, before these develop into more serious or even life-threatening problems. 8 During the perioperative period, patients are highly vulnerable and largely dependent on the surgical staff. The perioperative nurses are responsible for creating and maintaining a sterile and safe surgical environment, providing preoperative and postoperative patient education, monitoring the patient’s physical and emotional well-being, and integrating and coordinating patient care throughout the surgical care continuum. 9 Given the importance of perioperative nursing care for the patient, it is clear that patients should be given the opportunity to evaluate the care received. 10 Although there are many different ways of defining patient satisfaction, no commonly accepted definition has yet been established. Nevertheless, patient satisfaction is closely related to the effectiveness of perioperative nursing practice and is thus one of the most important outcomes. According to Crow and colleagues, patient satisfaction in perioperative settings is correlated with the quality of information and communication. Satisfaction with the quality and quantity of information considerably impacts patient satisfaction levels. 11
Patient satisfaction studies conducted in recent years have used a range of different data collection procedures; moreover, a wide range of tools have been used to measure patient satisfaction to suit the aim of the particular study. There is, however, no universally available tool to assess satisfaction with nursing care.12–14 Previous studies have explored the association between patient satisfaction and individual variables, environment factors, climate, and teamwork.15–17 Recently, Palese et al. 18 explored the relationship between dissatisfaction and the quality of care offered in medical units. However, most of the aforementioned studies include only a few items directly related to nursing care, and there is a paucity of studies examining perioperative nursing care exclusively. Most questionnaires and scales measure patients’ perceptions of the general perioperative care received.5,19,20 Although this information is undoubtedly useful, it does not take into account of the type of nursing care patients would like to receive during the perioperative procedures.
Assessment of patient satisfaction is required at all healthcare institutions, and it is important to have consistent, interpretable data to perform an accurate evaluation. 21 Most of the tools currently used to assess patient satisfaction with nursing care were elaborated for the needs of a particular healthcare center, these tools have not been statistically verified, and their validity and reliability have not been established. To our knowledge, no scales specifically designed to evaluate perioperative nursing care have been developed yet. As a result, until such scales become available, the only alternative to assess patient satisfaction in the perioperative nurse care setting is to use one of the instruments designed for acute care. In this regard, after carefully reviewing the various scales, we believe that the La Monica–Oberst Patient Satisfaction Scale (LOPSS) is the most appropriate. This scale is a research tool that was elaborated based on significant aspects of nursing care and reflects the nursing behaviors patient expected in an acute care setting and show satisfactory levels of validity and reliability. The LOPSS has been adapted to meet Spanish requirements and has both content validity and reliability. 22 Therefore, in this study, we used the 12-item validated Spanish version of the LOPSS-12 to measure patient satisfaction. It is a short and simple to use, reliable and valid 12-item scale that can be used to assess patient satisfaction with perioperative nurse care. Cronbach’s alpha is 0.82.23,24 Moreover, this abbreviated version correlates closely (0.95) with the original version, the 41-item LOPSS. 24 The use of abbreviated scales, when appropriate, is that the response rates are usually higher than obtained when administering longer scales. 5
In this regard, we wanted to examine the following research question: What is the occurrence of satisfaction with nursing care as perceived by surgical patients at the moment of discharge from a perioperative unit? Therefore, the objective of this study was to assess the satisfaction of surgical patients with perioperative nursing care at our institution to improve the quality of care. The second aim was to determine whether a modified version of the LOPSS-12 (in which the response options were reduced from a 7-point to a 5-point scale) could maintain the sensitivity of the instrument and thus be used to reliably assess satisfaction in surgical patients.
Material and methods
Study design and participants
This was a cross-sectional study carried out in a convenience sample of 150 patients who underwent surgery at a tertiary care hospital. Inclusion criteria were age ⩾ 18 years and ⩾24 h of hospitalization. Exclusion criteria were impaired cognition impeding the ability to communicate or to complete a self-administered survey. The sample size was estimated P = 80%, for the expected proportion of patients based on previously published studies25,26 and with a confidence of 95%, and a margin of error of 6%. In total, 150 patients were required. An additional 3% was added to account for losses, which is how the final number of participants was set at n = 155. The following sociodemographic variables were assessed: age, sex, marital status, and educational level. Clinical variables included comorbidities, surgical specialty, length of stay, and destination at discharge.
Instruments
The LOPSS is one of the few validated scales available to measure overall satisfaction with nursing care. 22 For this study, we used the abbreviated 12-item Spanish version of the LOPSS (LOPSS-12) to assess patient satisfaction with perioperative nursing care. 24 The LOPSS-12 contains a mix of 12 negatively and positively worded questions designed to assess the user experience with the nursing team’s capacity to communicate effectively with patients and respond to their needs. Each question has seven response options expressed on a Likert-type scale ranging from 1 “strongly agree” to 7 “strongly disagree.” The score is based on the mean values for each item. In terms of the psychometric characteristics, the original version of the scale was based mainly on input from nursing professionals.
Prior to initiating this study, we first conducted a pilot test involving 10 surgical patients to assess the ability of recently operated patients to understand the scale. That pilot study showed that patients had difficulty understanding the intermediate responses on the original 7-point scale. Given that a previous study reported a similar sensitivity for the 7-point and 5-point revised LOPSS, 27 we reduced the 7-point Likert-type scale to only five response options to facilitate the accurate completion of the scale. This modification was made after a consultation between the research team and seven experts in the field. Thus, the version of the LOPSS-12 used in this study consists of 12-items with a 5-point Likert-type response format, as follows: strongly agree (1 point); agree (2); neither agree nor disagree (3); disagree (4); and strongly disagree (5). The responses to all items on the scale are averaged to obtain a mean score, with higher mean scores indicating greater satisfaction with nursing care.
Data collection
Data collection was carried out between December 2014 and February 2015 (Supplemental Material). The research team was not directly involved in the care of the patients included in the study in order to avoid introducing any potential informational bias. The investigator gave patients a verbal and written explanation of the study, after which all patients provided written informed consent.
The survey was given to the participants and completed at the time of discharge. The same investigator was responsible for data collection in all patients. To evaluate the results of the questions, the positively worded items (questions 1, 3, 7, 8, and 10) were recoded in the same direction as the negatively worded items (2, 4, 5, 6, 9, 11, and 12). Patient satisfaction was calculated as described in the study by Ríos-Risquez and García-Izquierdo. 28
Data analysis
The SPSS program, version 22.0 (SPSS Statistics for Windows, IBM Corporation, Armonk, NY, USA) was used for the statistical analysis.
Data were visually checked for normal distribution using Q–Q plots (quantile–quantile plot) and tested using the Kolmogorov–Smirnov statistic (p = 0.056). The normal distribution assumption was supported and so parametric tests were used in the analysis. A descriptive analysis of the categorical variables was performed, with these variables given as absolute and relative frequencies. The continuous variables are expressed as mean + standard deviation (SD). The variable “overall satisfaction” was created for the modified LOPSS-12. Finally, a bivariate analysis of the independent variables was performed, using the Pearson correlation coefficient for quantitative variables, and the chi-square test, Student’s t-test, or analysis of variance (ANOVA) for categorical variables. Internal consistency of the scale was tested by Cronbach’s alpha. The content validity was determined using Lawshe’s index with a group of seven perioperative nursing experts. They were requested to specify whether an item is necessary to the performance of the construct. To this end, they are requested to score each item from 1 to 3 with a three-degree range of “not necessary, useful but not essential, essential,” respectively. Content validity ratio (CVR) varies between 1 and −1. The higher score indicates further agreement of members of panel on the necessity of an item in an instrument. The CVR value is computed for each item. The mean CVR across items was used as an indicator of overall test content validity (Content Validity Index (CVI)). 29 Statistical significance was set at p < 0.05.
Ethical considerations
Ethical approval for this study was obtained from the hospital Research Ethics Committee (approval ID #42/2014). The safety and confidentiality of the study data are guaranteed according to Spanish law (15/1999) on personal data protection. All patients signed an informed consent form. The study adhered to the ethics guidelines of the Declaration of Helsinki, and patient confidentiality was fully protected in accordance with national legislation.
Results
Sociodemographic and clinical characteristics of patients
A total of 150 surgical patients completed the scale, for a response rate of 96.8% (150/155). Of the five who did not respond, one could not be contacted and the others refused to participate. The mean age was 63 years (SD, 16 years) (95% confidence interval (CI): 61.04–66.22). Of the 150 patients, 73 (49%) were women and 77 (51%) were men. In total, 69 patients (46%) had at least one comorbidity and 57 patients (38%) presented at least one hospital-acquired complication. Four different types of complications were identified, distributed as follows: pain (n = 35, 23.3%); bleeding (n = 12, 8%); wound infection (n = 10, 6.4%), and others (n = 11, 7%). Most patients (144/150; 96.7%) were discharged to home. The mean hospital stay was 26 h (SD, 3.7 h). The sociodemographic and hospital characteristics of the patients are shown in Table 1.
Sociodemographic and clinical characteristics of the sample (n = 150).

Values noted with an asterisk are given as standard deviations.
The results follow a normal distribution, with good symmetry, but with a high kurtosis in the central values. The mean overall satisfaction score with nursing care for the entire sample was 3.17 (SD, 0.21), with scores ranging from 2.58 to 5 points (median, 3.17). Table 2 shows the complete results for all LOPSS-12 items. To facilitate interpretation of the table, the most frequent responses for each item have been bolded. Satisfaction was generally high for all 12 items, but particularly for items 2, 5, 11, and 12—all of which received mean scores > 4 points (except for question 5, which was slightly under 4). The lowest rated items were questions 7 and 8, with mean scores only slightly above 3 points (see Table 2).
Satisfaction with nursing care. Results of the LOPSS-12* (n = 150).

SD: standard deviation.
Scores range from 1 to 5, as follows: 1—strongly agree; 2—agree; 3—neither agree nor disagree; 4—disagree, and 5—strongly disagree.
Responses are given as percentages.
Overall satisfaction is the mean of all items.
Satisfaction with nursing care
As Table 2 shows, the mean overall satisfaction score on the LOPSS-12 was 3.17 (SD, 0.21). The highest rated aspects of care (mean scores > 4) were for questions 2 (listens to concerns), 11 (works conscientiously), and 12 (answers calls quickly). Question 5 (patience) was also highly rated, with a mean score close to 4. By contrast, the worst-rated questions were items 7 (provides useful advice) and 8 (makes me feel I can share my problems). In the recoded positive questions, the most prevalent answer was “neither agree nor disagree.” In the negative questions, the most common response—with at least 60% of respondents (and as high as 75.8% of respondents)—was “disagree” (4 points). Overall, this indicated good patient satisfaction.
The only sociodemographic variables that were significantly associated with overall satisfaction with nursing care (the sum of all 12 items) were patient sex (p = 0.008) and comorbidity (p = 0.007); more specifically, men and patients with comorbidities were more satisfied overall with nursing care. None of the other sociodemographic variables were significantly associated with satisfaction.
The analysis of the 12 individual items from the LOPSS-12 revealed several significant differences (Table 3). Patients with university studies were more likely than patients without university studies to consider the nurse’s advice useful (item 7), but these same patients also considered the nurses to be impatient. Patients with hospital-acquired complications were also significantly more likely to perceive that “the nurse is more interested in finishing tasks than listening” (item 2), although they also felt that nurses work conscientiously (item 11) (see Table 3).
Significant associations between LOPSS-12 items and patient characteristics (n = 150).
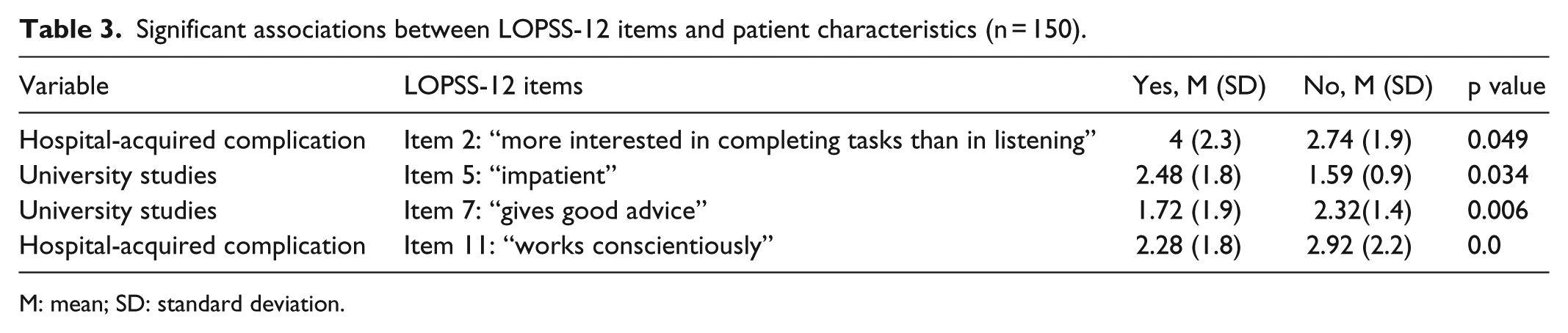
M: mean; SD: standard deviation.
Validity and reliability of the Spanish version of the modified LOPSS-12
Content validity was determined by an expert panel that reviewed the 12 items of LOPSS-12. The expert group consisted of seven nursing professionals specializing in perioperative nursing. They were asked to review and rate the relevance of each item. The CVR for each item was calculated, ranged from 0.71 to 0.86. The average CVR was 0.76. The statement was accepted if the CVR was ⩾0.56. 29 The experts agreed that all the items were relevant. No item was omitted. Cronbach’s alpha of the scale was 0.70; alpha coefficients for the items range from 0.695 to 0.718. Cronbach’s alpha was within the recommended range (α > 0.70). In general, values >0.70 are considered acceptable. The scale is brief and it takes about 10 min to complete.
Discussion
In this study, our aim was to assess patient satisfaction with nursing care in the surgical department and recovery rooms. The main finding is that patients were largely satisfied with the nursing care received, as evidenced by the mean overall satisfaction score of 3.17 on the LOPSS-12. These results are consistent with the results obtained in other studies.7,30,31 Although overall patient satisfaction was quite good, the findings from the scale identified two problems—both closely related—in need of improvement: (1) communication—to keep patients better informed about the perioperative care process—and (2) time dedicated to patient care. These findings regarding the need for better communication and the need to spend more time on patient care through the perioperative period are consistent with the outcomes of previous studies of satisfaction with surgical care.11,32 This is important, given that several studies have shown that patients have a better surgical experience when they perceive that they are well-informed and understand the process.32,33
This study reports a need to improve both the amount and the quality of information provided to patients. This is consistent with the results reported by Forsberg et al., who also evaluate perioperative procedures (rather than just surgical care in general, as in most other studies). However, those authors used a single instrument to assess the quality of perioperative care, evaluating the entire surgical hospital staff, not just the nursing team. 20
We found that patient satisfaction was associated with several different aspects, an awareness of which would allow hospitals to improve of quality services to better meet the needs of patients. For example, in line with previous studies, we found that men were more satisfied with nursing care than women.12,34,35 A study conducted by Findik et al. 15 found that women reported more problems with hospital care than men, because the female patients attach more importance to their health than male patients and tend to be evaluators and even administrators of care practices not only for themselves but also for other members of their family.
Another aspect is that patients with comorbidities were less satisfied with care than those without comorbidities because they may have a greater need for information, as other studies have reported.18,36 Despite our findings, other studies have not found any association between the presence of comorbidities and satisfaction.31,37 This discrepancy suggests that more research is needed to determine the true relation between these two variables, and to better understand how they may be related.
Alhusban and Abualrub 13 evaluated patient experience with nursing care and behaviors, with generally positive findings. However, in contrast to our research, the lowest rated aspect of nursing care in that study was patience. Our findings showed patients are satisfied with nursing care when the care is perceived as individualized and when nurses are perceived as caring, responsive, and empathetic. This difference could be due to the special emphasis at our institution on ensuring excellence in care through humanistic, personalized care. Some aspects of care and of nurse–patient interactions have been documented as attributes of patient satisfaction with nursing care.18,34
In our sample, 38% of the patients had complications, primarily related to postoperative pain, which is common in surgical care units. Postoperative pain did not significantly affect patient satisfaction, perhaps because these patients may have perceived the increased nursing care (to treat the pain) as more individualized. Also, surgical patients are likely to expect substantial pain and some complications after surgery, and thus, these factors may not negatively affect satisfaction with nursing care. Interestingly, the surgical patients who experienced hospital-acquired complications considered the nurses to be more interested in completing tasks than in listening (item 2). Surprisingly, those same patients also felt that the nursing professionals were conscientious in their work. 38 In contrast to our findings, some authors have reported that patients with postoperative complications show no decrease in overall satisfaction.39,40 Interestingly, patients with university studies were more likely than other, less well-educated groups to consider the nurses’ advice to be useful, although these same patients also perceived the nurses to be impatient. Patients’ educational level also influenced their level of satisfaction, perhaps because such patients want more information.18,19,34
Overall, the patients felt that nursing professionals need more time to satisfy patient needs. This finding was not entirely unexpected, given that high caseloads of acute care patients in the perioperative unit, and the corresponding complexity of the work required to care for them can increase the demands placed on nurses. Indeed, such patients require continuous, prolonged nurse–patient interaction, and ideally, the nurse should dedicate substantial time to explore patient perspectives and personal needs. However, in real-world situations, nurses are often pressed for time. Another factor to consider is that, in the perioperative setting, patients only spend a relatively brief period of time in the hospital—and thus their contact with the nursing staff is also relatively short, especially compared to inpatient wards, where patient stays are longer and thus there is a greater opportunity for patients and nurses to establish a closer relationship; as a result, this factor could have negatively influenced the patients’ evaluation of nursing care. 41
The results of this study could have important implications for the practice of perioperative nursing. Based on the overall satisfaction scores, we can conclude that the perioperative nursing care met patient expectations. We believe that the good results obtained in this study could be attributed to the systematic perioperative nursing care process in place at our hospital. In this sense, our system could be considered an example of a well-designed perioperative care process for other university hospitals. It seems clear that a systematic approach improves care delivery, thus allowing nurses to deliver care in a deliberate and competent manner, as other studies have reported. 42
A recent study conducted by Kennedy et al., evaluated the relationship between patient satisfaction and surgical outcomes, finding that satisfaction was not consistently associated with favorable outcomes in that setting, even though patient satisfaction is a clear measure of quality. In fact, as our results show, patients may be satisfied with the care received even if they experience hospital-acquired complications after discharge. Of course, a wide range of factors apart from nursing care—including staffing levels, the use of health information technology, hospital surgical volumes, and teaching status—can influence patient satisfaction. 43 As described by Pajnkihar et al., 44 nurses should be caring and establish personal contact, have a communicational approach, and have good relationships with patients. Based on our experience, we believe that it is essential to systematize perioperative care procedures while, at the same time, paying attention to the individual needs of patients. 45
Our findings indicate that nurses need to dedicate more time to patients—not only in providing nursing care but also in keeping them informed, providing written recommendations upon discharge, answering questions, and allowing patients to participate in the care process. 46 To our knowledge, our study is one of the few studies carried out to date to evaluate satisfaction with perioperative nursing care during the perioperative procedure. 47 However, additional studies are needed to expand our understanding of the factors that influence patient satisfaction in this setting in order to identify the specific aspects of perioperative nursing care amenable to improvement. Perhaps, the approach used in this study could be used to guide future studies on perioperative nursing care.
We found that the modified LOPSS-12 was suitable for assessing patient satisfaction with perioperative nursing care. The reported Cronbach’s alphas are well above the international recommended minimum levels and comparable to the previous validation studies.22,24,27 Moreover, the scale demonstrated adequate validity and moderate reliability, and therefore, this scale can be recommended for future research studies of patient satisfaction with perioperative nurse care. In our context, this instrument provides front-line researchers and managers with a reliable method of measuring and documenting patient satisfaction and identifying potential sources of dissatisfaction. Further research will expand the analysis and determine the instrument’s utility over time. The feasibility of using this instrument in other perioperative units should be assessed.
Study limitations
This study has some limitations that should be taken into consideration when interpreting the results. First, we used a convenience sample of 150 surgical patients, which is a relatively small sample size that affects the reliability of the results because it leads to higher variability. Ideally, a larger sample size would have provided more reliable results. In addition, we used a simplified version of the LOPSS due to the reduced ability of recently operated patients to understand a more complex instrument, and this could have influenced the results. Another issue is that we were not able to compare our results to recent data about patient satisfaction with perioperative nurses because no recent data are available. Despite these limitations, we believe that the study provides valuable data on nursing care in the perioperative setting that are not currently available elsewhere. Moreover, this study could be used as the basis to develop future studies. It would be more meaningful to repeat the study with larger samples to confirm the findings reported here.
Conclusion
Our findings show that overall patient satisfaction with perioperative nursing care was good. The patients in this sample rated all aspects of nursing care as satisfactory or better. Men were more satisfied than women with the care received, as were patients with comorbidities compared to those without any comorbidities. In addition, the educational level of the patient and the presence of hospital-acquired complications significantly influenced some aspects of patient perception of nursing care.
The results of this survey underscore several aspects of perioperative nursing care that may need improvement, at least in our particular setting. There is a clear need for nurses to provide patients with better advice, to keep them better informed, to exhibit greater patience, and to spend more time with them. The Spanish version of the modified LOPSS-12 was a reliable instrument to measure surgical satisfaction with perioperative nursing care, providing valuable information about the aspects of care in need of improvement.
Supplemental Material
Raw_Data__(2) – Supplemental material for Satisfaction of surgical patients with perioperative nursing care in a Spanish tertiary care hospital
Supplemental material, Raw_Data__(2) for Satisfaction of surgical patients with perioperative nursing care in a Spanish tertiary care hospital by Amalia Sillero Sillero and Adelaida Zabalegui in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express gratitude to all the surgical patients who kindly agreed to participate in this study, the nursing management team at the Fundació de Gestió Sanitària de l’Hospital de la Santa Creu i Sant Pau, Barcelona, España, and to Jose Manuel Garcia for providing statistical assistance. Finally, the authors thank Bradley Londres for editing the manuscript. This paper is extracted for the preparation in the Doctoral Dissertation: “Application of magnet values to the surgical area of a high-tech hospital.” All authors have contributed substantially to (1) conception and design of, or acquisition of data or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from ethics committee of the Hospital de la Santa Creu i Sant Pau (approval ID #42/2014).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.