
Abstract
The role of clinical nurse educators is essential in improving the quality of mentoring, supporting students’ learning and professional development during clinical training. The purpose was to explore the competence profiles of clinical nurse educators and background factors associated with these profiles. Data of this cross-sectional study were collected from clinical nurse educators (n = 19) at Finnish university hospitals, using two instruments measuring the competence of healthcare educators. Data were analysed with K-means clustering and two profiles were identified based on sum variables. Significance between the differences of Profile 1 and Profile 2 was evaluated by comparing independent groups. The STROBE checklist was used as the reporting guideline for the manuscript. Educators’ competence varied between intermediate (2.50–3.49) and high (≥ 3.50) levels, and self-assessment of the Profile 1 was average higher than those in Profile 2. The results can be used to identify and develop the competence of clinical nurse educators and to consolidate the role and position of clinical nurse educators within healthcare education.
Introduction
The competence of clinical nurse educators influences their ability to provide high-quality nursing education and mentoring during clinical practice, and thus affects the competence and commitment of new professionals in the field of nursing.1,2 The healthcare sector is constantly changing with the introduction of new patient care treatment recommendations, nursing practices, and organizational structures, as well as a changing demographic structure. It is therefore essential to ensure that student nurses have positive experiences during their education and clinical practice that reinforce their commitment to the field and the development of their professionalism.2,3
The roles of clinical educators vary between countries. For example, in Finland, positions for clinical nurse educators have become available in the last decade, mainly within hospital organizations. 4 However, in other countries clinical nurse educators are employed in higher education institutions or work jointly in higher education institutions and clinical nursing units. 5 In some countries such as Australia, universities and healthcare practice units have co-developed clinical education units or dedicated education units that provide clinical placements for nursing students. 5 The positions of clinical nurse educators also differ between the Nordic countries. For example, clinical nurse educators in Sweden are employed by universities and act as the links between the university and clinical placements. 6 Conversely, in Finland, nurse educators (working at education institutions) are primarily responsible for organizing clinical placements in cooperation with clinical nurse educators. 4 The job titles of clinical nurse educators also vary between and within countries; examples include clinical facilitator, 1 clinical instructor, 7 clinical nurse lecturer, 6 clinical educator, 8 clinical teacher in nursing, training coordinator, and teaching coordinator. 4 This variation in duties, job titles, and positions creates uncertainty about the competences and roles of clinical nurse educators, making it important to strengthen the competence of clinical nurse educators and emphasize the importance of the role in nursing education.8–10
Despite the differences in the duties and employment status of clinical nurse educators between countries, there is clear evidence that nursing students in all countries face similar problems and need effective support during their clinical practice.11,12 We also know that nursing personnel are often responsible for students’ mentoring and overseeing their clinical practice, but nursing personnel may lack pedagogical expertise relating to student mentoring.1,13 It is therefore essential for clinical nurse educators in hospital organizations to be actively involved in mentoring students’ clinical practice and to offer student mentors (registered nurses) their expertise and support in mentoring and guiding nursing students’ learning processes. In addition, it is important that they participate in the development of collaborative and evidence-based nursing by ensuring a high quality of people-centred care.1,2,14
Studies conducted around the world over the last decade have shown that clinical nurse educators experience uncertainty about their own competence because of the lack of consensus concerning their roles and job descriptions, and tensions between clinical nursing practice and theoretical working practices. 10 Additionally, research indicates that the work of clinical nurse educators is essential for high-quality evidence-based nursing practice and student mentoring.7,9 Consequently, there is a need for further research on the competencies of clinical nurse educators and for the national and international development and harmonization of their roles.9,10 An individual's abilities, knowledge, attitudes, skills, values, and experiences can be defined by the concept of competence, all of which allow an individual to perform their duties at the expected level and to achieve appropriately set goals. 15 Individual's professional competence is often understood as an ability to make decisions and solve problems in practice for the benefit of individuals and the community. 16
Several wide-ranging areas of competence have been defined in the social and healthcare sector, relating to both practice and education.2,17 Competence areas included in a recent competence model for social and healthcare educators 17 include subject and curriculum, evidence-based practice, mentoring students in professional competence development, student-centred pedagogy, digital collaborative learning, cultural and linguistic diversity, leadership and management, and collaboration and societal competence.2,17 Clinical nurse educators coordinate collaboration and consultation between hospital organizations and educational organizations to achieve strategic goals in healthcare education.1,4 For clinical learning environments to serve both students and student mentors, clinical nurse educators must know and understand the content and goals of the nursing curriculum.7,9 In addition, their responsibilities include organizing, mentoring, and supporting learning in clinical practice and developing research topics and projects. High-quality student mentoring can be guaranteed by ensuring the mentoring and professional competence of clinical nurse educators and nursing staff.2,13,18 To our knowledge there is currently no competence model for clinical nurse educators. However, a competency framework for clinical nurse educators has been established in one Finnish university hospital. 18 In this framework, clinical nurse educators’ competence is evaluated with respect to following distinct areas: research-based development of clinical education and nursing, production of health science research evidence, demonstration of the effectiveness of clinical education and nursing, promotion of recruitment of competent nursing staff, quality assurance of clinical learning environments, strengthening the professional competence of nursing staff and nurse students, and managing the didactics of clinical nursing science. In this study we aimed to operationalize these areas in an empirical study and measure the competence of clinical nurse educators in each area in order to i) identify competence profiles within this population and ii) identify background factors affecting the competences of clinical nurse educators. The objective of the study was to generate knowledge about the competence and development needs of clinical nurse educators in order to strengthen their role within healthcare education.
The research questions were:
What competence profiles can be identified among clinical nurse educators employed at university hospitals? What background factors are associated with these competence profiles?
Methods
A cross-sectional study design was used because the study is based on observational data on clinical nurse educators’ competence at the time of measurement. Guidelines for reporting observational studies, the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist, was used to confirm the study design and methods, and to increase the validity of study's findings. 19
Participants and settings
All clinical nurse educators (N = 31) at five Finnish university hospitals were sent letters (distributed by named contact persons at each hospital) inviting them to participate in the study. The letters included information on the study and how to complete the electronic survey as well as a data protection statement. Data were collected from August to November 2020. The questionnaire was completed by 19 clinical nurse educators at four university hospitals, giving a response rate of 61%.
The inclusion criteria for participating clinical nurse educators were: 1) completion of at least 60 ECTS credits at a university or university of applied sciences, during professional teacher education, or through education science; 2) completion of a master's degree or higher qualification; and 3) work experience in coordinating clinical placements and/or mentoring, and in supporting the mentoring and professional competence of nursing staff.
Instruments
Data were collected using the Health and Social Care Educator's Competence instrument (HeSoEduCo) 20 and the Competence of Clinical Nurse Educators instrument. A Likert scale ranging from 1 to 4 (1 = strongly disagree, 4 = strongly agree) was used to score the items of both instruments. The HeSoEduCo instrument has previously been validated and has been used to collect data from social care, healthcare, and rehabilitation educators working in higher education institutions. Despite their different operating environments, healthcare educators in higher education institutions and hospital organizations require the same competences, making this instrument suitable for assessing the competence of clinical nurse educators in hospital organizations. The HeSoEduCo instrument includes 43 items representing eight sum-variables corresponding to the following competence areas: leadership and management, digital collaborative learning, evidence-based practice, collaboration and societal competence, cultural and linguistic diversity, subject and curriculum, student-centred pedagogy, and mentoring students to develop professional competence. 20 Two of these competence areas had low Cronbach's alpha scores (0.43 for mentoring students to develop professional competence and 0.57 for collaboration and societal); the rest had scores between 0.76 and 0.95.
The Competence of Clinical Nurse Educators instrument was developed to measure the self-assessed competence of clinical nurse educators in hospital organizations and was tested in this study. The original instrument included 15 items representing four sum-variables relating to distinct competence areas based on a competence framework. 18 The instrument's structure was investigated by performing exploratory factor analysis using the Kaiser–Meyer–Olkin (KMO) test (0.615) and Bartlett’s test (218.433, df = 105, p < 0.01) with Principal Axis Factoring and Promax rotation (Table 1). An evaluation of the factor model's functionality showed that the eigenvalues of its factors were > 1 and their communality was ≥ 0.30. 21 The final factor model was constructed from three factors that cumulatively explained 70.36% of the variance in the data. Factor 1, Competence in ensuring and developing the quality of student mentoring and clinical learning environments, explained 40.23% of the total variance and had an eigenvalue of 5.23. Factor 2, Competence in promoting the availability of clinical placements, explained 15.60% of the total variance and had an eigenvalue of 2.02. Factor 3, Nursing competence, explained 14.53% of the total variance and had an eigenvalue of 1.88. The Cronbach's alpha coefficient, which describes the internal consistency of the instrument, ranged from 0.87 to 0.88. 22
Exploratory factor analysis and Cronbach's alpha values of the clinical nurse educators instrument (n = 19).
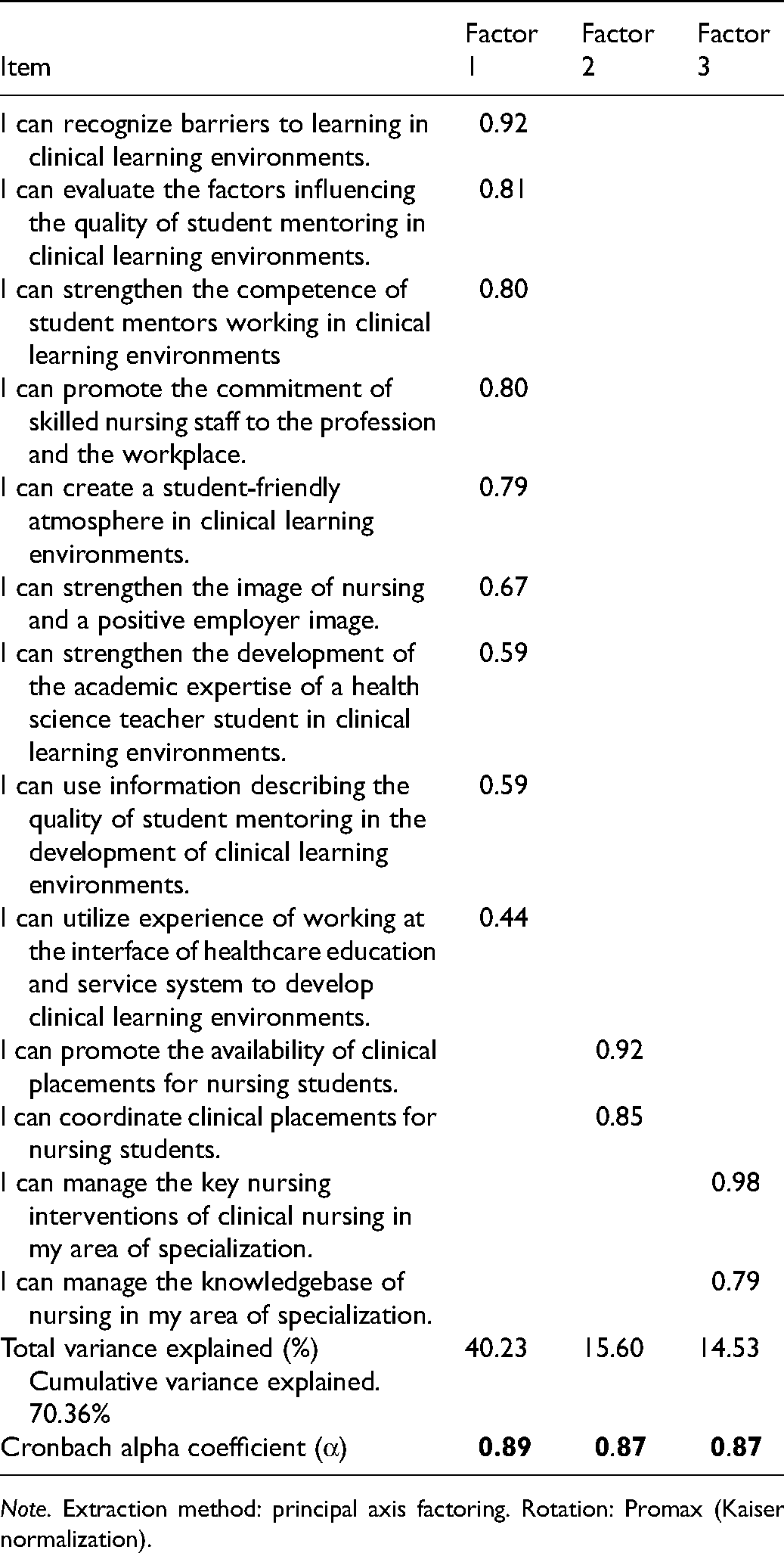
Note. Extraction method: principal axis factoring. Rotation: Promax (Kaiser normalization).
Data analysis
The gathered data were analysed using IBM SPSS 27.0 Statistics. The background factors were analysed by computing means and percentages. Eleven sum-variables were formed from the data and clustered into distinct competence profiles (cluster groups) designated Profile 1 and Profile 2 by using K-means clustering. Clustering is an algorithmic method designed to group datapoints by similarity. 23 While it is rarely used in nursing science, it has proven to be highly effective in a variety of contexts, including when grouping individuals based on competence.3,24,25 The purpose of competence profiling in this way was to identify differences in competence between groups that could be used to support the development of clinical nurse educators’ professional competence. The relationships between the background factors and the competences of the participants were tested using the t-test in the case of continuous variables and Fisher's exact test for classified variables. A Mann–Whitney U-test was used to compare differences in competence levels between two clustered profiles. Results are reported as means and standard deviations, and a significance threshold of p < 0.05 was applied. 21 The effect size of the differences between the competence profiles was evaluated by computing Cohen's d (interpreted as 0.2 = very small, 0.5 = reasonable, 0.8 = large, 1.3 = very high). 26 The competence levels of clinical nurse educators were classified based on their Likert scale responses: means of ≤ 2.49, 2.50–3.49, and ≥ 3.50 were taken to indicate low, intermediate, and high competence, respectively.
Ethical considerations
Throughout this study, good scientific practices 27 were followed in pursuit of honesty, transparency, accuracy, and diligence during the research process. 28 Permission to conduct the study was obtained from all of Finland's university hospitals in accordance with Finnish regulations concerning research practices. 29 Participants were informed in writing about the study and the voluntary nature of their participation. Due to the small sample and the small number of clinical nurse educators in Finland, the gender distribution of the participants and their current job titles were not broken down by competence profile to ensure anonymity. Data collected and generated during the study were processed and stored in compliance with the EU data protection regulations 30 and the Data Protection Act, 31 in line with which the data were archived at the end of the investigation.
Results
The study's respondents were 19 clinical nurse educators from four Finnish university hospitals. Most of the respondents were women. The mean age of participants was 47 years. Of the respondents, 84% had a master's degree from a university of applied science, 11% had a master's degree from a university and 5% had a doctoral degree. Respondents had completed pedagogical studies in health science teacher education (52.6%), in vocational teacher education (39%), and in education science teacher education (5.5%). On average, the respondents had nine years’ of work experience in the field corresponding to their degree and seven years of work experience as an educator in a hospital organization.
Competence profiles of clinical nurse educators in university hospitals
The competence of clinical nurse educators in Finnish university hospitals generally ranged from intermediate to high. Two competence profiles were identified among the respondents by K-means clustering, with statistically significant differences in competence levels for nine of the 11 sum-variables considered in this work (Table 2). Profile 1 contained 58% (n = 11) of the respondents and Profile 2 contained 42% (n = 8). The effect sizes of the differences between the profiles ranged from reasonable (0.34) to very high (1.88), showing that the sample size was adequate (Table 2).
Clinical nurse educators’ background factors and competence profiles (n = 19).
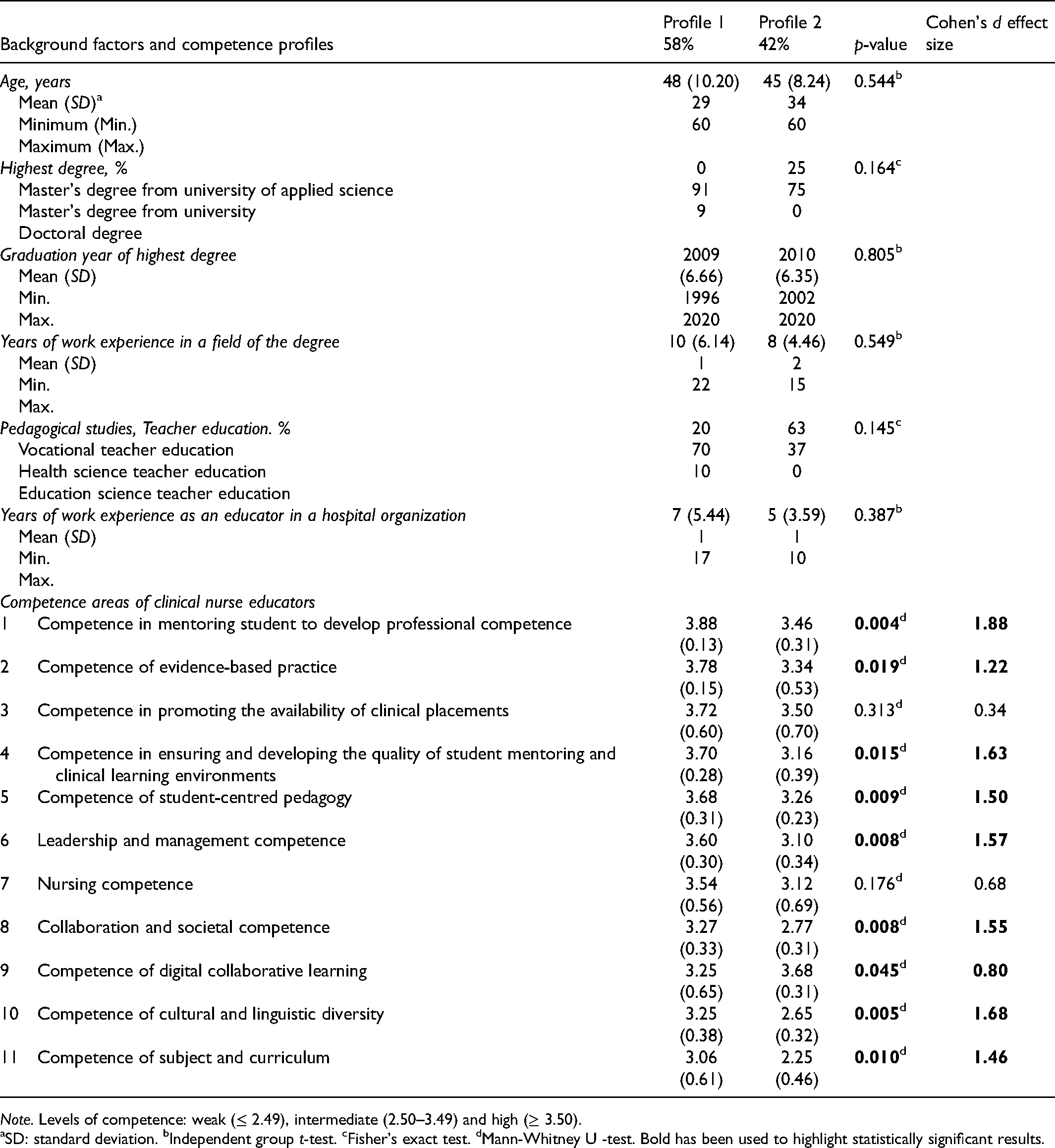
Note. Levels of competence: weak (≤ 2.49), intermediate (2.50–3.49) and high (≥ 3.50).
aSD: standard deviation. bIndependent group t-test. cFisher's exact test. dMann-Whitney U -test. Bold has been used to highlight statistically significant results.
The area in which Profile 1 respondents had the highest levels of self-assessed competence was mentoring students to develop their professional competence (mean 3.88, SD 0.13). In addition, respondents with this profile reported high levels of self-assessed competence in the areas of evidence-based practice (mean 3.78, SD 0.15), ensuring and developing the quality of student mentoring and clinical learning environments (mean 3.70, SD 0.28), student-centred pedagogy (mean 3.68, SD 0.31), and leadership and management (mean 3.60, SD 0.30). Areas in which Profile 1 respondents reported intermediate levels of self-assessed competence were collaboration and societal competence (mean 3.27, SD 0.33), digital collaborative learning competence (mean 3.25, SD 0.65), and competence with cultural and linguistic diversity (mean 3.25, SD 0.38). Finally, Profile 1 respondents reported lower (albeit still intermediate) levels of subject and curriculum competence (mean 3.06, SD 0.61).
The area in which Profile 2 respondents had the highest self-assessed competence level was digital collaborative learning (mean 3.68, SD 0.31). Profile 2 respondents had intermediate self-assessed competence levels in mentoring students to develop their professional competence (mean 3.46, SD 0.31), evidence-based practice (mean 3.34, SD 0.53), student-centred pedagogy (mean 3.26, SD 0.23), ensuring and developing the quality of student mentoring and clinical learning environments (mean 3.16, SD 0.39), and leadership and management (mean 3.10, SD 0.34). Areas in which these respondents had lower intermediate levels of competence were collaboration and societal competence (mean 2.77, SD 0.31) and cultural and linguistic diversity competence (mean 2.65, SD 0.32). Finally, respondents in this profile had weak self-assessed levels of subject and curriculum competence (mean 2.25, SD 0.46).
Background factors related to the clinical nurse educator competence profiles
None of the background factors were significantly related to the clinical nurse educator competence profiles. However, there were noticeable differences in the average and percentage values of the background factors between the competence profiles (Table 2). Specifically, Profile 1 respondents had a higher mean age (48 years), length of work experience in the field of their degree (10 years) and experience as an educator in a hospital organization (7 years) than Profile 2 respondents. The highest degrees held by Profile 1 respondents were master's degrees from universities (91%) and doctoral degrees (9%), while in Profile 2 they were master's degrees from universities of applied sciences (25%) and master's degrees from universities (75%). The majority of the Profile 1 respondents had completed health science teacher education (70%) whereas the majority of Profile 2 respondents had completed vocational teacher education (63%). The graduation year for the highest degree ranged from 1996 to 2020 for Profile 1 and 2002 to 2020 for Profile 2.
Discussion
The study purpose was to investigate the competence profiles of clinical nurse educators and related background factors. Despite the clinical nurse educators’ wide-ranging and varied job descriptions and the fact that their position in healthcare education is not well-established, 32 clinical nurse educators at Finnish university hospitals mainly exhibited intermediate or high levels of competence. The two competence profiles identified in this work differed significantly in nine competence areas. The self-assessed competence of Profile 1 respondents was intermediate or high in all competence areas considered here, whereas that of Profile 2 respondents ranged from weak to high. Previous studies have found that the age, level of education, and length of work experience of clinical nurse educators are all positively related to their self-assessed competence.33,34 It thus seems likely that the differences in competence between the two profiles identified in this work are related to the corresponding differences in their background factors – specifically, age, level of education, and length of work experience. However, given the small sample size and lack of statistically significant relationships, such inferences should be made with caution.
A significant part of healthcare education occurs in clinical learning environments. 33 Clinical nurse educators have an important role to play in ensuring and developing the quality of clinical learning environments. Their competence in the development and implementation of evidence-based practices and in the management of subjects and curricula is essential for the successful merging of theory and practice. 35 In addition, skills in training student mentors in student-centred pedagogy are important in ensuring that students have positive experiences of clinical practice.32,33 The results presented here thus suggest that there is a need to narrow the gap between clinical nurse educators in these competence areas. Profile 2 educators exhibited weaker confidence in evidence-based practice, student-centred pedagogy, and ensuring and developing the quality of student mentoring and clinical learning environments than those in Profile 1. This deficit could potentially be reduced by improving the orientation and organization of resources.32,34
To improve subject and curriculum competence, which respondents in both Profiles considered to be their weakest competence area, opportunities for continuous education should be offered in cooperation with healthcare and educational organizations. 34 The importance of defining the roles and competence areas of nurse educators (representing higher education) and clinical nurse educators (representing clinical practice) needs to be more emphasized in order to achieve that kind of successful cooperation. Teaching adequate theory and clinical skills prior to clinical practice is cited as essential to support students’ learning process. 36 For education between theory and clinical practice to meet and to increase the subject and curriculum competence, it would be necessary to develop different models of collaboration between healthcare and educational organizations.34,36 The development of competence in collaboration is thus essential, both for nurse educators in clinical and educational environments and also in health science education at the university level during master's degree courses and teacher education. 17
The increasingly multidisciplinary and networked nature of both healthcare environments and society in general necessitates continuous adaptation from clinical nurse educators. 34 Such adaptation and structural change necessitates managerial competence and an understanding of leadership and management. They should also be able to take account of cultural and linguistic diversity in nursing and student mentoring, both within the professional community and in society.32,34 Clinical nurse educators with higher levels of education and greater lengths of work experience often reported higher self-assessed levels of competence within these areas.32,34,37 Accordingly, in this study, Profile 1 respondents reported higher levels of competence in these areas than Profile 2 respondents. Conversely, the background factors of Profile 2 (lower mean age and more recent year of graduation) may explain their higher levels of self-assessed competence in digital collaborative learning competence: younger age has been linked to healthcare professionals’ attitudes toward digitalization and technology development. 35 In addition, over the past decade, digital education tools have been introduced and used in the training of healthcare educators.35,38
The differences between the clinical nurse educator competence profiles may also have been influenced by variation in job descriptions and the poorly established position of clinical nurse educators within healthcare education. This work, like that of Van Nguyen et al. 34 and Gardner, 37 reveals a need to consolidate the position of clinical nurse educators and to identify and narrow differences in their levels of competence. Both the self-assessed competence of clinical nurse educators and their certainty about their role were reported to increase with work experience, consolidation of their position, and continuous education.34,37 The information on the different competence levels of clinical nurse educators at the national level presented herein could be used within healthcare organizations to guide the development of continuing education programmes for clinical nurse educators and to more clearly define their roles.
Strengths and limitations
The research data were collected using the HeSoEduCo and Competence of Clinical Nurse Educators instruments. The reliability of the results could be weakened by the low Cronbach's alpha coefficients of the HeSoEduCo sum-variables for Mentoring student into professional competence development (α = 0.43) and Collaboration and societal competence (α = 0.57); α = 0.70 is often regarded as the minimum acceptable value. 22 However, the coefficients may have been influenced the small sample size used in this work and the application of the instrument to a new target group of nurse educators. The Competence of Clinical Nurse Educators instrument was based on a previously developed competence framework 18 and its Cronbach's alpha coefficients were good, which strengthened the reliability of the results.
The generalizability of the study's results may be limited by its small sample size (n = 19) and the fact that it only included clinical nurse educators working in university hospitals in a single country. Despite the small sample, the Cohen's d effect size estimates for the differences between the competence profiles were generally large (i.e. in the reasonable to very high range). 26 The small sample size can be justified by the limited pool of potential respondents; the exact number of clinical nurse educators working in Finnish hospital organizations at present us unknown. However, a significant proportion of them work in university hospitals (N = 31) and, despite the varying roles of clinical nurse educators, their role is most important in such institutions. Clinical nurse educators working at five university hospitals were invited to participate, and eligible staff from four of these institutions completed the survey, giving an excellent response rate of 61%; response rates in electronic surveys are typically between 10% and 30%. 11
Statistically significant differences were found between the two identified competence profiles, validating the choice of analytical methods used in this work. The relationship between background factors and self-assessed competence should also be critically assessed given the impact of the small sample size on the reliability, generalizability, and clinical significance of the results. While the associations between the background factors and the self-assessed competence levels of respondents in the two profile groups were not statistically significant, the large p-values obtained in this work may have been at least partly due to the small sample size. 22 Thus, although the results presented here can only be considered indicative, they could have value in guiding the development of programmes designed to improve the competence of clinical nurse educators in healthcare organizations. The differences in self-assessed competence between the two competence profiles identified in this work could serve as a basis for developing continuing educational interventions and evaluating their effectiveness.
Conclusions
Clinical nurse educators in Finnish university hospitals generally evaluate their own professional competence to be either intermediate or high. High levels of self-assessed competence in mentoring students and developing their professional competence, ensuring and developing the quality of student mentoring and clinical learning environments all enhance the quality of clinical practice, which can increase the commitment of new healthcare professionals to the field during their education. The lowest-rated competence area, subject and curriculum competence, should be developed in cooperation with higher education institutions and healthcare organizations to meet the development needs and competence requirements of healthcare education and nursing. Additionally, efforts should be made within nursing management to identify and narrow differences in competence levels by assigning appropriate resources and implementing targeted continuous educational interventions that address the development needs of individual clinical nurse educators. Additionally, clinical nurse educators with stronger competence profiles should be encouraged to assist with the orientation and development of new educators. The results presented herein can be used for the leaders and education coordinators of healthcare organizations to identify and develop the competence of clinical nurse educators and to consolidate their roles within national healthcare education. To further develop methods for the education of healthcare educators, comparative research on the competence of healthcare educators in educational and healthcare organizations is needed. In addition, more research on the competence of clinical nurse educators in national and international contexts is needed to clarify their unified role and guide the development of their competences. The research method used in this study can be applied to conduct scientific knowledge of competence of clinical nurse educators in different countries.
Footnotes
Author contributions
The study was concepted and designed by VK, KM, NP, SR, MK and TH. VK and KM collected the research data. VK, KM and TH carried out an analysis of the data. The manuscript was written by VK, KM and TH. KM, NP, SR, MK, HK and TH reviewed and evaluated the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.