
Abstract
During the COVID-19 pandemic, nurses in the field examined were required to manage large numbers of patients suffering from COVID-19 in in-patient clinics necessitating relocation of registered nurses (RNs) from other clinics in the department to support the care of those patients. The aim of the study was to explore how RNs attribute meaning to their experiences during the organizational changes caused by the first wave of the COVID-19 pandemic. This descriptive phenomenological study is based on thematic analysis interviewing 47 RNs who either continued working in in-patient clinics, were relocated to in-patient clinics, or remained in out-patient clinics. The study methods complied with the COREQ. The main finding, ‘Sense-making in a changed reality of nursing’, shows how RNs attribute meaning or not to the organizational changes, and explains how meaning-making in RNs continuing in in-patient clinics reinforced their identity as RNs or, conversely, how feelings of meaninglessness in those relocated to in-patient clinics or remaining in out-patient clinics contributed to identity loss. This article suggests that managers, by paying attention to the narratives of meaning or meaninglessness in nurses during organizational changes, could be instrumental in managing the anger, frustration, and hopelessness arising from experiences of meaninglessness.
Introduction
COVID-19 has had major consequences and attracted the world’s attention since the beginning of 2020, not only affecting the healthcare system, but also having a tremendous impact financially and socially and on well-being in societies.1,2 The large-scale and rapid spread of the ongoing pandemic has changed the way hospitals and related health services operate and their priorities, leading to necessary organizational changes in hospital managers’ and health professionals' mindsets, routines, and patterns of action in most of the world. 3
The number of COVID-19 patients in need of hospitalization may have led to less attention being paid to patients with other severe illnesses, 4 giving rise to an undertreated group of patients as well as fear of entering hospital treatment for patients suffering from chronic illnesses. 5 This points to several potential ethical concerns regarding patient safety and patient rights. 6 In summary, the pandemic has had major consequences for COVID-19 patients and patients suffering from other diseases, and their numbers have led to overwhelming pressure on healthcare systems worldwide. 2
Likewise, the emergence of COVID-19 has affected registered nurses (RNs) around the world, and has had major consequences in terms of an unreasonably hard workflow, high infection rate, and mortality, 7 as well as increased anxiety, burnout, and depression among RNs.8–10 Earlier studies suggest that pandemics challenge the nursing profession in several ways. For many RNs, a pandemic creates a strong obligation to support patients; it creates, in others, a starting point for leaving the profession. 11 Reasons such as personal health risk, overload of work, and consideration for family are pervasive.12,13 Conversely, other articles have pointed to the fact that RNs and their managers, to a high degree, have managed and adapted with excellence to the increased workload during the COVID-19 pandemic. 14 In terms of management, several factors can be pointed to as contributing to the successful implementation of the organizational changes in healthcare, including the desire of RNs to help patients, the global worship of healthcare professionals in the media,15,16 as well as national and worldwide attention of politicians, the World Health Organization (WHO), and hospital management.7,17,18
The shortage of RNs – the dropout rate, and the struggle in many countries to retain and recruit RNs – makes the understanding of RNs' responses to major organizational changes, as is the case with COVID-19, even more necessary.19–21 A lack of political and managerial awareness regarding RNs’ responses to working conditions may further inhibit future possibilities to recruit and retain RNs. In conclusion, the understanding of RNs’ responses to organizational changes is of interest not only to RNs and managers but also to politicians, society, and patients.
Aim
The aim of the study was to explore how RNs attributed meaning to their experiences during the organizational changes caused by the first wave of the COVID-19 pandemic.
Method
The study is based on 47 participant nurses where 27 remained in out-patient clinics, 10 were relocated from out-patient to in-patient clinics, and 10 continued working in in-patient clinics. Data collection included 14 individual interviews and five focus-group interviews analysed in accordance with thematic analysis. 22 The study methods here are reported in accordance with COREQ. 23
Methodology
The methodology of this study is based on descriptive phenomenology, exploring the meaning RNs attribute to their experiences through organizational changes during the COVID-19 pandemic. The structure of these forms of experience involves what Husserl called intentionality, the directedness of experience toward things in the world. According to classical phenomenology, experience is directed toward, represents, or intends things only through concepts such as thoughts and ideas. This directedness to certain things makes up the meaning or content of a given experience, and is distinct from what things present or mean. 24 In other words, thoughts, memories, emotions, desires, and social activities are central to the understanding of meaning-making in participant RNs during organizational changes in the COVID-19 pandemic. 25
Context
The more than 200 nursing staff members in the department were notified by managers of a possible need to relocate RNs working in out-patient clinics and the laboratory into in-patient clinics. The underlying causes were an expected increase in resources for isolated COVID-19 patients and increased sickness absence among the nursing staff as the pandemic intensified. During March and April 2020, the department relocated 18 RNs to other work areas. Of these, 14 RNs were transferred from their position in out-patient clinics or the laboratory to in-patient clinics. A process was carried out in which the relocated RNs had to be trained and qualified in a very short time to upgrade their competencies to care for COVID-19 patients, contributing to such nursing care in a responsible manner. New, stricter hygiene requirements and isolation regimes were likewise implemented regarding standardization of the application and removal of protective equipment which was sometimes changed daily. The relocated RNs had to adapt quickly to a new work environment, colleagues, and nursing tasks. For all RNs working in in-patient clinics of the department, this was challenging. All had to get used to special requirements when caring for COVID-19 patients while managing the complex task of adapting to new guidelines and implementing them immediately.
Data collection
The present study draws its empirical data from a hospital department in Denmark in which the authors are employed as post-doctoral researcher and head nurse of the department. A pragmatic sample of participants took place in the department's eight clinics: one laboratory, four out-patient clinics, and three medical in-patient clinics. An email was sent to all RNs in the three groups encouraging clinic managers to allow all interested RNs to participate where possible for the sake of clinic operations. RNs from all eight clinics participated in the study. Individual interviews were conducted in an office in the department and focus-group interviews in staff rooms or conference rooms with no-one else present. Twenty of the RNs were interviewed twice in terms of both focus-group and individual interview or participated in two focus-group interviews.
The study was undertaken over a period of eight months from the beginning of April 2020 to November 2020.
The nursing staff were recruited from the following three groups of RNs:
RNs relocated from the laboratory or out-patient clinics to in-patient clinics. RNs continuing in in-patient clinics and receiving COVID-19 patients. RNs remaining in out-patient clinics or the laboratory who still had to provide nursing to the usual patients.
Interviews lasted 25–75 minutes. The five focus-group interviews included six, 10, five, five, and 10 RNs and lasted 45–95 minutes, all including both relocated and remaining RNs. The data collection focused on the RNs’ experiences right up to, during and after the number of COVID-19 patients significantly declined to obtain in-depth understanding of the meanings that RNs ascribed to the organizational changes within the department during the COVID-19 pandemic.25,26 All interviews were conducted with audio recordings using field notes.
Participants
Participating RNs were between 26 and 59 years old and had between six months and 28 years of professional experience (Table 1).
Included participants (n = 47).
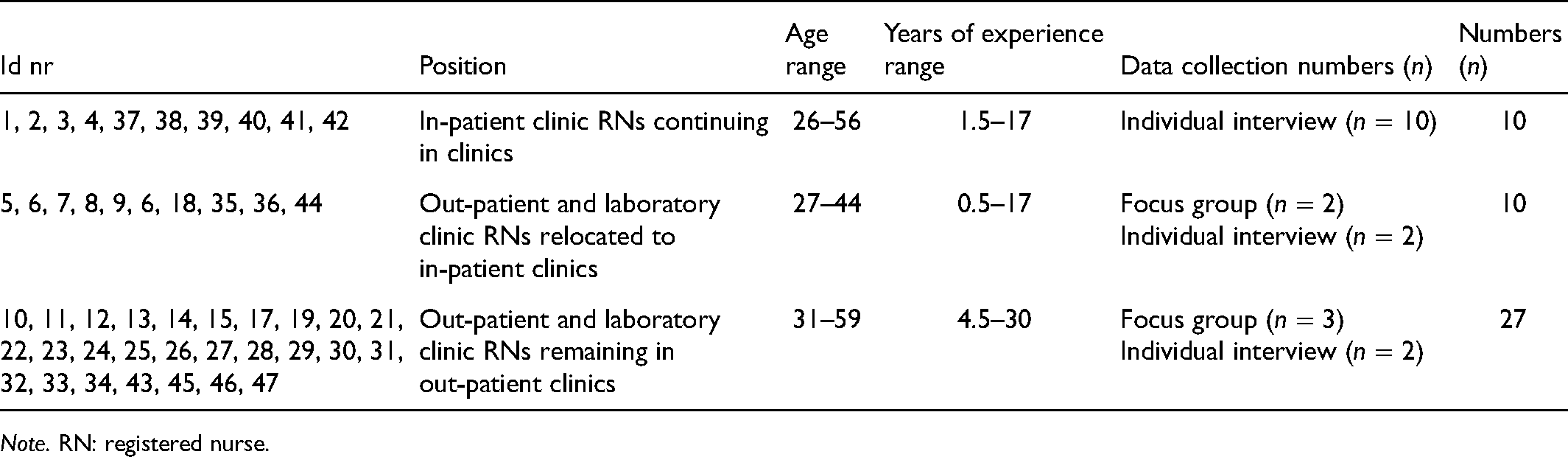
Note. RN: registered nurse.
Data analysis
The coding process explored underlying ideas, assumptions, conceptualizations, and interpretations of the RNs’ experiences in data. 25 Data from focus-group interviews and individual interviews were pooled for the three groups of participants and marked by colouring the transcriptions differently and numbering all participant statements to track overlapping or diverging experiences and meaning-making processes in the three groups of participants. Statements, sentences, or words in the initial open coding led to identification and labelling of minor and major themes. Clusters of themes were then labelled to capture meaning and significance in data. Finally, quotations were selected and translated to add richness to the themes. Throughout, coding, results, and conclusions drawn were discussed with participants. Data collection ended when no new significant codes were forthcoming.22,25
The present study has included a relatively large number of RNs who remained in out-patient clinics (n = 27) or were relocated from out-patient clinics to in-patient clinics (n = 10). Throughout the data collection, attention increasingly turned to exploring the anger and frustrations of those RNs relocated and those left behind in out-patient clinics. Other studies have drawn attention to frontline RNs, but the ambition in this study became, over time, to likewise give voice to the RNs who maintained the normal hospital department function and patient groups. For example, the production of early codes concerning the frustration, abandonment, and anxiety which several participants expressed. Notes and initial ideas were written down during all readings of the transcripts, where ideas were constructed describing what the data were about, meant, or represented. A pattern emerged that revealed diversity in experience between in-patient RNs, relocated RNs, and RNs remaining in out-patient clinics. The coding process remained open and inductive without any pre-set codes. Thus, all codes were developed and transformed throughout the data collection and coding process.
An example of the coding process is listed in Table 2, exploring the meaning the three groups of RNs attributed to their experiences during the organizational changes.
Coding of the meaning RNs attributed to their experiences during the organizational changes.

Note. RN: registered nurse.
Ethical considerations
Our presence, the topic, and the questions the RNs have been asked to answer have revealed some existential issues in many of the RNs. For some, the conversations have had a therapeutic effect on their frustrations. During the second interview, a nurse begins by saying to the interviewer: … it was really good to talk to you last time … to be allowed to sit down with you and be allowed to say everything I wanted to say … because I was so frustrated but it helped me a lot to be allowed to talk about it … (id 10)
The interviews have been carried out with respect for the participants’ experiences and actions. We have left out several of the more unguarded and strongly emotive comments for ethical reasons. 28 As the authors of this article with access to these comments we find them even more supportive of the conclusions we draw than the comments we have felt able to report.
Presentation of findings: sense-making in a changed reality of nursing
The overall theme of the findings was analysed as ‘Sense-making in a changed reality of nursing’, explaining the process of attributing meaning to the experiences of the organizational changes in RNs' working lives. The changes were positive or negative depending on location, work tasks, and degree of workload of the individual RNs. The effort to create sense-making emerged in terms of two sub-themes: ‘Creation of meaning or meaninglessness in nursing practice’, and ‘Identity-loss and identity-reinforcement processes in RNs’. The RNs did not experience a choice as to whether they would participate in the COVID-19 emergency response. The experience of powerlessness, amazement, and frustration when realizing they could be relocated at the whim of managers was an unpleasant surprise which created anger and distress. RNs continuing in in-patient clinics considered it mainly a privilege to be at the forefront caring for COVID-19 patients. Figure 1 illustrates the main theme and the two related sub-themes explaining the meaning or meaninglessness the RNs attributed to their experiences of the organizational changes leading to professional identity loss or identity reinforcement.
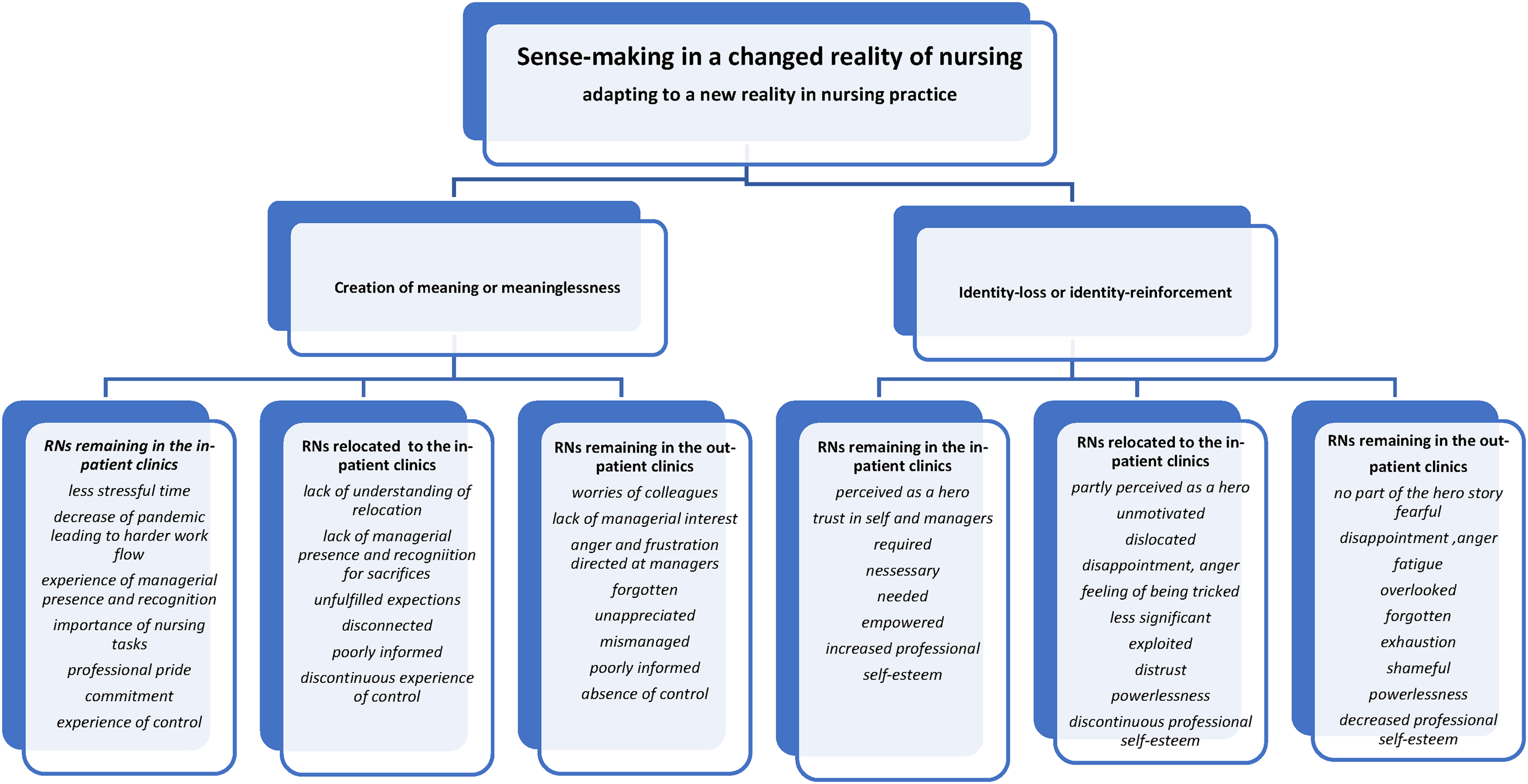
Sense-making in a changed reality of nursing.
Creation of meaning or meaninglessness
The extent to which the RNs experienced meaning or meaninglessness in the COVID-19 contingency in the clinics thus apparently depended on whether they had continued in in-patient clinics, were relocated, or remained in out-patient clinics. The RNs who had continued in in-patient clinics felt well informed and content in the management's handling of the emergency preparedness, and felt recognized, with excellent managerial attention and support.
Both relocated RNs and RNs who remained in out-patient clinics generally felt mismanaged and poorly informed and lacking managerial recognition of their willingness to adapt to major changes in everyday working life.
RNs remaining in in-patient clinics
To RNs who had their permanent employment in in-patient clinics, the corona pandemic became a break in a busy, time-constrained, and hard everyday life. Several RNs described an unusually hard time leading up to the pandemic: they went home from work exhausted due to a high occupancy rate and many patients had to lie in beds in the corridors due to lack of available patient rooms. The increasing number of COVID-19 patients in the department was followed by a decrease in the number of normal-intake patients admitted. At the same time, restrictions on exclusively single-patient rooms limited the normal-intake patient numbers further. There was thus an experience among the RNs that the work pressure eased, and they had time to adjust to the many new measures that the emergency necessitated. We have never had so much time before, so in many ways it was a break from an otherwise very busy workday. (id 3)
The experience of managerial recognition and of being meaningful and necessary was pervasive among the RNs who remained in familiar surroundings in in-patient clinics. After the first months, the number of COVID-19 patients decreased, and the intake of normal-intake patients increased again. This led to a harder workload, and beds were again full of the in-patient clinics' regular patients, who now had to lie two or three in the rooms as normal. At the same time, the RNs experienced that the many restrictions and new rules regarding protective equipment became an increasing burden in everyday life, which made workflows difficult and time consuming.
RNs relocated to in-patient clinics
For the RNs who had been relocated to in-patient clinics, it was a less meaningful time. Several had difficulty recognizing the reasons why they were relocated. Furthermore, they felt that managers did not recognize the sacrifice they themselves perceived they had made in having to adapt to night and weekend shifts, new patient categories, and an unknown working-space area. They felt little recognized and welcomed in the in-patient clinics. Likewise, they did not find the relocation meaningful, either personally or professionally, and the expectations around being transferred to frontline duty to care for severely ill COVID-19 patients were not met. Instead, relocated RNs were predominantly directed to care for stabilized, non-infected patients. The disappointment was not commensurate with the personal costs that many of them experienced. This took the form of suddenly having weekend and evening shifts again, as well as the worry that they would infect their families outside work. The relocated RNs felt no influence on whether they were selected for relocation or not, which created further frustration and powerlessness. The futility of the transfer could turn to anger and powerlessness after they were back in their familiar work environment in their out-patient clinic or the laboratory: … And after I got home I have become a little bit more angry, angry that they have dragged it so far … and I see no point in what we were there for … and it became clear quite quickly that we were not there for corona patients but for the staff as a ‘relief’ contingent. (id 7)
RNs remaining in out-patient clinics
The RNs remaining in out-patient clinics felt divorced from what happened in in-patient clinics and the management's calculations, which made them feel forgotten and unappreciated: … We have really all been ready to go into the battle but we have not been involved in anything. (id 11) We just knew that there was chaos out there. (id 24)
… not really nice for my colleagues to have a job you did not apply for yourself and at the same time continue to maintain positive … I thought that a contingency was when it was really urgent, but that was not the case at all. (id 10)
… we felt that every time our RNs were sent home sick from COVID-19 they just sent for ‘new fresh supplies’, for us who were left behind it looked like an unbelievable exploitation of our RNs … we didn't understand why they should remain out there. (id 12)
These RNs experienced a lack of managerial interest – of being forgotten and not appreciated – but, likewise, frustration and anger caused by the abnormally large amount of work pressure due to the absence of the relocated colleagues. The work pressure, and narrative of an unnecessary relocation and exploitation of relocated colleagues, became the catalyst for anger and frustration toward both the department and hospital management. There was a pervasive experience of being cheated and deceived which made the RNs consider their work effort as meaningless and unnecessary.
Identity-loss or identity-reinforcement processes in RNs
The ‘identity-loss’ or ‘identity-reinforcement’ processes differed across the three groups of RNs. Those continuing in in-patient clinics overall felt empowered during the pandemic, whereas RNs relocated or remaining in the clinics, to varying degrees, felt powerless. Stories of identity loss were found exclusively with RNs who had remained in out-patient clinics or with relocated RNs. Becoming dislocated from familiar surroundings and colleagues apparently created conditions for generating powerlessness, alienation, and loss of professional self-esteem.
RNs remaining in in-patient clinics
The RNs who continued in in-patient clinics had predominantly identity-reinforcement narratives: stories that were characterized by professional pride and a great professional commitment to being part of a focal point and, at the same time, being important and necessary to ensure the operation of the department. The experience of unreserved loyalty, support, and great recognition of their managers was strong in these RNs. At the same time, they felt involved and informed about decisions from the clinic management. But I have always had the feeling that the management was in control of it and it has given me a huge peace of mind … because then I could just focus on my nursing and what I had to do. (id 1) In the beginning of the pandemic it was very exciting … and because we had a corona section in the department, you could call yourself a corona nurse … That was really something special in the beginning … so it was wildly exciting and cool to be a part of … that you did your part in a chaotic situation where no-one really knew what they were dealing with … (id 13)
RNs relocated to in-patient clinics
Relocated RNs experienced a fearful time up to the final decision of which RNs were chosen from the out-patient clinics, and felt under huge pressure to accept the relocation. A nurse from an out-patient clinic described her feelings a week before she was relocated to an in-patient clinic: I can clearly remember the night when I realized how serious the situation was becoming. I realized how we were in the beginning of or entering a war and I started crying. We as RNs had to take the lead in a war where we did not really know the enemy. I was worried about myself and I was worried about my child as I am alone with him … what do I do if I get sick or my child gets sick? What do I do with my child if I have to go to work night and day and there is no one to look after him? (id 18)
The relocated RNs were disappointed due to the hectic introduction to in-patient clinics and did not feel welcomed. At the same time, several of them pointed out that, over time, they came to doubt the necessity of their contribution in in-patient clinics. They pointed out reasons such as ‘off duty’ and termination of leave regarding the permanent nursing staff, as well as the decrease in patient numbers as grounds for their doubts. In continuation with the RNs' experiences of not being necessary to the COVID-19 operation, their frustrations and feeling of having been tricked into an in-patient clinic increased.
The lack of managerial credit perceived by these RNs may have been co-creative of the emerging narrative of the RNs' interpretations of being considered less significant, and of being exploited. What initially encouraged the relocated RNs, and made the experience bearable, was the opportunity to become part of the hero story. However, since some of them did not have the necessary competencies or feared being infected, they were instead used to care for ordinary medical in-patients rather than being posted to the front line. As a result, a mismatch arose between expectations and their assigned realities, resulting in identity loss. This was instrumental in the creation of a completely different story of which they unwittingly became a part.
RNs remaining in out-patient clinics
For the RNs in out-patient clinics, the first few weeks were full of fear or anticipation. As the weeks went by, fear and anticipation were replaced by anger, disappointment, or fatigue caused by the oppressive work situation. Those RNs remaining in out-patient clinics felt forgotten, with many narratives concerning information being hidden from them; feelings which were reinforced as several relocated colleagues became COVID-19 infected without them being notified. The work pressure in out-patient clinics, the concern for relocated colleagues, and the experience of lack of managerial care were pervasive and stronger than in their relocated colleagues. It was an ugly time … You were just a small piece in a puzzle that managers can move around as they like. RNs were sent out and everything was redone, and we were busy out here and we did not know what was happening, and I experienced that RNs have no say whatsoever. (id 35) Instruction was redone depending on what kind of protection equipment managers could collect. It had nothing to do with our protection and safety. I had a few weeks where I considered whether I should be a nurse at all anymore. I thought to myself this is enough! I do not bother anymore. (id 11) I feel a little bit ashamed, not volunteering to participate working in the in-patient clinics, but just the thought gives me a feeling of a cold stone in my stomach. (id 23)
I can't do it and I won't do it but I guess I have to if they force me to. (id 28)
… so complaining, feeling tired-out is difficult to us left behind with all the work. (id 27)
The destructive experience was apparently reinforced by a sense of discomfort or shame over the relocated colleagues who were posted to what they thought of as an even worse alternative to remaining in their own out-patient clinic.
Deviant cases
Some cases differed from the patterns that the analysis generated. A small number of the relocated RNs shared, to a lesser degree, the same concerns, frustrations, and anxieties over being relocated as their colleagues but were less exhausted. An explanation for this deviance may be the fact that these RNs had recent experience in intensive care and were familiar with the staff and surroundings in in-patient clinics.
Discussion
The findings have pointed to variation in the RNs' attribution of meaning or meaninglessness to their experiences, and the extent to which the organizational changes generated identity reinforcement or, conversely, identity loss.
The findings in this study suggest that the meaning the RNs attributed to the organizational changes became co-creating to the experiences of identity loss or identity reinforcement in the RNs. The connection between meaning-making and identity has been explored by Weick, suggesting that there is a connection between how we perceive ourselves and how we perceive and create meaning in the world around us, and that this meaning-making has an effect on how we perceive ourselves. 29 In accordance with the findings in this study, the creation of narratives – being a hero, being tricked or left behind – seems to attribute meaning to the organizational changes causing experiences of identity loss or identity reinforcement in the RNs.
Numerous studies point to several consequences for RNs working on the front line during the pandemic, including depression, insomnia, burnout, nervousness, and anxiety,10,30,31 which cannot be found here regarding RNs on the front line continuing as usual in in-patient clinics. In contrast, this study finds that RNs were able to attribute meaning to changes they experienced, considering the pandemic to be an easier time in terms of workload and stress, even though new restrictions and regulations were time consuming and tiring over time. The divergence may be explained by the fact that several earlier studies reported that RNs experienced a high work pressure, poor involvement in the work and organizational changes, and lack of information from their managers.30,32 Even though RNs in this study may have felt less overworked, the involvement and trust in managers seems to have had an impact on the meaning the nurses attributed to their experiences of the organizational changes.
The RNs relocated from or remaining in out-patient clinics generally experienced meaninglessness and identity loss, perceiving themselves as discredited and, to some degree, victims being cheated, poorly informed, forgotten, or abused. Studies suggest that the unknown and unpredictable character of the COVID-19 pandemic may increase anxiety and frustration in RNs, 8 while other studies, exploring RNs' behaviours during previous epidemics, find that, while some RNs are willing to accept the personal risks during a pandemic situation, other RNs perceive the personal risks as too high, leading them to resign their position. 30 As with many RNs, managers may have experienced an unpredictable and chaotic time, putting their values and beliefs under pressure. 33 It may be that managers have kept their attention on RNs on the front line, paying less attention to the nurses behind the front line.
The hero narratives of the frontline RNs may have supported their sense of meaning and identity reinforcement, while being kept out of the narrative may have provided meaninglessness and identity loss in other nurses. Unintended consequences from perceiving RNs as heroes may lead to negative outcome in recruitment, narrowing the diversity of RNs since not all do, or should, care for intensive patients. Furthermore, the interpretation of RNs as overcoming danger and adapting to hard workload conditions may unconsciously, over time, lead to less political and managerial attention being paid to the nursing environment and well-being of RNs.15,17,19,20 Ultimately, the RNs in in-patient clinics became a part of the hero story, while, simultaneously, another story was created about relocated RNs being fooled and exploited, lacking managerial support, and left with unfulfilled expectations.
Every manager is a storyteller and their choice of words matters, stressing the importance of carefully chosen words describing the world within. Managers’ descriptions of reality can become reality. 34 This study shows that nurses too are storytellers, creating their private narratives as a means of making sense of whatever reality they find themselves within. Attending to narratives of meaning or meaninglessness in nurses during organizational changes could be instrumental to managing the anger, frustration, and hopelessness arising from experiences of meaninglessness.
Finally, future studies should further explore and discuss an avoidance of stigmatization of RNs who do not want to participate, or feel incapable of participating, in the response to a pandemic. Becoming excluded from the narrative of good nursing practice may have consequences not only for affected RNs but also for the future recruitment and retention of RNs.20,35
Methodological considerations
The pragmatic sample method used is in line with the descriptive phenomenology method for qualitative nursing research. 22 In terms of transferability, the findings in this study support those of a growing number of studies9,10,14,17 describing the consequences of COVID-19 for RNs, as well as adding new knowledge of the nurses left behind continuing their usual nursing tasks. Furthermore, the findings have relevance to any rapidly implemented organizational change in healthcare systems pointing to possible counterreactions in RNs.
In terms of trustworthiness of the data collection, the first author maintained an awareness of letting the RNs guide the interviews and supported any emotions or statements with curiosity and an openness to the variety of sometimes conflicting responses from RNs and across data. The authors’ in-house knowledge of the working conditions of the RNs provided the possibility to saturate the data. During the day-to-day contact with the RNs, the findings were overwhelmingly confirmed using participant verification of the emerging findings. Any new perspectives revealed were used in the focus-group interviews to add richness to the findings.
In the process of analysis, the authors coded separately with the purpose of revealing any differences in the interpretation process.
The advantages and disadvantages of examining one's own practice are well known.28,36 In this specific case, in a study of responses to managerial change where the second author is the manager of all the participants, the risk of this affecting responses was mitigated by having only the first author conduct interviews and then anonymizing data.
Conclusion
The findings have pointed to a divergence in the meaning or meaninglessness that the RNs attributed to their experiences, and the extent to which the organizational changes generated identity reinforcement or identity loss. The findings suggest that managers, attending to narratives of meaning or meaninglessness in nurses during organizational changes, could be instrumental to managing the anger, frustration, and hopelessness arising from experiences of meaninglessness.
Relevance to clinical practice
Globally, we are probably facing several future waves in the current COVID-19 pandemic (not to mention other potential pandemics) that will necessitate restructuring in many ways, including transferal of RNs to other clinics, departments, or hospitals. These changes are likely to continue to have major consequences for many RNs, both professionally and personally.
The data in this study are exclusively based on one medical department in Denmark. Nevertheless, the ambition is that the findings may inspire RNs and managers in a broader Scandinavian context to explore their organizations, revealing the possible consequences that the COVID-19 pandemic may have had for RNs and managers.
This study shows that, although other studies have indeed demonstrated the risks to those on the front line, those left behind, continuing business as normal, must also be recognized: a failure to do so, worshipping only the heroes in the midst of battle, could have serious and long-term consequences for hospitals and the entire health system if RNs, experiencing meaninglessness through future major organizational changes, simply walk away.
Footnotes
Acknowledgements
All included nurses have spent a significant amount of their energy and time participating in the project: they made a significant contribution to the study through discussions of their thoughts and experiences, as well as in discussions of the findings. A special thanks to PhD student Maja Pedersen who conducted the first seven interviews, and Professor Mark Grimshaw-Aagaard for academic discussions and the final proofreading.
Author contributions
Data collection was by the first author. Both authors participated in design, coding, and writing the final paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.