
Abstract
In meetings with healthcare professionals, transgender people are often met with ignorance. The meetings tend to focus more on the person’s gender identity rather than reasons for the contact and therefore may be perceived as being offensive to that person. The aim of the study was to describe transgender people’s experiences in their meetings with healthcare professionals. Fourteen transgender persons were interviewed in this descriptive qualitative study. The semi-structured interviews were audiotaped. Data were collected during January–February 2015 and analysed using content analysis. Three themes were identified: ‘Experience of treatment by healthcare professionals’, ‘Expectations of meeting with healthcare professionals’ and ‘Consequences of meetings with healthcare professionals’. Findings revealed that healthcare professionals do not always respect the patient’s gender identity. This could lead to their avoiding contact with healthcare services. More education/training of healthcare personnel for the treatment of transgender people seeking care is requested.
Introduction
Transgender is an umbrella term used to describe people whose gender identity and/or expression differs from the gender assigned to them at birth.1–4 In Sweden, a person who wishes to change gender will be diagnosed as transsexual, which is regarded as a psychiatric diagnosis. 5 Löfgren-Mårtensson 6 considered this to be a pathologisation of transgender people, which, according to the American Psychiatric Association, may cause distress and problems in coping with everyday life. 7
An increased number of people choose to be open about their gender identity, resulting in transgender people becoming more visible in society.8–9 Proper estimates of the number of transgender people in Sweden are difficult to obtain since not all forms are registered. 10 Between 1992 and 2009, over 540 people in Sweden applied to correct their legal gender and the number of applications has been increasing every year. 5 Despite this development, transgender people continue to be a vulnerable group in society. 8 Several studies report experiences of exclusion, loneliness, and abandonment from early childhood among some transgender people. Some transgender people experience discrimination from their parents and some have been ejected from their homes as young adolescents.4–6,9,11–12 Several reports conclude that those who choose to be open about their gender identity often risk discrimination in parental relationships, family life, employment, the workplace environment, as well as violence and loss of relationships.5,9,11–12 As a consequence, the general health of transgender people is below the level of that of the general population.13–14 Similar observations have been reported, for example, in the USA, where transgender people suffer from mental disorders (e.g. depression and anxiety) more often than the general population. 15 Substance abuse problems are also common, which increases the risk for other diseases4,15 and may lead to frequent contact with healthcare services. 4
Healthcare professionals working with transgender people may find that social security numbers and names do not match the patient’s gender identity, which may cause confusion. 16 Confirmation of the patient’s gender identity is important, as the opposite may cause the person to avoid healthcare contact in the future. 17 According to Darj and Nathorst-Böös, 18 transgender people are often treated with ignorance in their contacts with the health services, especially when they seek care that is unrelated to gender correction. The contacts tend to focus primarily on the person’s gender identity, rather than the actual cause of the contact. It can be considered offensive when questions about gender, genitalia, and treatments are irrelevant to the visit and steal focus from the person’s current problem. 17
According to the Swedish legislation, discrimination based on gender identity or expression is illegal. 20 This law protects against harassment, indignity and disadvantageous treatment. The law also states that discrimination within the healthcare system is prohibited. 20 Despite this law, transgender people are a group of patients at risk of being subjected to discrimination. 19
Research questions
Although previous studies have reported that transgender people are a vulnerable group in society,9,11–12 the outcome of visits within the healthcare system has been scantily studied. Therefore, the aim of the study was to describe transgender people’s experiences in their meetings with healthcare professionals.
Method
Study design
A descriptive qualitative design was used.
Participants
The sample consisted of 14 transgender people, aged 20–50 years, living in the Stockholm area and with experience of the Swedish healthcare system which was not related to gender reassignment.
Context
In this study, transgender people are defined as people living with a different gender identity and gender expression from the biological and legal gender assigned to them at birth.
Data collection
Suitable participants were contacted through the Swedish Federation for Lesbian, Gay, Bisexual, Transgender and Queer Rights (RFSL). An invitation to participate in the study was published via the RFSL website and Facebook group, transgender organisation Full Personality Expression Sweden (FPES) and the organisation Gender-Sex Identity-Diversity (KIM). The participants were selected according to the chain sampling technique called snowball sampling. 21 Prospective participants communicated their interest to the authors and received specific information about the study by email, e.g. information that the interviews would be audiotaped. Participation was then confirmed by telephone and a time was set for the interview in a place that the participant found suitable.
An interview guide with open-ended questions for maintaining consistency was developed as a checklist for the topics and issues to be covered. 22 It was tested in two pilot interviews with participants meeting the requirements for inclusion in this study. The interview guide was found to be appropriate and therefore the pilot interviews were included. Every interview started with an invitation to the participant to speak freely about their experiences of meetings with caregivers in the healthcare system. The interviews were conducted in January and February 2015, in a place and time chosen by the participant. Each interview lasted approximately one hour.
Data analysis and rigour
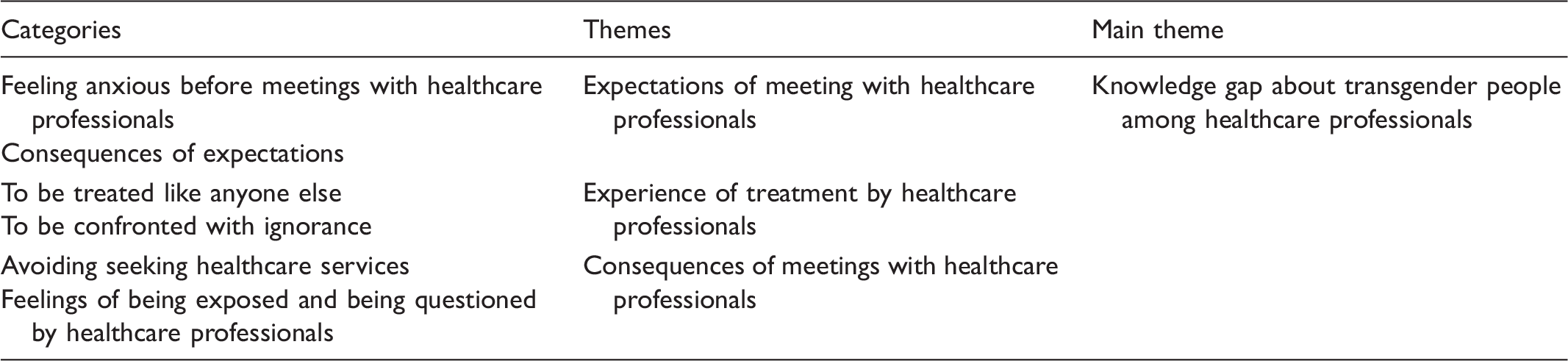
Content analysis of written reflections of transgender people on their experiences of treatment in connection with healthcare contacts.
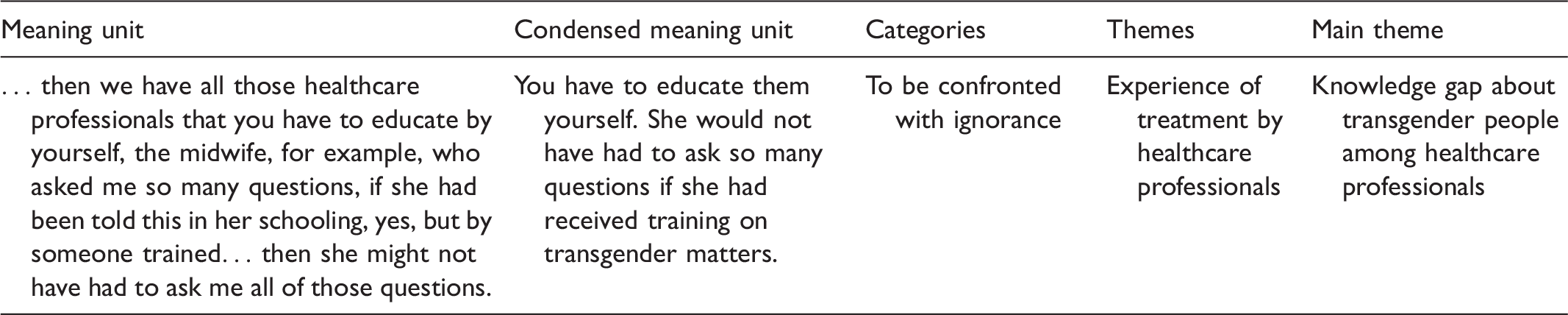
Example of the condensing and analysis process.
Ethical considerations
Ethical considerations were rigorously applied to every step of the procedure in accordance with the ‘Ethical principles for medical research involving human subjects’. 25 All the participants received a letter containing a full description of the aim of the study, the information that participation was voluntary, confirmation of their right to withdraw from the study at any time and assurance of confidentiality. Before the interview started, this information was repeated and the verbal consent of each participant was obtained. All names were removed from the data, which were then coded with a number to ensure anonymity and confidentiality. The Research Ethics Council at Sophiahemmet University approved the study.
Results
Knowledge gap about transgender people among healthcare professionals
The majority of the participants reported that they have had mostly positive experiences from their contacts with the healthcare system. They also indicated that they have rarely or never encountered direct discrimination by healthcare professionals. When the doctor took my personal information I told him that I am transgender because I thought it might be important. He looked at me and said, ‘Well, good for you’, and then he moved on.
Experience of treatment by healthcare professionals
This theme consists of two categories: To be treated like anyone else and To be confronted with ignorance. The participants stated that they often expected to encounter ignorance on the part of healthcare professionals, and also the risk of discrimination or malpractice. They said that they were surprised when they were treated like everyone else and when there was no unnecessary focus on their gender identity. Some participants reported that, in their experience, healthcare professionals rarely focused on gender identity, which they appreciated. Others experienced that healthcare professionals sometimes tended to concentrate on gender identity when they sought care for issues where gender was irrelevant instead of diagnosing and treating their actual health concern. People get hung up on it [gender identity] very easily. Now I’m here because I might have the flu. Can we focus on that? She asked me about my life in general and I told her that I was transitioning. She was very supportive and said many uplifting things, such as, ‘I think you are so strong to have come so far’. That made me feel very respected.
Most participants thought that the attitudes of the healthcare professionals they experienced were affected by ignorance and a lack of knowledge. They expressed some understanding for this situation. They stated that healthcare professionals should acknowledge their ignorance and dare to ask questions about things they do not know about transgender people that may be necessary for adequate examination, diagnosis and treatment. Some participants felt that physicians had sometimes been unsure if and how they could treat the patient because of the patient’s hormonal or surgical status. One informant stated that she got the feeling that they did not want to treat her because of fear of something going wrong. I have chosen not to do any genital surgery, for I believe that if there is a complication on a weekend, and I have to attend the emergency department, where they have no experience at all. When I show the staff my genitals they will be puzzled and say, ‘Oops, what is this? This I know nothing about’.
Expectations of meeting with healthcare professionals
This theme consists of two categories: Feeling anxious before meetings with healthcare professionals and Consequences of expectations. Some participants stated that they often felt worried before seeking healthcare. They have felt a particular aversion to such meetings. They found it difficult to explain their situation and they often worried about how the professional would respond. I am afraid that a difficult situation will be created. That it would not be just a regular thing, but something strange that I have to explain.
Another participant expressed anxiety about being treated poorly or denied help because of their gender identity. This resulted from hearing stories told by acquaintances who had been treated with ignorance by healthcare professionals. Some participants admitted that such stories had increased their concern and caused them to refrain from seeking care for this reason. There is a widespread perception that primary care does not have good skills for dealing with transgender people. I would rather wait a while and see if my health issues subside by themselves before I seek healthcare. I was in a position where I had to make up my mind, either I say something now and let this man know that what he was saying was not okay, or I try to enlighten and quickly trans-educate this poor man, and I chose the latter.
Some participants admitted that they had delayed or avoided seeking healthcare due to worries of being met with ignorance, even though they had health concerns. One informant explained that she refrained from seeking care because of fear of being treated badly, even though she believed that she suffered from cancer.
Consequences of meetings with healthcare professionals
This theme consists of two categories: Avoiding seeking healthcare services and Feelings of being exposed and being questioned by healthcare professionals. Although all participants had had several positive experiences with healthcare professionals, they had all at some point experienced negative encounters.
To have their gender identity questioned and their birth gender revealed in front of other people, e.g. in a waiting area, was something that the participants perceived as being upsetting. They were worried about having to explain their situation to a receptionist, e.g. when the social security number does not match their gender identity, or that a caregiver would call out their birth name in the waiting room. Revealing conversations initiated by healthcare professionals had occurred many times in waiting areas where there were other people. The participants considered situations in which outsiders could hear discussions about gender identity to be extra sensitive. Instead of just saying, ‘Yes, of course’, and ending the conversation there, she wanted to defend herself and said, so that everyone else could hear, ‘But I looked at your social security number…’ Thank you! Now you have also revealed that I have a male social security number!
Virtually all participants had experienced that their gender identity had been challenged in different ways in encounters with healthcare professionals. This had occurred directly in conversation and indirectly on the charts. Again, they stated that it was complicated when a social security number does not match their gender expression. Sometimes healthcare professionals questioned whether the social security number was correct, which led to further discussion. One informant pointed out that he is regularly questioned when he introduces himself.
Most participants had experienced that the healthcare professional’s own feelings affected how they were received as patients. It is not unusual for the healthcare professional to be uncomfortable and nervous in the meeting. The participants felt that these feelings have prevented healthcare personnel from daring to ask the necessary questions. I explained that I am not a biological male and she became incredibly embarrassed. She started on a long and incoherent discourse until she finally asked what I wanted.
Most participants compared the experiences they had had with general healthcare professionals with those they had had with the caregivers in the sex change investigation. All participants felt that general healthcare professionals had treated them better than the healthcare professionals in the investigation. One participant stated that he felt that the investigator was more closed-minded and prejudiced than his old family doctor was. The participant reported that healthcare professionals could use such expressions as ‘sweetie’ and ‘good girl’, expressions which were considered offensive. All participants stated that they believed that healthcare professionals working with investigations concerning sex reassignment have a stereotypical mindset and a conservative view of what is typically male or female. One informant stated how she could not be diagnosed with transsexualism because the investigator believed that she did not have a sufficiently feminine gender expression. As a trans person you are forced to be so very female. For example, a psychiatrist told me that I had to wear more make-up and more feminine clothes. But I don’t want to wear make-up and female clothes. There are different kinds of girls; some just want to wear jeans and sweaters, but it’s still a girl.
Discussion
The study revealed that attitudes towards transgender people among Swedish healthcare professionals vary between different types of care. For example, in gender reassignment clinics, the healthcare professionals were perceived as being predominantly negative, nonchalant and having a lack of compassion. In primary care, the experience was the opposite; the informants were often met with kindness, respect and dignity. The participants considered it important that healthcare professionals’ attitudes should always be characterised by openness. Polly and Nicole 19 highlighted the importance of patients always being treated with dignity, respect and compassion, and outlined that a basic principle to facilitate the first meeting is to ask the patient what pronoun and name is preferred, which is supported by other research.10,16–17 When the healthcare professional validates the patient in such a way, a trusting relationship can be created between them, which is consistent with other studies highlighting that a sign of respect is to use an person’s name and the correct pronouns10,16–17 and this is important for how the healthcare encounter will proceed. 26
The findings indicated that most of the healthcare professionals that the participants had encountered have not always possessed adequate knowledge about transgender people. Consistent with previous studies, 18 the informants in this study stated that they often encountered ignorance when they sought treatment. A lack of education about transgender people in healthcare is common according to Alegria and may explain why participants find healthcare professionals’ ignorance so vast. 9 They perceived this ignorance as being very troublesome. Fossum pointed out that if healthcare professionals do not reveal their lack of knowledge, it could result in the patient experiencing insecurity in the meeting. 26 The study indicated that some participants have concerns about future contacts with healthcare and therefore avoid seeking care when it is needed. This concern may stem from previous experiences of ignorant or unpleasant caregivers, but also from rumours of poor service. These results have also been reported by other researchers, who have shown that previous experience of poor treatment, as well as the rumours, may lead to transgender people being less likely to seek treatment.18–19
The lack of knowledge among healthcare professionals, combined with the absence of general guidelines and training in the treatment of transgender people 5 may be the basis for the negative experiences that the participants in this study described. One example is an irrelevant focus, i.e. when the caregiver is unnecessarily focused on the patient’s gender identity, a phenomenon that could arise from ignorance. Darj and Nathorst-Böös pointed out that that healthcare professionals usually tend to be more focused on a transgender person’s gender identity rather than the actual reason for the visit. 18 Sometimes healthcare professionals’ own curiosity may overtake their professionalism, which can lead to inappropriate questions and statements. It is therefore important that healthcare professionals should recognise their own ignorance and let the patient’s needs take control. Studies have shown that transgender people with experiences of inappropriate questions and statements are more likely to avoid healthcare than other groups of patients.4,18–19 Even rumours of a negative response from healthcare professionals have been shown to reduce confidence in the entire healthcare system. 19 Using simple and direct questions, healthcare professionals can reduce the risk of appearing to be curious and pushy. 17
When a transgender person seeks care, confusion about the patient’s gender identity may arise. In this study, it was the social security number that caused the most questioning of the gender identity of the participants. One reason for this is that the social security number is used almost universally for identification in Sweden. This has been described by Darj and Nathorst-Böös. 18 For example, a person may look like a woman and present herself with a female name, but have a male social security number. When the questioning of the patient’s gender identity occurs in places where other patients can hear, e.g. in a waiting room, the participants perceived it as being particularly disrespectful. Questioning of gender identity and revealing their birth gender may also be perceived as being offensive by the patient and is contrary to the National Board of Health and Welfare (NBHW) guidelines, which state that no one should feel offended in their contact with the health services. 5 Such issues are probably due to ignorance and unfamiliarity on the part of healthcare professionals and illustrate the need for education and action plans for the care of transgender people. The NBHW points out that a national care programme is needed and should be produced for the care of transgender people within the Swedish healthcare system. 5
The study indicated that the participants experienced treatment by gender reassignment investigators as being offensive and worse than that they experienced in general healthcare. They viewed the investigators as thinking stereotypically and normatively to the point that they felt compelled to exaggerate their gender expression to fit into stereotypical gender roles. The stereotypical and normative image of gender roles within the healthcare system was criticised in a report by the NBHW. 5 This is startling since the gender reassignment investigators are specialists for this group of patients. One explanation for this experience may be that the participants’ desire to live with their true gender identity probably makes the contact with the gender reassignment investigators more important than being treated for, e.g. an infection in the general healthcare system. Another explanation may be that gender reassignment investigators are bound to follow certain standards, e.g. which questions must be asked. Some of these questions could be perceived as offensive to patients who are already in a vulnerable situation. Gender confirmation treatment and/or corrected identification documents often affect a transgender person’s quality of life 27 and therefore a disrespectful response at such a time may be more important than a good response from general healthcare providers.
This qualitative study has several limitations. First, the informants volunteered to participate in the study and therefore we do not know the views of those who did not want to talk about the subject. Using a so-called snowball method 21 to recruit informants interested in participating in the study resulted in a variation of age and experience. During the interviews, the informants answered the questions quite exhaustively and there was a great interest on their part in sharing their experiences. We obtained varied and multifaceted data that gave us the opportunity to explore and analyse the informants’ experiences in meetings with healthcare personnel. Another limitation is that we did not collect demographic data from the informants. If we had done so, we might have highlighted other factors of importance such as social class or ethno-cultural background. However, the picture of transgender people’s experiences of Swedish healthcare is both complex and far from unambiguous and therefore warrants further research.
Conclusions and relevance to clinical practice
The results indicated that ignorance about transgender people in general was widespread among healthcare professionals, and this may result in transgender people delaying or avoiding seeking medical help. The most important thing for the informants was to be treated like any other patient. Therefore, it is important to educate healthcare professionals in the subject to improve the treatment of transgender people. It is essential to use the correct name and pronouns and not to question them routinely, especially when other patients may hear the conversation. By also noting the person’s correct name and pronoun in the medical record, embarrassing meetings may be avoided and healthcare professionals may thereby avoid questioning transgender people when they are seeking medical help.
Through training, clear guidelines and the development of adequate journal systems, healthcare professionals’ understanding of the patient’s gender identity can be facilitated. All in all, this will reinforce the prerequisites for person-centred care in appointments with healthcare professionals within the healthcare system. However, describing and visualising the experiences of transgender people in their meetings with healthcare professionals may also contribute to decreasing the healthcare professionals’ lack of knowledge about their special needs. This may result in transgender people not feeling that they have to educate healthcare professionals. This knowledge may lead to more respectful meetings and also help transgender people to dare to seek medical help when needed.
Footnotes
Author contributions
Study design: TB, LS, ER, NS, BJ, MW. Data collection: TB, LS, ER, NS. Data analysis: TB, LS, ER, NS, BJ, MW. Manuscript preparation: MW. Manuscript review: MW, TB, AA.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.