
Abstract
People with impaired hearing or deafness often perceive communication barriers when and participating in their daily lives, such as when contacting primary healthcare, leading to a risk of them using emergency services for less urgent conditions. Therefore, the aim of the present study was to describe the perceptions of individuals with hearing impairments and deafness in relation to the treatment and communication they received from primary healthcare professionals. The study employed a mixed-methods design, and the data comprised questionnaire responses from 101 individuals with hearing impairments or deafness, including 11 open-ended questions, analyzed with conventional content analysis. The study was evaluated using the COREQ checklist and the GRAMMS guidelines to further improve the transparency of the research. The results indicate that healthcare professionals who are responsive, considerate, and respectful regarding communication were perceived among people with hearing impairments or deafness to be professionals. The ideal healthcare encounter for people with hearing impairments or deafness would be where the healthcare professionals could perform sign language, which would allow the healthcare professional to communicate freely. Healthcare professionals need more knowledge about how they can best meet, care for, and communicate with individuals with hearing impairments or deafness.
Keywords
Background
In Sweden, approximately 10% of the population lives with hearing impairments or deafness. 1 Many people with impaired hearing or deafness perceive barriers to communicating and participating in their daily lives, for example, when contacting healthcare services such as primary healthcare. People with impaired hearing or deafness are thus more likely to use emergency departments,2,3 but the implications of this have not yet been fully explored. 4 A previous study showed that by communicating with the help of hearing aids, hearing implants, sign language, signs as support, or an interpreter, there are now more opportunities for such individuals to participate independently. 5
The cause of hearing impairments or deafness can vary. Common root causes can include age, medical problems, and prolonged exposure to loud noises. 6 Hearing plays a central role in daily interaction with other people, and hearing impairments can lead to intense feelings of isolation, shame, and guilt, and can trigger crisis and grief reactions. 7 Previous studies describe that hearing-impaired and deaf people's perceptions of their contact with healthcare and medical care as being complex, for example, when names are called out in waiting rooms verbally, and where people are only able to independently contact healthcare services via telephone.7,8
Healthcare professionals (physicians, nurses, and other healthcare professionals) can create meaningful care relationships by facilitating good communication. 9 Hearing impairments and deafness can lead to difficulties in benefiting from the information provided by healthcare professionals. 7 According to Travelbee, 10 communication is one of the most essential tools that healthcare professionals can have because, in communication, thoughts and feelings are shared and conveyed, which makes it a mutual process. 10 Through good communication practices, healthcare professionals create good relationships with the person for whom they are caring. 8 Communication is a prerequisite to achieving nursing goals, as healthcare professionals can help the person manage their illness or suffering and find meaning in what is happening. Through communication, the healthcare professional and the person establish an interpersonal relationship, which means that the goal of nursing is achieved. The purpose of communication is to get to know the person and see their needs. Communication is constantly being enacted at the point at which two individuals meet, both verbally and non-verbally. 10
As hearing loss always affects communication between people, healthcare professionals who communicate with hearing-impaired or deaf people should keep their mouths free and visible, for example, not hidden by a moustache, mouth guard, or hands, as this can affect the ability to read lips. It is also essential that healthcare professionals make eye contact with the person before the conversation begins.11,12 Aids such as hearing amplifiers and hearing aids or interpreting services 10 can also be used to promote communication with the hearing impaired. 9 Healthcare professionals should, according to the Patient Act 2014:82, 13 to the greatest extent possible, make sure that the person has understood the information and has grasped what it means. Concerning each individual's circumstances, written information must be provided if the individual requests it. 13 According to previous studies, having increased knowledge of the perceptions of people with hearing impairments or deafness can increase their participation and autonomy and can alleviate any potential suffering caused by healthcare.7,12 Therefore, the aim of the present study was to describe the perceptions of individuals with hearing impairments and deafness in relation to the treatment and communication they received from primary healthcare professionals in Sweden.
Methods
The study employed a mixed-methods design. 14 Data were collected through the following: 1) a quantitative sample; and 2) a qualitative sample of free-text answers drawn from open-ended questions in a questionnaire designed by the authors to describe how people with hearing impairments and deaf people perceive healthcare treatment and communication. The questions can be seen as being general, overarching mixed-methods questions. 14 The study was evaluated using the COnsolidated criteria for REporting Qualitative research (COREQ) checklist 15 and the Good Reporting of A Mixed Methods Study (GRAMMS) guidelines 16 to further improve the transparency of the research.
Participants
The participants were recruited in the spring of 2022 from six Swedish groups on one social network site, designed for people with hearing impairments and including people with hearing impairments or deafness (with a range of 248–3900 members each). This sample was deemed to be adequate 17 in relation to the study's aim. The inclusion criteria were as follows: affected by hearing impairments or deafness; membership in one of the six social network site groups; aged 18 years or older; and the ability to read and understand Swedish. No delineation was made regarding gender and ethnicity. A total of 101 participants (19 men, 81 women, 2 non-binary; age range = 20–77 years; mean age = 50 years) answered the questionnaire. In total, 41 participants were deaf or had profound hearing loss, 40 had severe hearing loss, and 18 had moderate hearing loss and mild hearing loss. Answering the questionnaire was voluntary for the participants in the six Swedish groups on one social network site; therefore, non-response analyses were not performed.
Questionnaire
The authors developed a questionnaire that is addressed with both quantitative and qualitative approaches, 14 comprising responses to seven statements inspired by the National Patient Survey for physician visits in primary care centers in Sweden. 18 The questionnaire includes the following subjects: (1) Are you satisfied with how you can get in touch with healthcare (e.g. SHD1177 is a Swedish website for information and services in healthcare. SHD 1177 offers healthcare advice, information, inspiration, and e-services and is available around the clock at 1177.se and on the telephone for healthcare advice)? (2) During your last healthcare visit, did you receive enough information about your care/treatment? (3) Were you involved in the decisions regarding your care/treatment to the extent you wished? (4) Did you have the opportunity to ask the questions you wanted and did you get answers that you understood? (5) If you asked questions, were the responses given with compassion and commitment? (6) Did you feel included in the conversation if the healthcare professionals talked to each other about you? and (7) Did you feel treated with respect and dignity during the care meeting? The response options were based on a 5-point Likert scale, ranging from ‘no not at all’ to ‘yes, completely agree,’ and participants were given the possibility to comment with free-text answers under each statement. Background questions, such as gender, age, and degree of hearing impairment, were also included in the questionnaire. The COREQ 15 and the GRAMMS 16 guidelines were used by the authors to develop and improve the questionnaire. The questionnaire has not been validated and was developed exclusively for use in this study, which may be considered a limitation.
Data collection
The digital platform EvaSys (Evaluation System) was used to host a link to an electronic copy of the questionnaire online. The link was then shared on the six social network site groups that were included in the study. A total of 101 participants completed the questionnaire and responded to all of the quantitative (Likert-scale) and qualitative (free-text) questions (which resulted in a total of approximately 20 pages of free-text responses to the seven questions). Answering the questionnaire was regarded, in this study, as providing consent to participate.
Data analysis
The data from EvaSys were entered and analyzed in IBM SPSS 19 version 27. Descriptive analyses for comparing differences in the perceptions of healthcare professionals’ treatment and communication with individuals with deaf/profound, severe, moderate, or mild hearing loss were conducted using analysis of variance (ANOVA). As only two individuals had mild hearing loss, the groups with moderate and mild hearing loss were merged. Sub-analyses were conducted comparing sex differences among participants with deaf/profound hearing loss using the T-test. The significance level was set at 0.05.
The qualitative responses to the questionnaire were analyzed using conventional content analysis 20 to describe a phenomenon, for example, in this case, how people with hearing impairments and deafness perceive healthcare treatment and communication. The data analysis took place in four steps. In step 1, the data were read word by word repeatedly to achieve immersion and obtain a sense of the whole. In step 2, the data were read, and the researcher made notes of the text's impressions (initial analysis). As this process continued, labels and codes were generated and then became the coding scheme. In step 3, these codes were sorted into categories, and meaningful clusters were identified. Step 4 identified categories and codes from the data, and a new version of the text was written to describe these categories. 20 The analysis generated three categories. To secure trustworthiness, the text was analyzed separately by all authors, who then compared, and discussed the results together to reach a consensus in the interpretation of the data. The study was also evaluated using the COREQ checklist. All of the authors were involved in each of the steps, and all authors discussed and reflected upon the text to secure trustworthiness. 19
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki's principles, 21 taking into account the four ethical principles: respect for autonomy; beneficence; non-maleficence; and justice. The study was designed, planned, and performed as per Swedish law, which states that ethical approval is not needed when individuals are invited to participate voluntarily in questionnaires. In this case, regarding the perceptions of individuals with hearing impairments and deafness relating to healthcare professionals’ treatment and communication, the participants were not considered vulnerable, and their health was not negatively impacted by participating in the study. Written information about the study aim was provided in EvaSys, and this emphasized the study's adherence to confidentiality and the voluntary nature of participation. Participants were also clearly informed that answering the questionnaire constituted the providing of informed consent to participate. To promote anonymity, the data were analyzed after being anonymized. Confidentiality was achieved by storing the anonymized data files, with printed copies of the questionnaires, in a locked fireproof cabinet, and data analysis only occurred at the group level.
Results
The results are presented in two parts as follows: (1) quantitative responses; and (2) qualitative responses from the questionnaire to describe the perceptions of individuals with hearing impairments and deafness in relation to the treatment and communication they received from primary healthcare professionals.
Quantitative responses
Among the 101 completed questionnaires, 41 (41%) were answered by individuals with deafness/profound hearing loss, 40 (40%) with severe hearing loss, 18 (18%) with moderate hearing loss, and 2 (2%) with mild hearing loss. The mean age among the participants was 49.0 ± 12.1 years; 19 (19%) were men, 80 (79.2%) were women, and two (1.8%) were non-binary (Table 1).
Characteristics of the study participants.
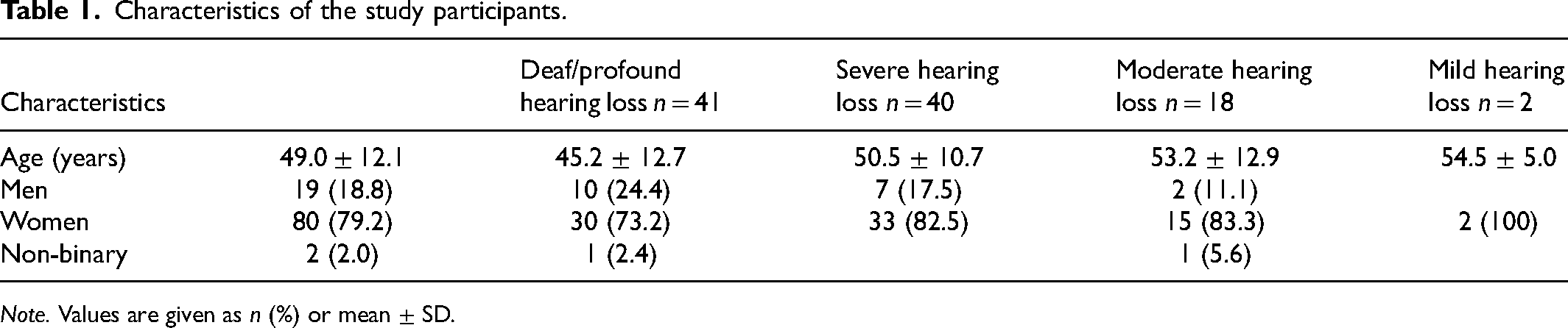
Note. Values are given as n (%) or mean ± SD.
Statistically significant differences were found between the groups on their perceptions of satisfaction with how to get in touch with healthcare (p = 0.001). Individuals with deafness/profound hearing loss were less satisfied compared to those with severe and moderate/mild hearing loss, respectively. Furthermore, individuals with deafness/profound hearing loss agreed to a lesser extent compared to the other groups on whether they received enough information about their care/treatment during their last visit to healthcare services (p = 0.040) (Table 2).
Results from the questionnaire divided into levels of hearing impairments.
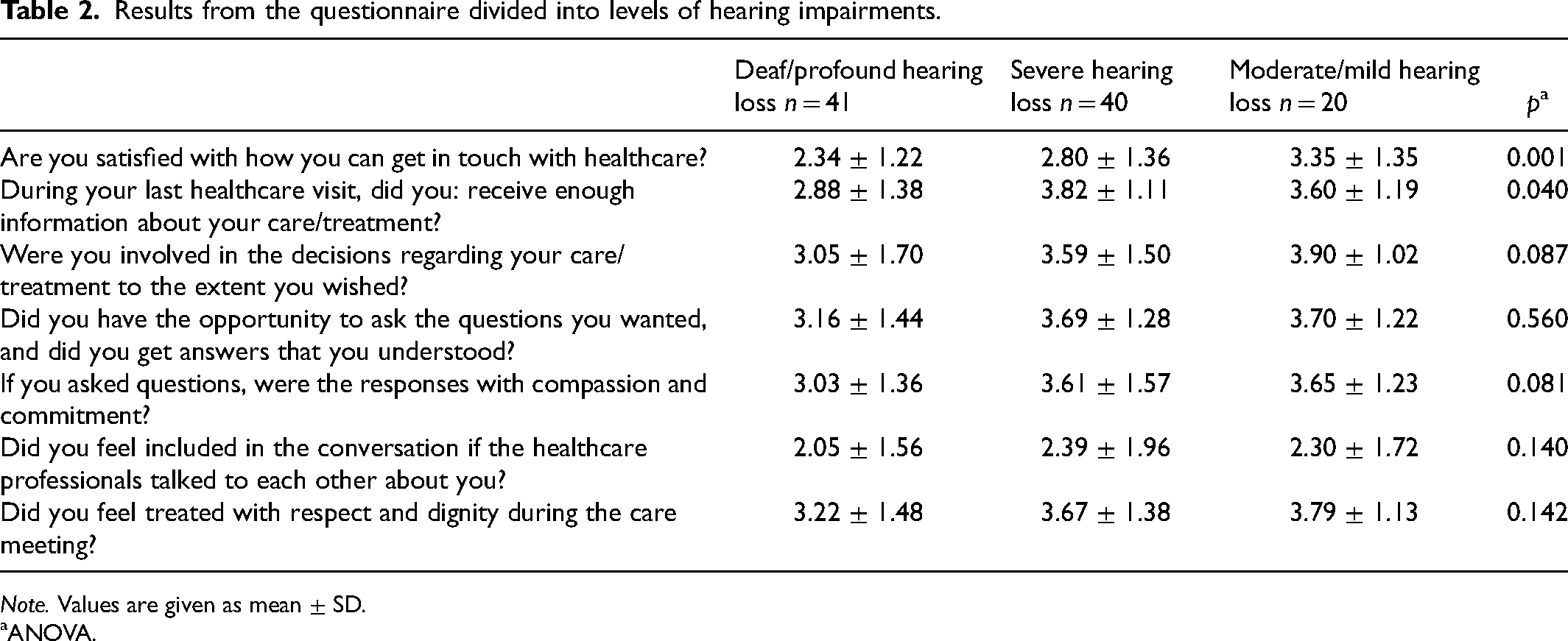
Note. Values are given as mean ± SD.
ANOVA.
Sub-analyses on gender differences among individuals with deafness/profound hearing loss showed that women were more likely to agree that they were treated with respect and dignity during the care meeting compared to men. Men, on the other hand, agreed to a higher extent that they felt included in the conversation if the healthcare professionals talked to each other about them, compared to women, although not significantly (Table 3).
Differences between sex among persons with deaf or profound hearing loss.
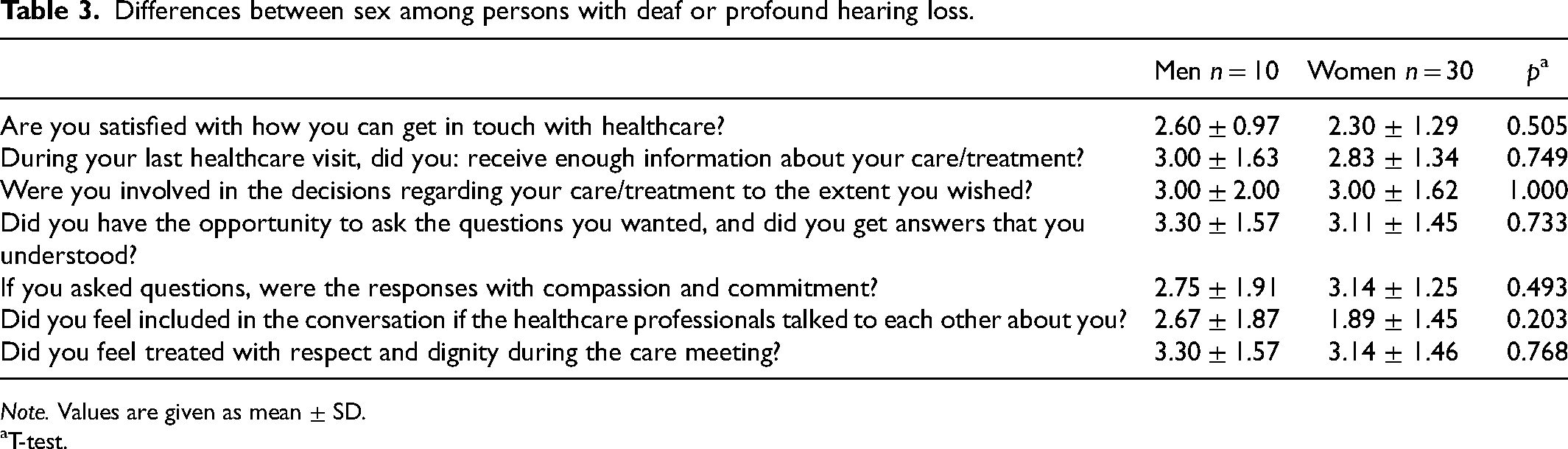
Note. Values are given as mean ± SD.
T-test.
Qualitative responses
The qualitative responses are presented in three categories: Getting in touch with the healthcare system; Communication with healthcare professionals; and Healthcare professionals’ knowledge and behavior in the encounters.
Getting in touch with the healthcare system
The participants perceived that the primary care centers’ call-back system creates problems for people with hearing impairments as they cannot instruct how they would like to be called back. Relatives or friends are needed to support the contact, as one person described:
I call and want to talk to the nurse – and they give me an appointment and call me back… But they can’t because I use a video phone. It is impossible to tell when I call them, and I am forced to try to reach them via Swedish healthcare direct (SHD1177) text message function… and I only get an answer a few days later. I rely on hearing acquaintances to be able to stand by and call in an emergency. Even for my children… There are 3–4 people involved in a call, unnecessary!
The lack of knowledge among healthcare professionals about, for example, intermediary services such as text and video telephony, also entails hearing-impaired individuals having to make multiple calls when they connect to primary care centers. The messaging function in SHD1177 was described as being limited because each message starts a new case, and the response time is often long. Therefore, opportunities for the person to chat online with the primary care centers instead of calling them by phone were deemed preferrable.
Communication with healthcare professionals
The participants wished for the healthcare professionals to individualize how they communicate with hearing-impaired individuals to increase feelings of inclusion. The sense of involvement was also affected when communication was performed via a third party as an interpreter, as it is challenging to follow conversations when more than two people are involved. Communication with an interpreter was perceived as potentially excluding the hearing-impaired person. However, interpreters were also perceived to facilitate communication, as did pen-and-paper communication. Interpreters who were also relatives could lead to a lack of privacy. Physical interpreting is perceived to be better than digital interpreting, as there is less risk of misinterpretation, as one person described: It is not safe with remote interpretations in healthcare – there must be a physical interpreter on site because it is about patient safety and communication.
Digital interpreting was also perceived as being unsafe as technology cannot be trusted to be accurate. In addition, a sense of uncertainty was perceived in that the interpreter may not accurately interpret everything that the healthcare worker communicated.
Oral communication without an interpreter was perceived as presenting a risk of misunderstanding and omission of information. Processing verbal communication was also perceived to take longer; for example, follow-up questions may arise afterwards. When healthcare professionals need to wear protective masks, communication was also perceived as being more complex, as masks cover the mouth and make it impossible to read lips and hear when a name is called in the waiting room.
During conversations, being attentive to body language and ensuring that the healthcare professional faces the person during the conversation was perceived as being essential for optimal communication. Healthcare professionals who choose to wear a protective visor instead of a protective mask were seen to help facilitate communication. Supplementing verbal and written information was regarded as being positive, but not all healthcare professionals offer this. One person described how:
Some doctors didn’t want to take written communication with me on the spot when no physical interpreter showed up – and told me to get a new appointment. That's not right!
Feelings of not being included and that healthcare professionals are talking over the person's head were perceived to emerge if they also face away from the person. Increased engagement with the person with hearing impairments can be promoted by making eye contact during the conversation.
Healthcare professionals’ knowledge and behavior in the encounters
The participants perceived that healthcare professionals do not always see the person behind the hearing impairment, but instead see a persona with illness for whom they feel pity. One person expressed it in this way:
Often people have difficulty seeing behind the disability/impairment and tend to see only the deafness when looking for a broken finger. They are either afraid and stay far away or behave completely differently towards me than others, e.g. ‘You are so good and so happy.’
Healthcare professionals’ lack of understanding when meeting people with hearing impairments was perceived as them being indifferent and absent. Ensuring that interpreters or hearing aids are available, having a positive attitude, and behaving professionally were all perceived as being necessary. A lack of interpreters or hearing aids was perceived as leading to information being missed. Healthcare professionals need knowledge about how the person with hearing impairments communicates, and this information is required for the medical record to prevent misunderstandings, such as not arranging to book interpreters.
Discussion
These findings indicate that the groups of participants perceived some difficulties when contacting primary healthcare, particularly as the system is based on calling via telephone, making them dependent on using their relatives when making contact. A similar result was found in a previous study 10 describing that deaf individuals prefer to use an interpreter to contact healthcare, especially when there is a lot of information to receive. The present study also indicates that deaf people are generally more dissatisfied with contact with primary healthcare care than the rest of the group. Textphones 22 were also seen as a possibility for people with hearing loss or who are deaf to communicate with healthcare services; however, healthcare professionals lack knowledge about using textphones and this can be a barrier. Many participants also perceived that the messaging function in SHD1177 could be restructured to improve possibilities for people who are deaf or hearing-impaired to contact healthcare. Negative attitudes among healthcare professionals regarding the booking of an interpreter and a negative attitude towards deaf individuals have also been described in a previous study. 8
In this study, healthcare professionals were described as being indifferent and absent, as they were not interested in adopting communication with an interpreter. On the other hand, healthcare professionals who were accommodating and adapted their communication with an interpreter were seen as being professional. A greater proportion of women than men felt that they received a good response and empathy when asking questions in the healthcare services meetings. However, unlike the women, the men agreed to a higher extent than women that they were treated with respect and dignity during the care meeting. In line with this result, Teunissenet al. 23 found that, when experiencing care during a hospital stay, women assessed the quality of hospital care significantly lower than men did.
The results indicate that wearing face masks can make communication more difficult as they affect the ability to read lips as they cover the mouth, which aligns with previous research by Stevens et al. 7 and Shepperd et al. 24 Healthcare professionals who use visors instead of face masks can be perceived as being more accommodating and considerate to the person. These healthcare professionals took the person's condition into account and were therefore seen to provide good treatment as a prerequisite for good care. In conversations involving several individuals, it is difficult for people with hearing loss or who are deaf to be included. The feeling that healthcare professionals are talking over their heads is described in the result, as were difficulties in following conversations when healthcare professionals face away from them. Barnett 11 also highlights the importance of making eye contact and paying attention to the person in question before the healthcare professionals start talking. Communication should occur face to face and with proper lighting in the room and should also give the person a feeling of being included in the conversation about what is happening. The participants also perceived difficulty hearing when they were called in the waiting room, as described in a previous study. 25 Solutions such as those proposed by Scheier, 12 using pagers or vibrating devices, were considered to be reasonable solutions and were described as decreasing the risk of missing appointments.
The results indicate that the interpreter can be a facilitator in establishing involvement in relationships with the healthcare professionals. Travelbee 10 describes how communication can be used by healthcare professionals to convey a shared and engaged feeling, making it a mutual process in the healthcare encounter. 10 Conversely, Ayala-Hernandez et al. 8 suggest that it becomes more difficult for individuals with hearing impairments or deafness to find trust and establish contact with the healthcare professionals if the interpreters are not neutral or if they are too involved in the healthcare encounters. Some participants described that healthcare professionals could have difficulties seeing the person behind the hearing impairments or deafness. The participants described how healthcare professionals see hearing impairments or deafness as a disease and that the person was a ‘poor disabled thing’ or felt that they were an inconvenience. Travelbee 10 explains this by describing that a reduced sense of self-worth can cause suffering, various types of losses, or separations. Often, suffering is related to the illness that results in loss of spiritual, emotional, and bodily integrity. 10
The results also indicate that healthcare professionals can find it challenging to meet individuals with hearing impairments or deafness and only allow relatives and close relatives to attend, not interpreters. According to the Patient Act 2014:82, 13 healthcare professionals should, in the meeting, consider the individual circumstances of the person with hearing impairments or deafness, understand the information and what it means, and written information must be provided if the individual requests it. 13 However, healthcare professionals can perceive stress in encounters with persons with hearing impairments or deafness, as the meeting can take up more time than regular healthcare meetings. 8
Strengths and limitations
This study's main strength is that it explores a rarely studied area: how people with hearing impairments and deaf people perceive healthcare treatment and communication. The analysis can broaden the knowledge of healthcare professionals in how to meet individuals with hearing impairments and deafness. Recruitment took place through contact with six groups of individuals who engage on a Swedish social network site, a network designed for people with hearing impairments and that included people with hearing impairments or deafness, to obtain a purposive sample to obtain dependability, credibility, and transferability. The questions included in the questionnaire were adapted for the purpose of the study and are based on a validated questionnaire. 19 As the questionnaire consisted of both quantitative and qualitative parts, there was an opportunity for the participants to explain their responses. One limitation of the study is that the participants could choose to provide a neutral response to the questions; providing a scale of 1–6 would have meant that the informants would have had to take a definitive position. Authenticity was secured by including original quotations from the qualitative responses in the questionnaire in presenting the results. Credibility and reliability were also secured by including all of the authors in the coding, analysis, and interpretation of the data. One strength is that the participants were of both genders and that their ages were in the range of 20–77 years. This was therefore seen as a suitable sample for the aim, which further secured credibility in the study. One limitation may be that all participants were from Sweden and the sample only included a total of 101 individuals. Including more participants could have presented the results in more depth, and differences in the results may have been more significant. The relatively small sample size could limit the generalizability of our results, and the questionnaire was explicitly developed for this study. The small group size also reduces the transferability of the results. However, the sampling sizes are appropriate when performing this type of study and therefore strengthen the reliability. Credibility and reliability were enhanced when all participants answered the same questions.
Conclusions
This study contributes to knowledge about what the ideal healthcare encounter for individuals with hearing impairments or deafness would be by illustrating that, if the healthcare professionals could perform sign language, this would allow the healthcare professional to communicate freely. The study indicates that healthcare professionals who are responsive, considerate, and respectful regarding communication are perceived among people with hearing impairments or deafness as being professional. The lack of knowledge among healthcare professionals in primary care about how to best meet, care for, and communicate with people with hearing impairments or deafness is also highlighted. The study findings might also provide healthcare professionals with knowledge and insight into how individuals with hearing impairments or deafness want to be treated in primary care.
However, future studies need to be performed to describe how people with hearing impairments and deaf people perceive healthcare treatment and communication in meetings with different groups of healthcare professionals, across different cultures, and in different languages, to further investigate the perceptions of those affected by hearing impairments deafness.
Footnotes
Acknowledgements
The authors would like to express their gratitude to all the participants who shared their perceptions of living with hearing impairments, and to Aileen Ireland for the language editing and proofreading of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.