
Abstract
Simulation-based learning is a learning method used in educational programmes for health professionals. Little is known about nurses’ experiences after a long period of time has elapsed since the simulation. The aim of this study was to describe nurses’ experiences of simulation scenarios and their perceptions of learning 12–18 months after the simulation. An explorative qualitative approach, including three focus-group interviews, was used. A total of 21 nurses participated. Data were collected in September 2017 and April 2018. The COREQ checklist was used to report the study. Three themes emerged: Simulation as a rewarding learning method, Pedagogical factors that affect the simulation and Perception of different roles in the simulation. The findings indicate that 12–18 months after the simulation took place, the nurses could still recall their experiences from simulation-based learning and the cases used. This indicates that simulation is an important method for strengthening clinical competence.
Introduction
Nurses carry personal responsibility and accountability for nursing practice, and for maintaining competence through continual learning. 1 In the European Union, member states should encourage continual professional development, for example, for nurses responsible for general care. 2 Moreover, this continual professional development should cover technical, scientific, regulatory and ethical development and motivate professionals to participate in lifelong learning relevant to their profession. Simulation-based learning (SBL) is a pedagogical method that uses different educational techniques or equipment with the aim of helping nurses achieve further knowledge and strengthen their (technical and non-technical) skills. Indeed, the World Health Organization recommends that educational programmes for health professionals and training institutions use simulation methods at contextually appropriate fidelity levels in the education of health professionals. 3
SBL is used both in nursing education4–8 and for nursing staff in different clinical settings. 4 ,9–11 SBL with manikins has existed since the early 1900s and has increased since the technological development of manikins made realistic practice possible. 12 An integrative review on SBL in the Nordic countries showed that the number of published studies has increased since the early 1990s. 13 Recent studies highlight the use of high-fidelity simulation (HFS) for different professionals, often with different emergency scenarios. High-fidelity simulation enables multiple learning objectives to be achieved in a realistic and secure context for nursing staff. 14 McRae et al. 15 found that nurses’ self-confidence in performing cardiac surgical resuscitation procedures was higher after simulation. Moreover, HFS has been shown to help staff retain the knowledge necessary to perform cardiopulmonary resuscitation. 16 Three months after completing a simulation workshop, nurses reported that simulating different types of cases had improved their performance in both technical and non-technical skills when responding to actual clinical emergencies. 17
The head manager at the medical department at a regional hospital in Norway wanted a collaboration with the university to practice on challenging situations that may occur in clinical practice, through SBL. As SBL was not a frequently used learning method in the medical department, the faculty members wanted to investigate nurses’ experiences of the simulation scenarios and perceptions of learning 12–18 months after the simulation session took place. Although research has demonstrated the utility of different kinds of SBL, there is little research on the time aspect: specifically, what nurses recall after a long period of time has elapsed since the simulation scenario. 18 Therefore, the time aspect was interesting to evaluate in this study.
The aim
The aim of this study was to describe nurses’ experiences of simulation scenarios with a computer-driven manikin and their perceptions of learning 12–18 months after the simulation. The main questions guiding the research were as follows: 1) What were the participants’ experiences with simulation as a learning method? 2) How did the participants experience the cases used in the simulation scenarios? 3) What were the nursing staffs’ perceptions of the hands-on role and the observer role in the simulation scenarios?
Method and design
An explorative qualitative approach including focus-group interviews was used, yielding empirical data on a group level, with social interaction as the source of data. Participants in a group setting will often remember more than those interviewed individually. By utilizing the dynamic through conducting focus -group interviews, the data – and thus the findings – were richer. 19 , 20 A qualitative approach was selected as it has been found helpful for understanding nurses’ thoughts on their experiences. 21 The Consolidated Criteria for Reporting Qualitative Research (COREQ) was followed when presenting the study. 22
Presentation of the project
For more than a decade, SBL with different types of manikins (Laerdal Medical) has been used in nursing education at the Department of Nursing and Health Sciences at the University of (South-Eastern Norway). Through collaboration with a medical department at a regional hospital in a city with approximately 70,000 inhabitants, nursing staff were trained in various emergency simulation scenarios at the university’s preclinical department. The nursing staff included both registered nurses (RNs) with bachelor’s degrees and practical nurses (PNs) with vocational degrees. The medical department was responsible for patients with gastrointestinal and heart failure problems. In October and November 2016, the nurses participated in a simulation of two acute medical scenarios (anaphylactic shock and hypoglycaemia).
The planning phase was inspired by the International Nursing Association for Clinical Simulation and Learning (INACSL), 23 and the faculty members developed the two acute medical scenarios (anaphylactic shock and hypoglycaemia) together with the nurse manager. These cases were selected based on realistic events from the ward that the nurses had experienced as challenging. A manual from Laerdal Medical was used to plan the scenarios.
The simulation workshop was mandatory for the nursing staff and preceded on three different occasions (one for each nursing staff team). It began with theoretical lessons about anaphylactic shock and hypoglycaemia presented by the nurse manager, which was followed by the two simulation scenarios. In each simulation session, the case was presented first, followed by a demonstration of the manikin for the nursing staff, and then a short briefing. Each simulation lasted approximately 10–15 minutes, followed by 25–30 minutes of reflection during debriefing. Three teams of 12 nurses from the medical department participated. The RNs actively participated in pairs during the simulation scenario and the PNs assisted. In total four RNs and two PNs actively participated each time. In the simulation room, one faculty member and the nurse manager were present to provide guidance if needed. A second faculty member – concealed behind a one-way screen – controlled the manikin, provided the patient’s voice, and guided the scenario. The manikin used was Nursing Anne® from Laerdal Medical, a computer-driven manikin. The two faculty members had a long experience with simulation as pedagogical method, and both were educated as facilitators.
During the scenarios, both the Identify, Situation, Background, Assessment and Recommendation (ISBAR) – a mnemonic created to improve safety in the transfer of critical information 24 – and the medical department’s guidelines for hypoglycaemia and anaphylactic shock were followed. The nurse manager played the role of doctor, whom the nurses could call for prescriptions. Observing nursing staff were seated in a separate classroom, watching the simulation via video screen. They were asked to focus on the nurses’ interaction, implementation of the procedure and communication. After the simulation, everyone came together in the same classroom for the debriefing, which was facilitated by a faculty member competent in the process of debriefing. The faculty members from the university, the nurse manager and the nursing staff were all actively involved in the debriefings. During each debriefing, the nurses who participated in the simulation talked about their experiences and what they could have done differently. Feedback was given both from the observers, the nurse manager and the faculty members.
Participants and data collection
All nursing staff (36) who participated in the workshop (actively participated in the simulation scenario or/and observed) were invited by the nurse manager to participate in a focus-group interview. For practical reasons the participants were invited to focus-group interviews on the same day as they had a one-day course at work, on three different days. A total of 21 (58.3%) nurses accepted to participate in the interviews. Due to e.g. shift work, maternity leave, illness, not everyone could participate in the focus-group interview. Before the interview, the participants completed a form anonymously, containing information about their background, including age, education and work experiences.
The participants (n = 21) were divided into the same groups as during the simulation according to work team, with the aim of promoting interaction. In September 2017, four RNs and two PNs participated in the first focus-group interview and seven RNs participated in the second. The third interview was in April 2018 with eight nursing staff participating, five RNs and two PNs (one missing background variables). The nursing staff had not participated in any simulation scenario between the workshop and the focus-group interview. A semi-structured thematic guide was developed (Figure 1).
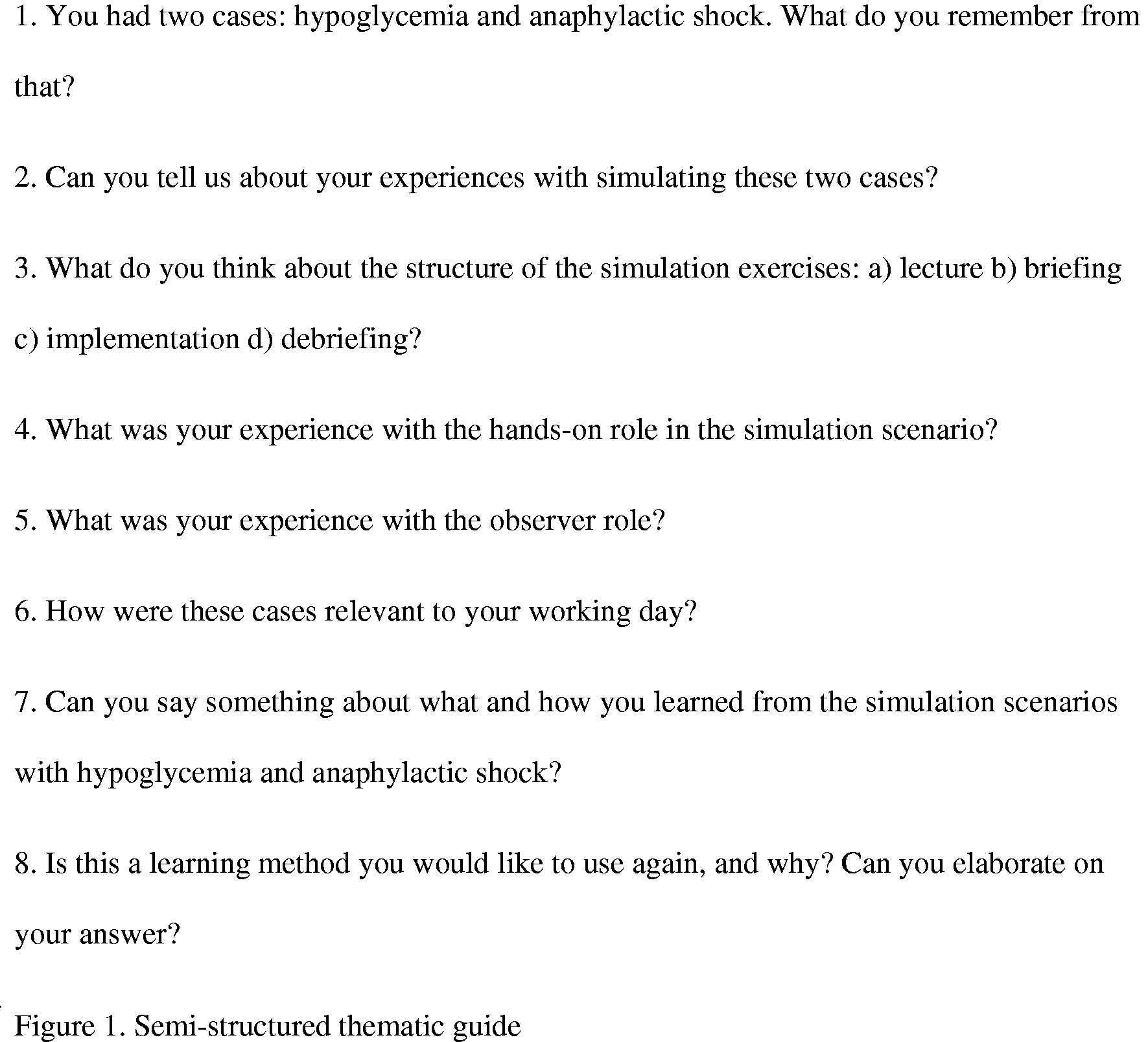
Semi-structured thematic guide.
The faculty members (researchers) were known to the participants from earlier simulation scenarios at the university’s preclinical department. Both researchers had experience in quality research methods and worked as faculty members as associate professor (J.F) and assistant professor (E.S).
The researcher (J.F) moderated all three focus-group interviews, and the researcher (E.S) took notes and asked supporting questions. As a moderator, the researcher (J.F) initiated the interview, and the semi-structured thematic guide was followed. Both researchers focused on creating a setting where all participants could freely express themselves. There were no right or wrong reflections. All focus-group interviews took place at the regional hospital in a meeting room located outside the medical ward and lasted between 45 and 60 minutes. The focus-group interviews were audio-recorded and transcribed verbatim by an assistant. A professional transcription company checked all the quotations and their translations.
Analysis
Qualitative content analysis was performed to systematize, categorize and analyse the data 25 and to create replicable and valid conclusions from the transcribed texts. 26 This method of analysis emphasizes the linguistic, inductive, or text-driven search for patterns. The researchers (J.F and E.S) discussed and reflected on the data at each step of the analysis to strengthen trustworthiness and reach consensus. In this study, the analysis was performed in following steps:
Step 1: Both researchers read all the material from the interviews several times to garner a comprehensive understanding.
Step 2: Meaning units were highlighted and condensed, while still preserving the core meaning. The researchers interpreted the meanings through reflection and discussion over several sessions.
Step 3: Each meaning unit was sorted into a code. Following this, the codes were sorted into categories – a grouping of content that shared a commonality.
Step 4: The data were further analysed. New dimensions emerged, new categories were created, and finally, themes were created. An example of this is shown in Table 1.
Example of codes, categories and theme.

Ethical considerations
The Norwegian Centre for Research Data (NSD) assessed the study in May 2017 (#54162), and the appropriate permission and approval were sought from the nurse manager in the medical department at the regional hospital. Participation in the study was voluntary and all participants were assured that their identity would remain confidential. Written consent was obtained from the participants. At the start of the interview, the moderator repeated the written information the participants had previously been given about the research and clarified ethical aspects. For example, the participants were again informed that all information from the participants would only be available to the researchers, that the interviews would be audio-recorded and transcribed, and that all data would be shredded upon completion of the study.
Results
The participants included 16 (76.2%) RNs with bachelor’s degrees and four (19%) PNs with vocational degrees (one missing background variables) (4.8%). Their ages ranged from 24–67 years (mean 42.16). Their work experience varied from 2–48 years (mean 15.75), and they had worked in the medical department for 2–25 years (mean 10.90). Respondents were mostly women (20), with only one man. The inclusion criteria were that they had participated in the workshop, either in a hands-on role or as an observer.
Based on the content analysis of the three focus-group interviews, three themes emerged: 1) simulation as a rewarding learning method, 2) pedagogical factors that affect the simulation, and 3) perception of different roles in simulation. Categories were identified within each theme (Table 2).
Themes and categories.

Simulation as a rewarding learning method
Two categories emerged from this theme: a new way of thinking and practical and good way of learning.
A new way of thinking
Many of the participants were enthusiastic about the simulation, even long afterwards. They thought it was exciting and represented a new way of thinking. One of the nurses pointed out: … It is a new way of thinking, a rethinking for me, who has worked for 45 years as a PN … … It was a good learning method and a smart way to learn … … it was better than expected …
Good way of learning
The participants expressed that they had the opportunity to learn differently than in theoretical lectures. Moreover, during a typical working day in the medical department, the participants did not know what kind of patients and situations they would encounter, and they felt that simulation was a good way to prepare them for the unexpected. One nurse pointed out: … I feel I am left with something and learned about the things I was unsure of …
Pedagogical factors that affect the simulation
Four categories emerged from this theme: small groups with known members, wanted to repeat, debriefing and realistic cases.
Small groups with known members
Being observed in the simulation scenario was a new situation for many of the participants. Everyone expressed that having small groups was a big advantage, although some said they wanted even smaller groups, which would have made them feel safer. They also highlighted the benefit of knowing each other: working with someone they knew made the simulation less ‘scary’. As one participant explained: … Smaller groups are crucial in a simulation situation, as then you can have fun and learn from it …
Wanted to repeat
One aspect that emerged in all the interviews was that simulation training was something participants wanted more often. Some of them wanted simulation to be a part of their daily work, while others said they wanted it several times a year. Those who had done simulations before, e.g. in educational programmes, felt safer than those who had not. They also emphasized that they wanted more trials on each case: if things did not go well the first time, they wanted to be able to do it again. Those who had felt stressed and uncomfortable during the simulation wanted it to be used more often as a learning method so that they could get used to it. One participant explained: … If I had done this more often, I might not have experienced such stress …
Debriefing
The participants were positive regarding the debriefing after the simulation. They appreciated receiving constructive and positive feedback from colleagues and found it helpful to reflect after the scenario. However, participants also had to be willing receive critical feedback. As one pointed out: … Even though one might not have done anything good, emphasis must be placed on what is positive and good, but you must … hear what is not so good as well … … For my part I think that smaller groups are absolutely the key in a simulation setting. They make it possible to have fun and really get a good learning outcome from it too … … I feel that the debriefing is important to gather my thoughts afterwards … Yes, because one has to do that. One is bubbling over inside, so one has to sort of gather one’s thoughts and decompress – yes, how did it go? Could we have done something differently …
Realistic cases
The cases were inspired by real situations from the nurses’ work, and the participants found the simulations realistic and relevant for their work – even though the simulated situations were not something they encountered on a daily basis. They mentioned that, following the simulation, they focused much more on measuring patients’ blood sugar, even if diabetes had not yet been diagnosed. One of the participants noted: … I will never forget to check blood sugar or blood pressure after this … … I have never experienced that someone has had such a strong reaction to a drug. I was perhaps made more alert to the fact that it can happen. And not least, what to do when it does happen … It was adrenaline, in any case I remember that.
Perception of different roles in the simulation
Two categories emerged from this theme: perceptions in the observer role and perceptions in the hands-on roles.
Perceptions in the observer role
A few participants felt so stressed by the simulation situation that they thought they learned most from observing the others: … It was chaos in my head when I did the simulation, but it was useful to observe the others … … As an observer, you have time to think that ‘oh, there I could have done that’. It will be a completely different setting then, you have time to think more about what you would do even in that situation … … You see much more easily other people’s mistakes when you look at them than when you stand in it yourself. Right? You see it in a completely different way. You learn a lot from looking at others as well …
Perceptions in the hands-on roles
Some of the participants thought the hands-on roles were intimidating, even though they learned from them. As one said: … It was an exciting and intimidating setting, but I learned a lot … … I think that the subject of the simulation, that’s to say the task itself, is actually less important. It’s more about having to work as a team. That was the main aspect of the simulation, that one sees that it works. We know that by and large it works in the department, and so it’s good when one manages it in these situations … … The task itself, it doesn’t really mean much, it’s more that you work as a team … … It’s quite good to see that my colleague does exactly the right things. It means that you can sort of trust them a bit more. Now of course I usually do it, but now I’ve had confirmation that we do what we have to … … I think that maybe I would have remembered more about it if I had been active in both the cases, because then you have kind of been in that situation …
Discussion
The main findings of this study indicate that the nurses still recalled what took place during the simulation 12–18 months later. They also reported SBL to be a good learning method. The nurses also perceived that they had become more conscious about what could happen and the treatments of anaphylactic shock and hypoglycaemia.
Simulation as a rewarding learning method
The nurses’ work experiences ranged from 2–48 years (mean 15.75) with between 2–25 years working in the medical department. The RNs and PNs were thus advanced beginners, competent or proficient, or experts. 27 Despite their extensive experience as nurses, the participants were still positive regarding simulation as a learning method and considered it a new way of thinking. This is in line with the International Council of Nurses’ code of ethics, which indicates that nurses carry personal responsibility for maintaining competence through continual learning. 1 Following their formal education, both RNs and PNs develop more specific competencies, preparing them to meet and manage patients’ needs. 28 Nevertheless, patients’ situations change, or they get diseases that are unexpected; this must be handled properly when it occurs. Identifying and addressing these specific problems through SBL increases the likelihood that medical staff will possess the skills to address them in reality. 18 The nurses in the present study reported that simulation was a good way to prepare them for unexpected situations, which is in line with nurses’ experiences in other studies. 18 , 15 SBL thus represents a ‘pedagogy for the unknown’ (a term borrowed from the military), as it helps nurses prepare for the unforeseen. 29 This is especially important as some of the nurses felt simulation with a computer-driven manikin was intimidating. It shows how important it is to simulate scenarios rarely encountered so that the nurses strengthen their skills regarding different kinds of emergency scenarios. This study shows that, although it was 12–18 months since the nurses had participated in the simulation, SBL is a learning method that they remember.
Pedagogical factors that affect the simulation
Our findings show that the participants wanted small groups and that knowing each other beforehand was important. They also found the debriefing after the simulation to be positive, supporting findings showing that debriefing is a part of SBL that is often highly rated. 16 Participants moreover felt that they received constructive and positive feedback from their colleagues.
It should be noted that learning accelerates when participants are given opportunities to repeat and alter their clinically simulated approach immediately in response to constructive debriefing. 17 Indeed, the nurses in the present study wanted to have simulation training several times a year. Relatedly, Everett-Thomas with colleagues showed that cardiopulmonary resuscitation (CPR) training may require more frequent simulation to help nursing staff retain the necessary knowledge, especially when the skill is rarely performed in their daily work. 15 The cases used here, anaphylactic shock and hypoglycaemia, were rarely encountered during daily work in the medical department, and the nurses wanted to have more trials for each case, especially if they felt they had failed in the scenario. Our results indicate that it is important for nurses to be able to simulate scenarios they rarely encounter in their work on a daily basis.
The nurses found the cases that were used (anaphylactic shock and hypoglycaemia) to be both realistic and relevant to their work. They also noted that they recalled the cases better because they were relevant, although the cases were rarely encountered in the medical department. Similar findings were seen in a study using role play. 30 Interestingly, although the specific scenarios used in the present study did not occur frequently in the medical department, the nurses became conscious of them because of the simulation: they therefore remembered that testing glucose levels is important for hypoglycaemia and that adrenalin is used to treat anaphylactic shock. In a systematic literature review, Hegland and colleagues found that simulation seemed to have a positive effect on nurses’ skills, but its effect on their knowledge had not been established. 11 During workshops, nurses have the opportunity to practise critical thinking, clinical reasoning and clinical judgment, 31 but these skills are not tested in any way. Similarly, in the present study, it was the nurses’ own recollections of their learning that emerged from the focus-group interviews. According to Hallenbeck, 32 more studies are needed of nurses’ recollections of skills and knowledge obtained through simulation, and our findings indicate that this is a promising line of research.
Perception of different roles in the simulation
The nurses’ perceptions of the different roles were related to their experience of the simulation situation. Those who found it stressful preferred to observe instead of taking a hands-on role and expressed that it was useful to observe the others. This is in line with social cognitive theory, which maintains that human beings can learn by observing. 33 It is worth noting here, however, that the discomfort experienced by some nurses while being observed may be related to self-efficacy: that is, a person’s belief in his/her own ability to master a specific task. 33 , 34 Studies show that SBL in different settings promotes positive self-efficacy 35 and self-confidence. 15
Another finding that emerged during the focus-group interviews was the importance of good communication. The nurses who had a hands-on role in the study expressed that teamwork and communication were essential. This is supported by several other studies that have found that SBL affects non-technical skills such as communication and teamwork. 17 , 36
Methodological strengths and limitations
To ensure trustworthiness, we sought to establish credibility, dependability and transferability. 37 Credibility was established by researchers’ experiences and knowledge regarding simulation as a learning method and knowledge of the scenarios used in the simulations. The method was described thoroughly, themes and categories were present and authentic citations were used where they reinforced and highlighted different categories. Concerning dependability, the same introduction and thematic guide were used in all three focus-group interviews. To promote transferability, the methods and analytical processes used for the study were detailed in this article. It should be noted, however, that transferability is difficult in qualitative studies, since the samples are small and it is difficult to reproduce the same result in another context. 38 As we found the interviews to be rich with data, and saturation was believed to be achieved, three focus-group interviews were considered sufficient to answer our research questions.
A weakness of the study may be that the RNs and PNs were mixed in the focus-group interviews. It has been argued that having the same level of education may make people more comfortable sharing opinions and experiences. 39 However, we felt that this was mitigated by the fact that the RNs and PNs worked together in teams in the medical department, as well as in the simulation scenario. Moreover, although the medical department has more RNs than PNs, it was not natural to divide the nursing staff according to job title.
Conclusion
One to one and a half years after the simulation took place, the nurses found simulation with the computer-driven manikin to be a good learning method and mentioned that they wanted to do simulations more often. The nurses highlighted repetition, debriefing, using realistic cases, and having small groups whose members know each other, as important factors affecting their learning. This indicates that simulation is an important method for strengthening clinical competence. The fact that the nurses recall what happened in the simulation scenarios 12–18 months after, implicates that SBL is a learning method that can be used as a supplement to theoretical lectures regarding unexpected situations.
Supplemental Material
sj-pdf-1-njn-10.1177_20571585211032774 - Supplemental material for Nurses’ experiences of simulation-based learning, 12–18 months after the simulation: A qualitative study
Supplemental material, sj-pdf-1-njn-10.1177_20571585211032774 for Nurses’ experiences of simulation-based learning, 12–18 months after the simulation: A qualitative study by Elisabeth Solheim and Jill Flo in Nordic Journal of Nursing Research
Footnotes
Data availability
The data from audio-recorded interviews used to support the findings of this study are available from the corresponding author upon request. The data used to support the findings of this study have not been made available for ethical reasons.
Acknowledgments
Special thanks to the nursing staff at the medical department at for their cooperation and participation in this study.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.