
Abstract
Various support interventions, such as nurse case managers (NCMs), have emerged in response to increasing inequality in health and the growing population with multi-morbidity. NCMs collaborate with a wide range of professionals across social and healthcare services. This study explored social and healthcare workers’ perspectives on collaborating with hospital-based NCMs. A total of 16 social and healthcare workers were interviewed. A thematic analysis led to three themes that describe the NCMs as follows: 1) being crucial allies who gather the threads; 2) breaking free of standardised care to create flexible support solutions; and 3) making a difference to individuals who are in vulnerable positions. Highly effective and specialised societal systems have created a need for services such as the NCMs, who will act as crucial allies to both collaboration partners and patients. Based on the accounts of our participants, NCMs contributed with something more to the cross-sectorial collaboration, than what they had experienced in previous collaborative partnerships. This study underlines the need for structural changes if we are to address the sustained issues of health inequalities.
Background
These days, many western society healthcare services are advancing in areas such as effectivity and specialty treatments. While this may be beneficial to many in the general population, there are numerous reports of increased inequality in health and illness among groups of people experiencing multi-morbidity along with severe psychosocial difficulties in everyday life.1,2 Multi-morbidity is characterised as the coexistence of two or more chronic conditions, where each must be a non-communicable disease, a mental health disorder or an infectious disease of long duration.3,4 Besides the substantial condition and treatment burden, people with multi-morbidity face higher safety risks due to complex illness and treatment management regimens, more frequent and more complex interactions with healthcare services, greater need for coordination, higher demands for self-management and risks related to polypharmacy. 5 In addition, these people are also considered more vulnerable to safety issues due to a poor general health state.4,5 Even though multi-morbidity has been of concern in political and healthcare arenas for years, research into the management of the growing number of people with multi-morbidity is limited. 5 Some suggest that an integrated treatment approach is needed, rather than specialist treatment focused on single illnesses. 6 However, there is limited evidence to support any specific intervention.5,7
In recent years, various clinical-based support interventions have been developed in response to the inequality in health and the growing population with multi-morbidity. In Denmark, such interventions include nurse case managers, 8 transitional care nurses9,10 and social nurses.11,12 These initiatives all, in some way, deal with the management of patients who transition between care settings. Transitions of care, 13 understood as the process of a patient transitioning from one organisational context to another, can be difficult to manage for both patients and healthcare professionals. Important threats to safe patient transitions have been identified as related to poor quality of instructions provided in handovers, discharge of patients before arrangement of care at home are in place, challenges related to medication (e.g. availability) and unreasonable workload in handover from the hospital setting to the community setting. 14 It is reasonable to think that the complexities embedded in managing multi-morbidity will only worsen in such transitions of care.
This study focused on the context of nurse case managers (NCMs) employed at a university hospital in the North Denmark Region. The NCMs were all registered nurses employed in the emergency departments at three geographical locations of the university hospital, and as part of their work they assisted patients by coordinating complex pathways during their healthcare trajectory. 8 The NCMs collaborated extensively with a wide range of healthcare professionals at the hospital, with municipal social and healthcare services including those responsible for addiction treatment, temporary housing and street level outreach teams. A key element of NCM work was their ability to collaborate with all these various internal and external actors – building bridges to all stakeholders in the patient's transition of care. NCMs themselves have described how their ability to make a difference in the patients’ lives depend on these collaborative relations. 8 However, knowledge about the perspectives of the collaboration partners is lacking. Hence, the aim of the study was to explore social and healthcare workers’ perspectives on collaborating with hospital-based nurse case managers.
Methods
Design
This study was a qualitative interview study and drew on the theoretical perspective of social constructionism. 15 Within this perspective, our knowledge about the world, and what we perceive as reality, is considered as continuously produced and shaped through our participation in social interactions. To rephrase it, we as researchers took part in the social constructions of different versions of reality in the interviews with the informants. Thereby our knowledge and understanding of the reality is forever changeable and continuous. 15
Study context
The study was conducted in the North Denmark Region and explores the perspectives of social and healthcare workers, who at the time collaborated with hospital-based NCMs on cases involving people in complex healthcare trajectories. These patients often experienced multi-morbidity and social issues and their trajectories were typically characterised by multiple contacts to social and healthcare settings across sectors. 8 These issues affected the patients’ ability to navigate the usual care and support trajectories and manage everyday life in general. Hence, the study context included a heterogeneous collaboration sphere, which involved employees from public regional and municipal settings as well as housing facilities based in the private sector, such as care homes.
The research group responsible for this study consisted of experienced qualitative researchers who were employed at two Danish university hospitals (MGK, CB and BL) and two university students during their last year of studying sociology (SAG and MLRR).
Participants and recruitment
Eligible participants were social and healthcare workers, who had collaborated with the NCMs. At the time of the study, six NCMs were employed at the university hospital. To identify eligible participants, three of the six NCMs were approached and asked to act as gatekeepers enabling our access to potential participants. The three NCMs who were approached were the most experienced in working in an NCM function. These three NCMs were asked to each make a list consisting of 5–10 collaboration partners that they found to be essential in their daily work. In some cases, the NCMs mentioned a general hospital ward or healthcare service as a collaboration partner; in these cases, the secretary of each place facilitated contact to an employee who had collaborated with the NCMs.
The identified eligible participants received an invitation to participate and written information about the study via email. In some cases, the preliminary contact was via telephone. As a result of this purposeful sampling, 16 16 social-care and healthcare professionals agreed to participate in the study. Eight were employed in the public regional services, seven were employed in public municipal services and one was employed in the private sector. Furthermore, both somatic and psychiatric hospital departments were represented in the group of participants. As such, there was great heterogeneity in the composition of the participant group, which included registered nurses (n = 8), social-care and healthcare assistants (n = 2), chief physicians (n = 2), and social workers (n = 4). All but one of the participants were women (age range = 28–64 years; mean age = 48 years).
Individual interviews and data generation
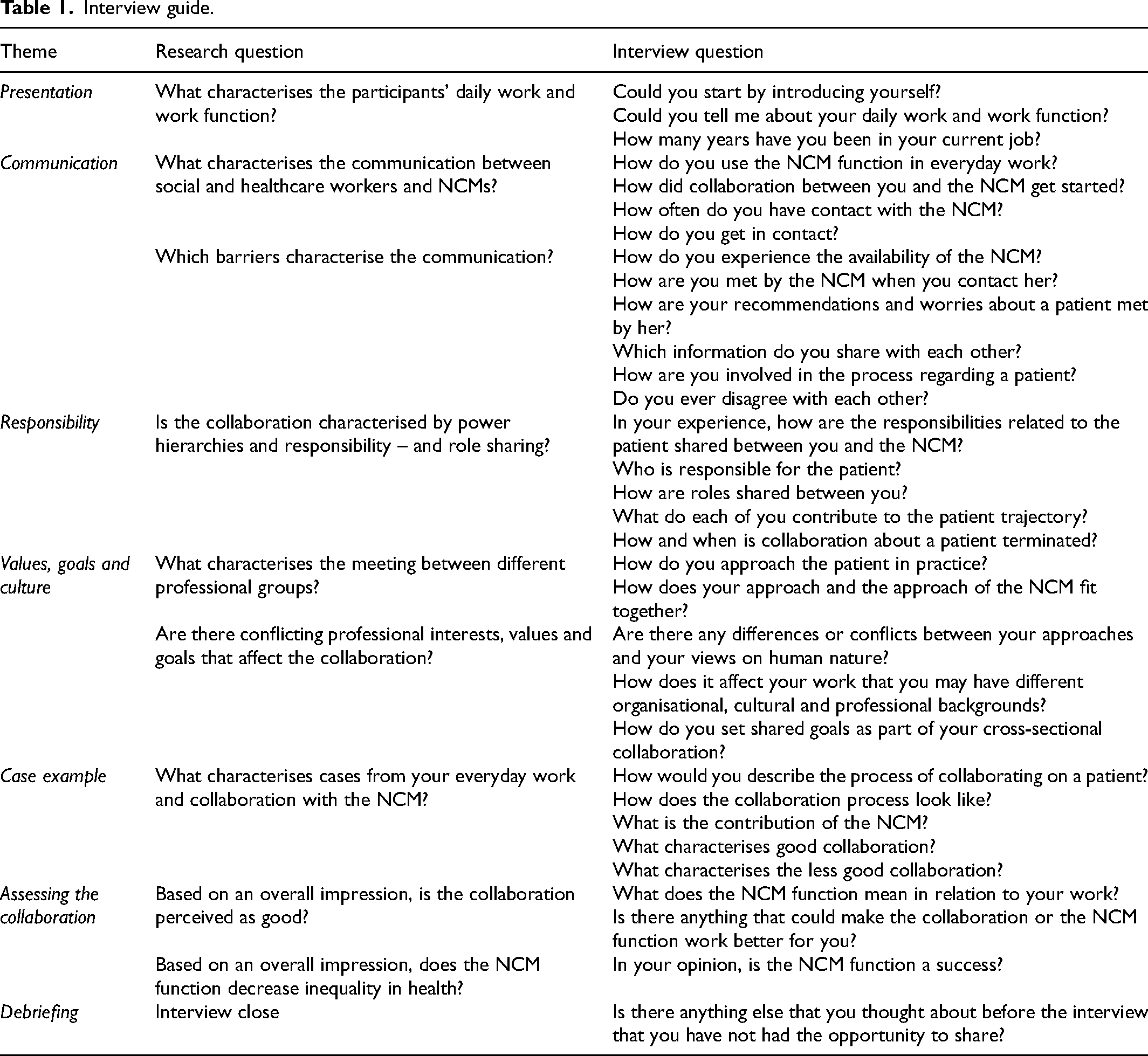
The participants were interviewed using a semi-structured interview guide 17 (see Table 1). The guide was based on themes derived from literature on topics such as distribution of responsibility and roles, professional values and culture, aims for patients, inequality in health and disease, and general knowledge of communication in interdisciplinary collaborations.18–20 The interview guide was developed by the first, second and last authors (SAG, MLRR and BL).
Interview guide.
The interviews were conducted by the first and second authors (SAG and MLRR) during October 2022 and held at a location of the participant's preference, e.g. at the participants’ workplaces or at conference rooms at the university hospital. The interviews varied in length, lasting 26–97 min (mean = 63 min).
In total, 15 interviews were conducted; 14 were individual interviews and one was performed as a joint interview with two participants, based on their wishes. The interviews were audio-recorded and transcribed verbatim.
Data analysis
Data were analysed using a thematic analysis as described by Braun and Clarke.21 The six steps of thematic analysis move from initial familiarisation with data, open coding and identifying themes to a more structured and densified analysis consisting of broader themes. 21 In this analysis, the social constructionist perspective provided a frame for exploring patterns of meaning embedded in participants’ accounts about how they experienced collaborating with NCMs in their everyday practices. 15
The first and second authors (SAG and MLRR) approached the analysis by reading the transcripts and making initial codes separately. The first, second and last authors (SAG, MLRR and BL) discussed the codes and initial themes and reached an overall structure of the final themes. 21 The themes shed light on the social and healthcare workers’ perspectives on collaborating with NCMs and built on patterns found across the data. Finalising the analysis included writing up the themes and providing illustrative quotes from the participants to strengthen the presentation of our findings.
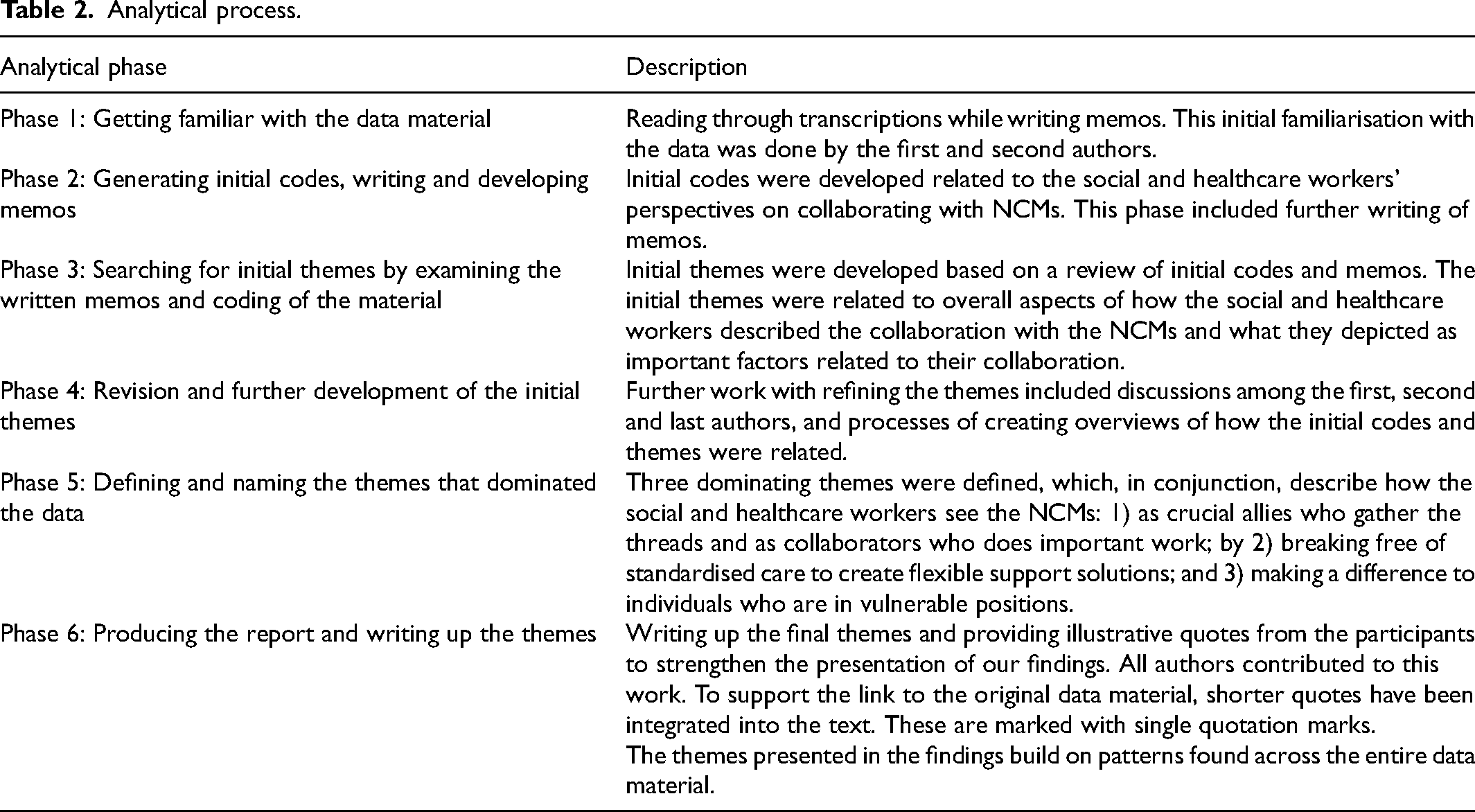
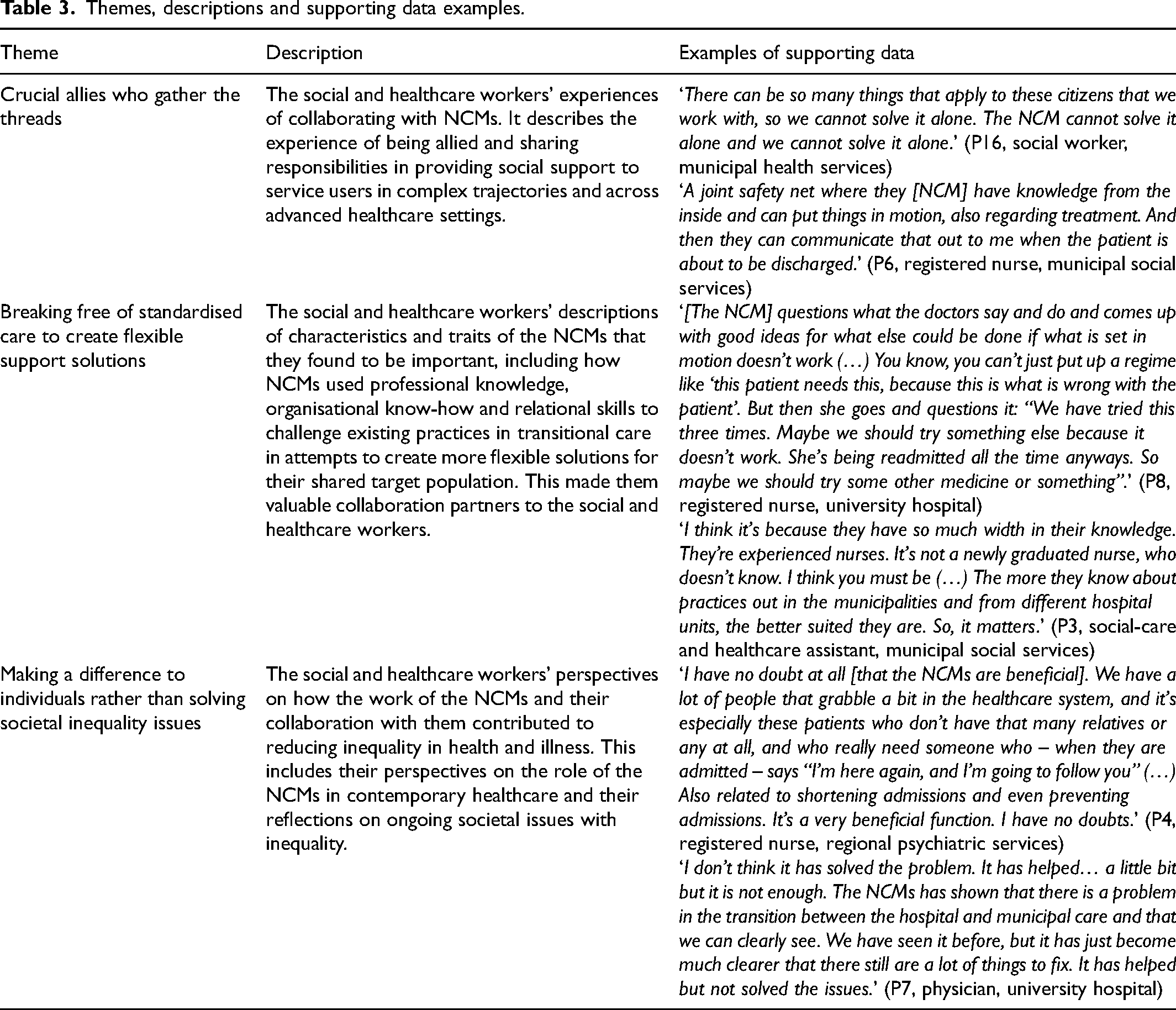
Table 2 provides description of the process of analysis. Table 3 illustrates the three themes and supporting data examples.
Analytical process.
Themes, descriptions and supporting data examples.
Ethics
The social and healthcare workers received written and oral information about the study before giving written consent to participate. The study was carried out in accordance with existing rules for storage and management of research data and was reported to the regional research administration (ID F2022-118).
Findings
The analysis led to the following three themes that describe how the social and healthcare workers saw the NCMs: 1) as being crucial allies who gather the threads and as collaborators who do important work; by 2) breaking free of standardised care to create flexible support solutions; and 3) making a difference to individuals who are in vulnerable positions.
Being crucial allies who gather the threads
According to the social and healthcare workers, a fundamental part of their collaboration with the NCMs was focused on providing support to people with extensive psychosocial support needs who were in vulnerable positions and complex situations. They described the NCMs as ‘crucial allies’ in preventing these patients from ‘falling between two chairs’. Furthermore, they described how they and the NCMs shared a sense of obligation to step in and provide support to these patients, who were described as people who other healthcare professionals had ‘given up on’. Due to the complex nature of the patients’ transitions across social-care and healthcare systems, sharing responsibility related to providing adequate support was described as an important part of the collaboration. One said: ‘There can be so many issues in play with the citizens who we work with, and so we can’t solve them alone. The NCM can’t solve them alone and we can’t solve them alone.’ (P16, social worker, municipal health services)
In this way, they emphasised how they and the NCMs needed each other to succeed in creating sufficient social support and healthcare trajectories to the shared patients. Being allies reflected this shared responsibility and a commitment to their collaboration. As part of the collaboration, they and the NCMs came to share responsibilities related to providing support to the patient, while also covering each of their respective elements of the cross-sectoral patient trajectory. As an example, the social and healthcare workers highlighted how the NCMs, due to their organisational placement at the hospital emergency departments, were able to access important knowledge about each patient's physical, mental and social state and set supportive measures in motion while the patient was admitted at the hospital. Such measures could be related to cleaning the patient's home before discharge if necessary or making sure that sufficient support from municipal services would be provided in the home. One characterised their collaboration as: ‘A joint safety net where they [NCM] have knowledge from the inside and can put things in motion, also regarding treatment. And then they can communicate that out to me when the patient is about to be discharged.’ (P6, registered nurse, municipal social services)
In the social and healthcare workers’ experience, NCMs being based in the hospital setting could improve the chances of achieving a successful cross-sectional transition. When describing the role of the NCMs in their collaboration, social and healthcare workers portraited the NCMs as ‘an entrance door into the hospital system’, ‘someone who gathers the threads’ and ‘coordinate the patient's care trajectory’. These were collaborative aspects that contributed to continuity in the patient trajectory. In other words, the NCMs were described as establishing connections and strengthening the cross-sectional collaboration.
The social and healthcare workers also described how the NCMs became a kind of ‘security in an insecure system’, ‘a familiar face’ in a system where the patient was ‘thrown around’ in different settings and was in contact with a lot of different personnel. One explained: ‘The sooner they [the patients] meet some familiar faces, someone they can learn to trust and someone who can help them, the greater the chance that we can do something good for them.’ (P13, registered nurse, university hospital)
According to the social and healthcare workers, it improved the patients’ experiences with and attitude towards the general healthcare system when they met a familiar face in the form of the NCM. The social and healthcare workers also valued how this close relationship between the NCM and the patient created greater trust. Some social and healthcare workers had witnessed how the NCM became a confidential authority, which was equal to the doctors who were responsible for the treatment. The NCM became someone to whom the patients could confide in, and this was crucial for the treatment they would otherwise often disengage from. This was valued by the social and healthcare workers because they believed that it could relieve the patients from unnecessary stress and strain.
Breaking free of standardised care to create flexible support solutions
According to the social and healthcare workers, the NCMs were valued collaboration partners who used professional knowledge, organisational know-how and relational skills in attempts to create more flexible solutions for the shared patients.
The social and healthcare workers described how the NCMs’ everyday practices continuously challenged the traditional ways of managing the complex situations of the patients they interacted with. This approach was contingent on the NCMs’ willingness to take part in decision-making regarding planning of care trajectories. One described: ‘[The NCM] questions what the doctors say and do and comes up with good ideas for what else could be done if what is set in motion doesn’t work (…) You know, you can’t just put up a regime like “this patient needs this, because this is what is wrong with the patient”. But then she goes and questions it: “We have tried this three times. Maybe we should try something else because it doesn’t work. She's being readmitted all the time anyways. So maybe we should try some other medicine or something”.’ (P8, registered nurse, university hospital)
According to the social and healthcare workers, this way of challenging traditional thinking involved a way of ‘thinking outside the box’ and ‘breaking free from the standardised care packages’ to figure out what would be the best care option for each individual patient. The participants expressed different ways in which the patient's care trajectory improved when they collaborated with the NCMs. First, they believed that the collaboration created a better experience for the patient as everyone involved contributed with expertise from within their specialty. They described the value of having found a common ground with the NCMs in this fundamental approach to patient treatment and individual patient goals. In the eyes of the social and healthcare workers, the NCMs were ambassadors for planning suitable care trajectories for the patients that was based on individualised thinking and the NCMs’ ability to follow up on each individual person and their situation during and after discharge from the hospital.
The NCMs were described as experienced nurses with broad professional knowledge about the relatedness of medical and psychosocial aspects of life. Furthermore, NCMs were described as familiar with a variety of cross-sectoral settings, covering both the social support system and the healthcare system. One participant said: ‘I think it's because they have so much width in their knowledge. They’re experienced nurses. It's not a newly graduated nurse, who doesn’t know. I think you must be (…) The more they know about practices out in the municipalities and from different hospital units, the better suited they are. So, it matters.’ (P3, social-care and healthcare assistant, municipal social services)
Besides professional knowledge and organisational know-how, the social and healthcare workers highlighted certain personality traits that they believed were essential for NCMs. These included ‘being sturdy’, ‘not giving up that easily’ and ‘not taking ‘no’ for an answer’ if they believed something was in the best interests of the patient. In addition, the NCMs were described as ‘considerate of others’ and as ‘having an eye’ for the shared patients. One said: ‘I also think that the reason you apply for a job as a nurse case manager is because you want to contribute to make a difference and you care for this patient group. You would never do it if you were a little bit afraid of people with substance use or mental illness.’ (P16, social worker, municipal health services)
These personality traits implied a certain set of inherent values that cannot be learned or taught, and which contributed to the NCMs’ special way of viewing their patients. This meant that NCMs were able to look beyond the patients’ individual physical health issues and take other social and psychological aspects of the individual situation into consideration to create sustainable and durable care plans for each person. One said: ‘I can’t say that they have more time because they are very busy. But they take their time to dig a little deeper and maybe go further back in the patient record and discuss this with the nurse in the hospital unit.’ (P3, social- and healthcare assistant, municipal social services)
Most of the participants described sharing the values and approaches in taking care of the patients with the NCMs. However, in some cases, they expressed lacking the ability to cope with the patients who faced heavy use of substances and severe difficulties with engaging with healthcare or social services. In these situations, the social and healthcare workers were grateful of NCMs taking charge.
In general, the social and healthcare workers appreciated the collaboration with the NCMs as it relieved them in their daily work. One said: ‘I definitely think that it lightens my workload because there are some things they will take care of that either would have been a larger task for a doctor or something you would not have gotten done. So, it has filled a gap, I think. And I rarely think it is, you know, extra work (…) We can usually see the point with it. That it is good for the patient (…) It is usually a huge help.’ (P12, physician, university hospital)
Making a difference to individuals rather than solving societal inequality issues
This theme describes the social and healthcare workers’ perspectives on how the work of the NCMs and their collaboration with them contributed to reducing inequality in health and illness. This includes their perspectives on the role of the NCMs in contemporary healthcare and their reflections on ongoing societal issues with inequality.
When asked about whether the NCMs contributed to reducing the societal inequality in health and illness, the social and healthcare workers expressed certainty in that the NCMs made a difference in reducing the inequality of health and illness while others were more ambivalent. One said: ‘I have no doubt at all [that the NCMs are beneficial]. We have a lot of people that grabble a bit in the healthcare system, and it's especially these patients who doesn’t have that many relatives or any at all, and who really needs someone who - when they are admitted - says “I’m here again, and I’m going to follow you” (…) Also related to shortening admissions and even preventing admissions. It's a very beneficial function. I have no doubts.’ (P4, registered nurse, regional psychiatric services)
Even though most of the social and healthcare workers agreed that the NCMs made a difference for the individual treated patients, some called attention to a more fundamental problem in society that is not yet solved: ‘Hopefully it can help someone to a better life, but we don’t solve those huge societal issues. And I think that even if we hired 25 NCMs in this hospital department, we don’t solve a societal problem (…) Society as a whole has to be geared to this function and there have to be more resources allocated and that, I think, is really to hit the nail on the head because there is so many challenged people… both regarding diagnosis and substance abuse and loneliness and all kinds of things, so it is a huge, huge, huge societal task.’ (P13, registered nurse, university hospital) ‘I don’t think it has solved the problem. It has helped… a little bit but it is not enough. The NCMs have shown that there is a problem in the transition between the hospital and municipal care and that we can clearly see. We have seen it before, but it has just become much clearer that there still are a lot of things to fix. It has helped but not solved the issues.’ (P7, physician, university hospital)
The social and healthcare workers found that even though the NCMs did not solve the issues on a higher societal level, the establishment of the function made it clear that there is a serious societal problem that needs to be addressed. This societal challenge also made them aware of how dependent they were of the NCMs and their competencies in helping patients in the most complex cases.
A problem that prevailed related to collaboration with the NCMs was the fragility surrounding the function. To the social and healthcare workers, this fragility was linked to NCMs’ availability as the number of employed NCMs did not always match the number of patients who could benefit from their help: ‘Well, if this patient is to get some proper help with these problems that he has, well he is dependent on whether there is an available NCM who can join the case. But they don’t always have the time. It depends on how many active cases they have at that current time.’ (P6, registered nurse, municipal social services) ‘She was about to go on her summer break and that is the way it is, it is vulnerable when there is only one [NCM]… There is no one to take over but that is “the game” and that is also how it is in a lot of other workplaces.’ (P14, registered nurse, municipal health service)
It created vulnerable situations when the NCMs were unavailable because of holidays and weekends. This was described as problematic since the patients’ life situations and problems could not be expected to follow the work plans of the NCMs. The participants described how collaborating with NCMs could potentially decrease the number of days these individuals were admitted to hospital, and make sure that they were given the best possible support after discharge. However, when the NCMs were not available, it created situations where the social and healthcare workers themselves had to adapt to help patients in need. They described how they would then seek help in other places, to try to keep the patient in the hospital or extend the current treatment until the NCMs returned.
Discussion
This study explored social and healthcare workers’ experiences of collaborating with hospital-based NCMs. The findings include their descriptions of NCM as crucial allies, who they valued as collaboration partners in providing support to patients with extensive psychosocial needs, due to their ability to persistently challenge the traditional ways of thinking treatment and care trajectories. By exploring the perspectives of some of the NCMs’ collaboration partners across social-care and healthcare settings, this study provides additional insight into the NCMs’ capabilities into collaborative practices.
Support interventions such as the NCMs have been developed and implemented across healthcare settings as a response to changing population demographics and increased inequality in health.22–24 Our current social and healthcare systems are often described as highly specialised and fragmented in nature and as causing patients with multimorbidity and extensive psychosocial needs to have multiple contacts during their trajectories. 25 Owing to this, it may seem paradoxical that the solution should be to introduce yet another type of healthcare professional with whom these patients need to engage. Even though the social and healthcare workers in our study did not perceive the work of the NCMs as decreasing social inequality in health at a societal level, they did describe how the NCMs’ particular way of approaching patients with extensive psychosocial support needs paved the way for making a difference in that individual's life. Previous research has described how a key element of NCMs work practices was their ability to build collaborations with all potential stakeholders in the transition of care for patients with extensive psychosocial needs across advanced healthcare settings. NCMs themselves have described how their ability to make a difference in the patients’ lives depend on these collaborative relations. 8
The social and healthcare workers characterised the NCMs as crucial allies and as collaboration partners to share responsibilities with when providing social support to patients with extensive psychosocial support needs. The social and healthcare workers’ description of their collaboration with the NCMs depicted a collaborative practice that entailed sharing knowledge across settings and professional disciplines. This echoes what is at the very core of interdisciplinary and cross-sectional collaboration and how such collaboration may benefit patients, who then have a greater chance of receiving multidisciplinary attention. 26 Even though such collaborative practices could be expected to be part of a cross-sectorial collaboration in general, the social and healthcare workers highlighting this as special and as characteristic of their collaboration with the NCMs may indicate how this was not the general experience when collaborating with other healthcare professionals. Previous research into the NCM function mirrors these differences and describes how hospital-based NCMs were found to be providing something other than normal hospital nursing care. 8
In this study, the social and healthcare workers’ descriptions of the collaboration with the NCMs illustrated how they in some ways had succeeded with building collaborations that entailed the sharing of patient-related information, mutual respect and a shared understanding of how none of them would be able to provide sufficient support alone. Knowledge sharing, mutual respect and a shared understanding of responsibilities are factors known as the essential elements of interdisciplinary and cross-sectional collaboration, and has previously been described as difficult to achieve. 26 Inherent in this, are the main aspects of interdisciplinary collaboration, such as different work cultures coming together, a high level of interaction, mutual authority and sharing resources. 27 The knowledge gained through our findings about social and healthcare workers from different cultures can be used to understand how they succeeded in creating an environment based on trusting collaborations between professionals working with transitional care across specialties and sectoral borders.
Once again, it could be argued that the collaborative practices described in this study should take place as part of ordinary nursing care in relation to any interdisciplinary or cross-sectorial patient trajectory. However, continued focus on increasing specialisation and effectivity across contemporary social-care and healthcare systems facilitates an increased fragmentation of care. 28 Furthermore, as part of this development, it seems that key values and competencies of nursing, such as building relationships with patients and attending to psychosocial needs, have been put under pressure by an increased focus on providing task-oriented care and treatment.8,29,30
Collaboration is pivotal to adequate address the needs of the group of patients with complex issues in relation to health and social life. 8 However, this may be difficult to achieve in a healthcare system characterised by efficiency and specialisation, goal-based activities, accelerated care and treatment trajectories that is based on specific medical diagnosis. 22 Establishing and maintaining interdisciplinary and cross-sectorial collaboration has been described as contingent on social relations with one's collaboration partners.31–33 Relational coordination as described by Gittell32,33 and Bolton30 becomes possible through frequent communication of high quality, which is supported by relationships. Building collaboration based on shared goals, shared knowledge and mutual respect enables the involved parties to achieve better outcomes. 31 In our study, building collaboration across social-care and healthcare sectors was depicted as relying on mutual trust and knowledge about the collaboration partner. The social and healthcare workers described their collaboration with the NCMs as building on a shared understanding of both parties needing each other to be able to provide adequate support to their shared target population. Building relational collaborative practices is complex and involves multiple stakeholders at different organisational levels and should not be considered an easy task. 34 Across the interviews, the social and healthcare workers described the knowing each other as an important factor in the collaboration with the NCMs. Even so, it was beyond the scope of this study to provide in-depth exploration of the meaning of relationships within this collaboration. However, building on the work of Gittell and others30,32,33, future studies should focus on exploring the relational aspects of this collaboration. The social and healthcare workers who participated in our study worked in very different settings and with different levels of professional autonomy. One particular thing they shared with the NCMs was the aspiration to provide adequate support to their shared patients. 8 Based on our findings and the participants’ descriptions of NCMs as crucial allies, it seems that the opportunity to collaborate with the NCMs was welcomed. Their descriptions of how having someone to share the responsibilities with had relieved some of their workload leaves the impression that they had been lacking this in the time before the NCMs were employed. In their everyday work, which was targeting patients with extensive physical and psychosocial needs, gaining collaboration partners such as the NCMs – who could help gather the treads and provide access to valuable information – was highly appreciated. This was reflected in the overall positive attitudes towards the NCMs, which was reflected during the interviews.
Providing care to patients transferring between different locations or levels of care in transitions involves coordination of services and building continuity of healthcare. Such transitional or cross-sectoral care is often challenged by a lack of collaboration, knowledge sharing and acknowledgement between professionals across sectors.27 Complexity in such care only increases in cases with patients experiencing multimorbidity and extensive psychosocial needs. 5 Internationally, it is a general challenge that health systems do not meet the needs of patients with multimorbidity due to the care and treatment approaches being ‘disease oriented’ and targeting single medical specialties, resulting in fragmented care.23 From the perspective of social philosophy, the patients shared by the social and healthcare workers and the NCMs could be characterised as a group who are being wronged by social systems, i.e. wronged by the functioning of institutions and structures in society. 35 Laitinen and Särkelä 35 described how these ways of being wronged are related to the ways social practices are structured. In the context of our study, this has to do with how social practices of both social support and healthcare are structured in ways where certain people or groups of people are at risk of being left behind. It is important to clarify how wrongdoing in this sense may result from what Laitinen and Särkelä call cumulative unintended consequences and the fact that the people enacting the social practices in social support and healthcare may be unaware that they are contributing to a harmful pattern. In the context of social support and healthcare, an example is employees acting in the roles that they have been granted, 35 e.g. the hospital-based staff following standard treatment packages or attending only to health issues that are relevant to their particular medical specialty. They may not be aware of any social practices that are potentially harmful to the patients; however, seen in the perspective of the larger institutions and structures, to patients experiencing extensive physical and psychosocial issues attending to only one thing – one illness or one social problem – may not be helpful. According to the social and healthcare workers in this study, the NCMs were not only crucial allies to them as collaboration partners, but also to the patients with whom they engaged. They described the work of NCMs as truly making a difference in the lives of the individual persons. When speaking about making a difference in relation to reducing inequality in health, the NCMs’ efforts made an impact at the individual level rather than at a societal level. As part of this, it was depicted how the NCMs were not afraid to challenge the system and the traditional ways of thinking within social care and healthcare. Our participants saw the NCMs’ willingness to break free of siloed mentality as something of great importance to their collaboration – and to the support they could provide to the patients with extensive psychosocial challenges in life. Returning to the work of Laitinen and Särkelä, 35 the NCMs’ role and function, and their collaborative capacities, could be understood as attempts to undo some of the social wrongdoing.
Drawing on sociological theory describing different conceptions of social pathology, 36 both the individual and society can be viewed as ill or pathologic. Society can be understood as pathologic if structural systems and organisations contribute to certain groups in society being left behind, hence reproducing inequality in health 36 – as in the case of the patient group described by the social and healthcare workers in this study who were typically given up on and in great risk of falling between the cracks. 8 Just as our participants described the work of the NCMs and the potential impact on inequality in health at the individual level, the notion of social pathology claims that to treat and cure the illness affecting the individual person does not cure the pathology of society. 36 To achieve true changes in the current levels of health inequality, we need to attain multifaceted knowledge about how inequality manifests in real world settings. 37 Such knowledge should be at the very core of the development of complex interventions targeting the specific issue.
A recent study described the everyday work practices of NCMs as something other than usual nursing care, taking the time to support each individual patient in building a network inside as well as outside the hospital organisation. 8 According to the social and healthcare workers in our study, functions such as the NCMs are needed. Collaboration with NCMs made it possible to provide support to some of those people who would otherwise fall through the cracks. Offering more flexible social-care and healthcare solutions is suggested to potentially address some of the health inequality issues we face in these years. The continued specialisation of the care and treatment provided in contemporary hospitals accentuates fragmentation and increases complexity in patient trajectories. The complexity rises with the number of healthcare professionals involved who come from different healthcare services that are typically delivered at different locations. 28 Furthermore, the inability to enact in accordance with the expected norms related to individual rights and duties of patients may leave the most vulnerable groups in society with poor possibilities for accessing healthcare.2,38 This would most likely apply to the patients who the social and healthcare workers and the NCMs collaborated on. The flexible approach used by NCMs when engaging with these patients could be perceived as a potential solution. However, it is a paradox embedded in attempting to fix problems in a fragmented healthcare system by adding a new service and potentially increasing fragmentation and complexity. Based on the continued population development and increasing numbers of people with multimorbidity, healthcare systems need to adapt to be able to accommodate the complexities among patients and the fact that these may be associated with social circumstances. 28 Increased focus on attending to the individual needs of patients in the planning and delivery of care and treatment is pivotal and speaks to the application of person-centred approaches across social-care and healthcare settings. 8
Strengths and limitations
This study comes with certain strengths and limitations, some of which are addressed here. The study builds on interview data as the only data source. However, the research group included researchers with experience within the field of NCM work practices and researcher triangulation was applied to establish trustworthiness of the data and to validate the interpretations made in our study. 39
Reflexivity is an unavoidable characteristic feature in social research, and is concerned with how we, as researchers, are always part of the social world that is being studied, and that the social world and the people acting in it therefore are bound to be affected by the presence of the researcher. 40 In addition, the social constructionist perspective meant that we, as researchers, took on active roles in the co-construction of the studied phenomenon.15,40 A basic assumption related to this is that we engaged in the process, interacting with both participants and the data, hence unavoidably impacting the research. 15 To clarify our different roles and impressions during this research, we have declared our different levels of experiences with qualitative research and how we have contributed in different parts of the planning, conducting and reporting of this study.
As it always applies in qualitative research, 41 the results might have been different if the participants had been recruited by means other than the NCMs acting as gatekeepers. In this study, it is worth considering whether there may be a positive bias because of the purposeful sampling, 16 as our access might have been influenced by a more positive relationship between the NCMs and the social and healthcare workers. As reflected in the study findings, we did find the participants to be generally positive about the collaboration with the NCMs. However, the applied sampling process was considered the most favourable since it provided direct access to those social and healthcare workers whom the NCMs deemed essential to their everyday work.
Furthermore, this study sought to provide nuanced descriptions instead of general descriptions. As such, the findings add to the existing literature on international trends, such as specialisation and fragmentation within the contemporary context of healthcare and social support. It does so by providing descriptions of how support services such as the NCMs were perceived as making a difference in the lives of people, who are considered some of the most vulnerable in contemporary society. Further research should focus on in-depth explorations of the collaborative relationships that are formed in collaborations targeted to patients with extensive psychosocial care needs.
Conclusion
Providing adequate support to people experiencing coexisting physical health issues and extensive psychosocial issues in life is a challenging task that requires attention from across multiple support systems. Collaborating with hospital-based NCMs who were not afraid to challenge the existing institutional structures was perceived by most social and healthcare workers as paving the way for strong collaboration across professional disciplines and social-care and healthcare sectors.
The ongoing development towards more effective and specialised societal systems seems to have created a need for services such as the NCMs, who will act as crucial allies to both collaboration partners and patients to whom highly specialised and effective care and treatment trajectories are not beneficial due to the complexities of their situation, almost like a service working in parallel with and fighting to challenge the established system. Even though cross-sectorial collaboration could be expected to be part of the everyday work practices of traditional hospital nursing care, the way the practices of the NCMs were highlighted as crucial by participants in this study speaks to how this may not be the case.
As part of their collaboration, the social and healthcare workers saw how the NCMs managed to make a difference in the lives of individual patients, but without it affecting inequality in health and illness understood as a societal issue. Hence, the findings of our study underline the continued need for structural changes if we are to address the sustained issues of health inequalities.
Implications
This study contributes with knowledge about how the NCMs, according to the participants, play an important role in establishing and maintaining cross-sectorial collaborations and providing adequate support to people with extensive physical and psychosocial care needs. Our findings speak to how supporting interventions, such as the NCMs, has become a necessity for some groups of people to be able to navigate the highly specialised and effective healthcare system.
Certain characteristics of the NCMs were highlighted as important by the social and healthcare workers in the study. These were related to NCMs taking on the challenge of breaking down the established silos of our social-care and healthcare systems to achieve solutions that are in the best interest of the patient. The NCMs were described as attempting to pave the way for what they believed to be necessary to avoid these patients falling through the cracks – breaking down barriers between support systems to avoid the patients being socially wronged. Building on the accounts of our participants, they contributed something more to the cross-sectorial collaboration than they had experienced previously.
The findings of this study underlie the necessity of providing flexible care and treatment solutions based on the needs, wishes and preferences of the individual patient. In particular, multifaceted efforts are necessary for the group of patients with extensive physical and psychosocial support needs.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.