
Abstract
Providing care and support to persons with intellectual disabilities (ID) requires in-depth knowledge about ID and challenging behaviour (CB) as well as communication and interaction. Knowledge deficiencies in these areas may prevent staff from understanding their clients and their behaviours, particularly those behaviours considered to be challenging. The aim of this study was to explore staff’s perceptions about CB among clients with ID in residential settings before and after a web-based training programme using the survey instrument ‘Checklist of Challenging Behaviour’ (CCB). The CRe-DEPTH guideline has served as a guide in this study. Upon completion of the training, staff perceived a reduced frequency of CB as well as reduced management difficulty of CB among clients. As such, training should routinely be offered to all staff in residential settings, but also healthcare professionals in general responsible for caring for clients exhibiting CB to ensure, improve and reinforce the quality of care and support provided to them.
Background
The provision of effective care and support by staff in residential settings to individuals with intellectual disabilities (ID) is crucial.1,2 Individuals with ID living in a residential setting are referred to as clients. As this study concerns the residence staff's perceptions of individuals with ID, the term ‘client’ will be used in this work as well. Although improving the quality of life and providing effective support to clients can be satisfying for staff,1,3,4 the work requires knowledge and skills in communication and interaction.5–8
Knowledge deficiencies in care and support provided to clients can therefore be a cause of concern and a source of uncertainty among staff, 8 in many instances preventing them from fully understanding their clients and their clients’ behaviours. This can be particularly problematic when it comes to challenging behaviour (CB), as understanding and knowledge concerning the dynamics underlying CB is a crucial foundation for coping with, supporting, and interacting with clients exhibiting such behaviours.9,10
Within the research field of ID, CB is a term used to describe behaviours that have physical or social impacts on individuals who exhibit those behaviours and/or their surroundings. 11 CB can be divided into aggressive behaviours, such as physically hitting others, injuring oneself, or otherwise acting in a physically aggressive manner not necessarily directed at other people. 12 Such behaviours, even when not directly harmful to oneself or others, e.g. destruction of property or persistent screaming, can be difficult to manage and address by staff. 11 In recent years, stereotyped behaviour has been highlighted in connection to the definition of CB. Also, the researchers contend that dimensions such as the frequency and severity of CB should be considered when attempting to determine – and rate – which behaviours are challenging. 13 From a functional viewpoint, CB is and should be considered as a means by which persons with ID communicate their will and intentions to those in their surroundings, since other means may not be available to them due to impaired communication.14,15
Communication and interaction, especially with clients who have impairments in these areas, such as those with ID, is considered important by staff. 16 Earlier studies have shown that staff working with persons with ID reported CB as a problem they could not always address in the desired manner while performing their work duties.4,17,18 This predicament was shown to often generate stress, anger and powerlessness among staff, increasing the likelihood of burnout.17,19–21 Moreover, being unable to effectively address CB had a definitive impact on the interactions between staff and their clients, leading the former to adopt less appropriate coping strategies, e.g. avoiding their clients and being emotionally distant when providing care. 22
Several reviews have shown that educational training in communication with persons with ID that goes beyond verbal means should be a priority in healthcare.7,23 This is particularly crucial in the context of residential settings as the social networks of those with ID living in these facilities are often limited compared to those of the general population. The staff in a residential setting typically comprise a large part of their clients’ social network. 24
Earlier research has demonstrated that health problems occur to a greater extent in persons with ID compared to the general population. 25 There is also growing evidence that health problems are linked to increased instances of CB among those with ID.26,27 As CB may marginalize persons with ID from society and thereby prevent them from accessing, e.g. health and medical care,11,15 their health problems may be exacerbated even further.
As experienced by healthcare professionals, e.g. nurses, nationally and internationally, exposure to persons with ID during the nursing education period is often insufficient. 23 Similarly, healthcare professionals within the ID sector have identified the need for enhanced training that will better prepare them for working with persons with ID.7,28
Research has been conducted worldwide on various educational initiatives targeting healthcare professionals within the ID sector to enhance their readiness to communicate and interact with clients.29,30 Most such studies have reported positive outcomes among participants. In Sweden, a pilot-tested web-based training programme for staff to improve communication and interaction with adults with ID at a residence has yielded beneficial outcomes, including the appreciation of the staff. 31 The training was constructed based on a theoretical model developed by Farrell et al. 32 The model was built on the assumption that CB is caused by communication disruption between staff and persons with ID. The results of the study 31 demonstrated a reduced frequency of CB in the form of aggressive behaviour in the client in addition to reduced difficulties managing CB as perceived by the staff. Given this result, we wanted to take advantage of the knowledge acquired 31 and conduct a larger study to improve staff understanding of the underlying mechanisms behind CB and to generate greater knowledge about communication and interaction with persons with ID, thereby promoting better health and improved quality of care and support for this population. Helping staff to better understand and be better prepared prior to meeting, communicating and interacting with persons with ID, especially concerning addressing CB, could also help to establish and maintain a healthy work environment. Since the basic assumption was that CB is a consequence of interrupted communication and interaction between staff and persons with ID, our hypothesis was that by introducing web-based training focusing on ID and CB as well as communication and interaction, the frequency of CB and degree of management difficulty of CB in daily care would be reduced. Measurements of the frequency and degree of management difficulty of CB as perceived by staff before and after the web-based training programme served as the training's outcome value assessed in this study.
Aim
The aim of this study was to explore staff’s perceptions about CB among clients with ID in residential settings before and after a web-based training programme, specifically addressing ID and CB as well as communication and interaction.
Research questions
Do staff report a lower frequency of CB among clients with ID in residential settings after the web-based training?
Do staff report a lower degree of management difficulty of CB among clients with ID in residential settings after the web-based training?
Methods
A quantitative approach is considered appropriate to respond to the aim of this study with the associated research questions. CRe-DEPTH, Criteria for Reporting on Development and Evaluation of Professional Training interventions in Healthcare, has served as a guide in writing and structuring this study. 33
Design
A within-subjects study design was applied in which the participants were exposed to the treatment – in this case, web-based training – and measurements were made before and after treatment exposure to examine any potential changes that occurred. 34
Setting
The web-based training was offered to staff in residential facilities for adults (aged 18 years and above) with ID in a medium-sized city in Sweden. The staff in these facilities were support assistants and support educators whose main task is to support and assist the clients in structuring their daily lives, for instance, when to work, when to carry out other activities including housework. Depending on the needs of the clients, staff also provided supportive health and medical care. Staff density was based on the number of clients who lived in the residence, the severity of the clients’ ID, and the time of day. The staff usually had access to an office with one or two computers used for administrative tasks, for example documentation. However, at some residences, the staff did not have access to an office.
The web-based training
The web-based training in this study was built upon the same concept applied in the study by Antonsson et al., 31 in which the web-based training included both text sections and streamed lectures covering different subjects, for example definitions and characteristics of ID and CB, as well as underlying causes such as mental illness and its consequences. Furthermore, attention has been paid to communication and interaction in addition to the availability of coping and prevention efforts. These subjects were discussed in relation to the quality of care and support. Similarly, the values and feelings of the staff themselves, along with the culture and the physical environment at the workplace, were highlighted in relation to the development of CB among clients.
In this study, further development of the web-based training was undertaken by the third author who was already familiar with it, and the fourth author. Both the text section and the streamed lectures were constructed to cover a wide range of knowledge, from basic information to more theoretical discussions linked to scientific findings within the area to meet the differences of the participants in terms of prior knowledge. In total, there were 12 streamed lectures with lengths of 4.5–14 minutes. The text section consisted of three chapters, each of which ended with a question to stimulate self-reflection. The participants were prompted to discuss these self-reflections with co-workers. Lastly, the participants were given opportunities to take part in authentic cases from previous research where meetings between staff and persons with ID and CB were studied.
Data collection
Sample
Cluster sampling was conducted whereby 20 residential facilities were included. All staff in those residences were offered web-based training and invited to participate in this study.
Survey instrument: Checklist of Challenging Behaviour.
The Checklist of Challenging Behaviour (CCB) was used as a survey instrument to systematically rate the frequency of CB among clients and the difficulty in managing these behaviours as perceived by participating staff (see Table 1).
Checklist of challenging behaviour with frequency and management difficulty of challenging behaviour.

Values: mean, SD = standard deviation, n = number of participants, z = test statistic of Wilcoxon signed rank test. r = effect size: 0.1 = small, 0.3 = medium, 0.5 = large.
The CCB was developed by Harris et al., 12 who assessed the instrument's content validity and inter-rater reliability. The researchers concluded that the instrument was a reliable indicator of the presence or absence of CB. Since its development, the CCB has been used in several studies internationally.35–38
In the study by Antonsson et al., 31 the CCB was first translated from English to Swedish and then back-translated into English before the Swedish version was applied. The Swedish version of the CCB was employed in the current study. The CCB includes 41 items related to topographies of aggressive and other CB divided along the dimensions of physical violence/aggressive behaviour, property destruction, miscellaneous behaviour, and mental illness. To answer the research questions, the focus was placed on measuring the frequency of different CB and the degree of difficulty in managing these CB as perceived by staff in the past three months.
All measurements were based on a five-point scale. For frequency, 1 = never, 2 = once a week, 3 = a few times a week, 4 = once a day and 5 = a few times a day. For management difficulty, 1 = no problem, 2 = slight problem, 3 = moderate problem, 4 = considerable problem and 5 = extreme problem.
The CCB was distributed to staff in hard-copy format, as it was believed that doing so would make it easier for the staff to complete and return the survey instrument. Reply envelopes were attached to the CCB so that the staff could return them by mail.
Procedure
In April 2018, the managers and staff were provided with all relevant information about the research and the web-based training in both written and verbal form, and were fully informed that participation was voluntary. Subsequently, the staff were asked to complete CCB for the first time. In May 2018, the web-based training was made accessible to staff with the instruction to complete the training within six months. In November 2018 – the staff were asked to complete the CCB a second time. For each of the staff, 10 hours were allocated to complete both the training and the CCB. Via the learning platform where the web-based training was delivered, the research group received information about whether the staff had logged in to the training or not. However, information on whether the staff had completed the training was not available. Two reminders were sent, at three-week intervals, to those staff who has logged in to the training but whose CCB had not been received. A returned completed CCB was considered to constitute written consent to participate in this study.
Data management and analysis
All CCB responses were transferred to a digital format via the FileMaker Pro 12 software program. Then, the data were exported to IBM SPSS Statistics 25, for the statistical calculations to be carried out. First, descriptive analysis was performed to summarize the characteristics of the sample. All returned CCB with rated sub-items both before and after training were included in the following analysis. Central measurements were presented as the mean and dispersion by standard deviation. As the data were represented on an ordinal scale, the Wilcoxon signed-rank test was used to determine whether alterations existed between the responses before and after training. 39
Considering the number of calculations performed, a significance value of p < 0.05 was established. In addition, p-values < 0.1 were interpreted as tendencies. To contribute to indications of practical significance, a correlation coefficient r was calculated by converting the z-values, as described by Pautz et al., 40 of those sub-items with significant values. According to the rule of thumb for interpretation of Cohen's 41 r: 0.1 = small effect size, 0.3 = medium effect size and 0.5 = large effect size.
Findings
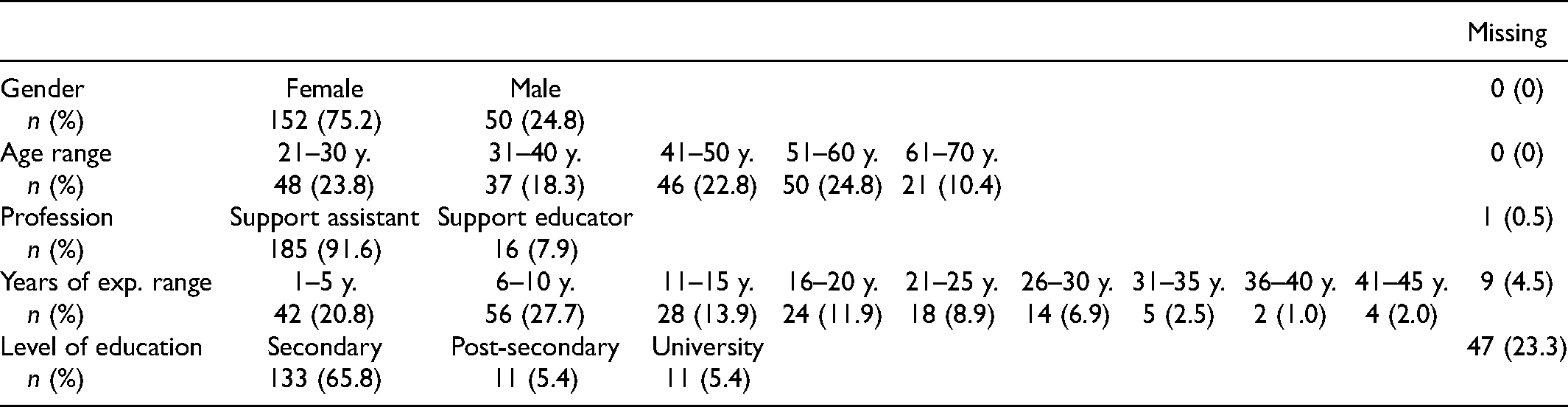
A total of 202 participants accepted the invitation to participate in the survey. The demographic description of the sample can be found in Table 2. Of the participants, about 75% were women. The ages of the participants were fairly evenly distributed, between 20 and 60 years old, with a gradation of 10 years and a range of 21 to 67 years. Of those who provided information about their job type and level of education, approximately 92% worked as support assistants in the facilities, and most had completed secondary education. Most participants had 6–10 years of work experience; second-most had 1–5 years of work experience; followed by those who had 11–15 years of work experience. Quite a few participants had up to 45 years of work experience.
Demographic description of the sample.
The average response rate concerning the frequency of CB was 41.44% (range 35.64–43.56%), while the average response rate regarding management difficulty of CB was 30.04% (range 16.83–37.62%). The results of the calculations can be found in Table 1.
Frequency of challenging behaviour
The analysis showed that staff self-reported a significantly lower degree of frequency on the dimension of property destruction, on the sub-item damaging others’ clothes, furniture, or other objects (z = −1.994, p = 0.046, r = 0.15) after training. Similarly, a significant difference was revealed on the dimension of mental illness, on the sub-item obsessional behaviours, after training (z = −2.657, p = 0.008, r = 0.20). However, the effect sizes were considered small. Apart from that, the calculations also showed tendencies towards significance on the sub-items biting, throwing things at people and breaking windows (Table 1).
Management difficulty of challenging behaviour
The analysis revealed that, after training, staff self-reported a significantly lower degree of management difficulty on all sub-items on the dimension of property destruction as follows: damaging own clothes, furniture or other objects (z = −2.179, p = 0.029, r = 0.23), damaging others’ clothes, furniture or other objects (z = −1.989, p = 0.047, r = 0.18), slamming doors repeatedly (z = −2.646, p = 0.008, r = 0.22), breaking windows (z = −2.388, p = 0.017, r = 0.22) and, lastly, other behaviours (z = −2.095, p = 0.036, r = 0.19). Further on, three sub-items on the dimension of mental illness also showed the same trend. These sub-items were obsessional behaviours (z = −2.413, p = 0.016, r = 0.20), upset speech (z = −2.275, p = 0.023, r = 0.19) and other behaviours (z = −2.145, p = 0.032, r = 0.20). Here as well, the effect sizes were considered small. Similarly, some tendencies towards significance were identified on the sub-items absconding, causing disturbance at night, other miscellaneous behaviours and depression (Table 1).
Discussion
The findings showed that staff reported a lower frequency of CB among their clients as well as a significant reduction in management difficulty of CB after the web-based training. Since, according to Hewett 14 and to Walsh, 15 CB is and should be considered as a means by which persons with ID communicate, eliminating CB could, in this instance, also mean taking from them their only means to communicate with the outside world. On the other hand, the observed reduction in the frequency of CB after the web-based training may have been due to enhanced knowledge and understanding by staff of CB among their clients, which could have consequently led them to no longer consider these behaviours as challenging. In earlier research, it was found that the amount of knowledge possessed by staff could act as a significant predictor of their behavioural responses to CB. 42 Accordingly, it is reasonable to suspect that reduced CB as perceived by staff may have been due to their enhanced knowledge of such behaviours, which impacted their views and behavioural responses to CB. This, in turn, could improve interactions by staff with their clients and consequently the former's perceptions of management difficulty of such behaviours. Indeed, the present study did not measure staff skills or knowledge, thus any improvements in these areas because of training were not captured. Likewise, measuring staff–client interactions was beyond the scope of this study, but it is nonetheless meaningful to consider in this context. Some aspects of interaction were noted in a parallel interview study conducted as part of the evaluation of the web-based training. 10 In these interviews, staff revealed, for example, that, after the web-based training, they recognized the importance of allowing clients the space and time to express themselves when they were experiencing an emotional episode, as doing so could ultimately benefit their interactions with clients. 10
The descriptive characteristics revealed that most of the study participants had completed secondary education; in addition, quite a few of the participants were aged 21–30 years, and many had the lowest range in terms of years of work experience: 1–5 years. As jobs within this sector are considered to be highly complex, 43 it would be unreasonable to expect all of the staff to have the capability to perform all job duties without sufficient opportunities to expand their knowledge and improve their skills with the support of the relevant healthcare organization.
As shown, the perceptions of healthcare professionals in earlier studies also reinforced the fact that knowledge concerning how to work with clients with ID was insufficient despite the education they had received.7,23,28 This finding corresponds with those generated in a recent study in the Swedish context. 44 In addition, as already mentioned, persons with ID experience a higher prevalence of health problems 25 and may be marginalized in terms of access to health and medical care.11,15 To effectively meet the complex needs of persons with ID, in addition to job-specific knowledge, collaboration with interprofessional teams is also recommended. 45 As such, educational investment should be made to increase knowledge of the different professions in the interprofessional team in the sector.
Whereas several studies have reported an increased likelihood of burnout among staff working with persons with ID but who lack skills in the management of CB,19–21 the association between exposure to aggressive CB and burnout among staff could not be demonstrated. 46 This suggests that exposure to aggressive behaviour alone is not a causal factor for burnout, but instead that such exposure in combination with a lack of sufficient knowledge and understanding for managing CB may be a root cause. As such, enhancing knowledge among staff responsible for caring for persons with ID who exhibit CB may help them better manage these behaviours and thereby improve the well-being of both staff and clients.
Lastly, web-based training, as an approach, should be given some consideration in terms of both its benefits and shortcomings. On the one hand, such training can provide participants with the freedom and flexibility to control how and when to complete the training; on the other, however, the training places high demands on the participants’ own responsibility. 47 In this study, the procedure used to deliver the web-based training was not considered. More specifically, the consistency and accuracy of how the training was delivered were not investigated. When it comes to job training, organizational support plays a crucial role in improving learning outcomes. 48 Attention should therefore be paid to the procedures used to implement staff training and support such that staff have greater opportunities to acquire the knowledge needed to provide better care and support to vulnerable segments of the population.
Strengths and limitations
This study had some limitations. Data collection relied on self-report measurements, which are prone to biases, such as social desirability bias, as noted by Outar and Rose 49 as well as Story and Tait. 50 Consequently, the frequency of CB – and especially the degree of difficulty experienced when managing CB – may have been underreported, as admitting to experiencing problems in these areas could be perceived negatively regarding one's professional reputation and image. Nevertheless, self-reports represent one of the most straightforward methods used to measure emotion-related constructs in social and psychological research.51,52 Moreover, self-report instruments such as the CCB employed in the present study allow participants the freedom and flexibility to complete such assessments at a time most convenient for them. 52
The range of response rates in this study did not fully cover ≥ 40%, as recommended. 50 However, a downward trend in the response rate has been identified in healthcare provider surveys. 53 In this study, the response rate of participants was considered twice, i.e. both before and after training. This may have placed higher demands on the participants. The average response rate concerning the frequency of CB was nonetheless over 40%, whereas that concerning management difficulty of CB was not. One explanation for this could be that the question concerning the management difficulty of CB could have been considered a follow-up question to that regarding the frequency of CB. Therefore, if a participant rated the frequency of CB as 0, then that participant would have skipped the question concerning the management difficulty of CB. Consequently, the response rate concerning management difficulty of CB was not as high as that for the frequency of CB. Further, we suggest that measurements linked to individual clients should be included in future research, as doing so could contribute an additional, accurate measure; one that reflects the effects of training.
Another limitation of the current study was the research design. In a within-subjects design, factors that may have influenced scores on the post-test, such as maturation and test effects, could not be controlled. 54 Moreover, demand effects should be another concern in this regard. 34 Nevertheless, despite these aspects, a within-subjects design has its advantages, e.g. the internal validity does not depend on random assignment. We suggest, therefore, future research should consider combining a within-subjects design and a between-subjects design to help verify the effects of training. 34 Likewise, an investigation of the longitudinal effects of training could have contributed valuable knowledge in this connection. This study nonetheless contributed by providing directions for future research in this area.
Conclusion
Working with persons with ID and CB places high demands on staff, especially those who work in residential facilities for persons with ID. As mentioned above, many healthcare professionals do not feel sufficiently equipped for this job even after completing the required education. Considering the complexity of meeting the needs of persons with ID, different competences gleaned from collaboration with interprofessional teams are recommended for implementation in the training of healthcare professionals. Employers have the primary responsibility in this regard, ensuring that all staff are trained in the necessary competences to sufficiently carry out their job duties. We therefore recommend that such multi-competence training be offered to all healthcare professionals involved in caring for persons with ID, and that it should be given routinely to maintain and reinforce the knowledge and skills gained from the training.
Footnotes
Acknowledgements
We would like to give special thanks to Ulf Isaksson, Associate Professor at Umeå University, for support in FileMaker Pro 12. Also, we would like to thank the staff for their participation as well as the management team for their ongoing support during the study.
Ethics approval
Approval has been granted by the Swedish Ethical Review Authority, Dnr 35517. This study has followed ethical principles in accordance with the Helsinki Declaration. 55 Ultimately, this study intended to provide staff with the opportunity to acquire essential knowledge to support their work with persons with ID and CB, thereby improving the quality of care and support to one of the most vulnerable groups in our society. Participation was entirely voluntary. The confidentiality of all participants was ensured by excluding any information that could personally identify them. This study was registered in Clinical Trial, identification number NCT03390868.
Availability of data
Data are not available to anyone other than the members of the research group.
Author contributions
AT contributed to data management and led the writing of the article. Data analysis and interpretation were carried out by AT and AE-B. HA and CJ contributed to the conception and development of the web-based training and its implementation, and a portion of the data analysis. All authors contributed to the critical revision of the article and in obtaining final approval.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.