
Abstract
The aim of this study was to examine the learning experiences of nursing students when problem-based learning was used as a pedagogical strategy in simulation-based learning. Simulation-based learning has been integrated in nursing curriculums worldwide to address the lack of clinical competency among newly graduated registered nurses. There is little known about the teaching and learning processes that support simulation-based learning. There is also a lack of research studies evaluating students’ experiences with the integration of simulation- and problem-based learning. Data were collected at a School of Nursing in Denmark, and used data from qualitative interviews with six first-year nursing students who had participated in a course about essentials of nursing where problem- and simulation-based learning were used as pedagogical strategies. Meaning condensation was used to analyse data. Our findings suggest that problem-based learning is appropriate in connection with simulation-based learning, but not ideal for the students’ reflections and self-directed problem-solving. The students found participation in the course very motivating and fun due to realism and engagement from facilitators. However, there was a gap between students’ expectations and the intentions of problem-based learning.
Introduction
In 2006, a national evaluation of newly graduated Danish nurses showed that clinical employers found they lacked clinical competencies, the ability to critically reflect, and clinical experience. 1 As a result, in 2008, a new national curriculum for the bachelor degree in nursing was implemented. At several schools of nursing in Denmark, simulation facilities were developed to address the newly graduated nurses’ inabilities. This problem was not only a Danish concern. Internationally, there was also a lack of competencies among new graduates, and educators demanded more teaching of clinical skills.2–4 Simulation-based learning (SBL) has been integrated in nursing curriculums world-wide 5 for various reasons, including a shortage of clinical placements and a lack of time to practice skills.6,7
Background
In spite of the widespread adoption of SBL in nursing education, little is known about the teaching and learning processes that support this type of teaching. In studies that focus on simulation, the process is often outlined but it can be difficult to find descriptions of the chosen pedagogical strategy.4,8,9 Problem-based learning (PBL) is a well-known pedagogical strategy used in various nursing education settings. According to Pettersen, 10 the overall purpose of PBL is for the learners to be stimulated to restructure information that they already know within a realistic context to gain new knowledge and elaborate on the new information they have gained, for instance by discussing it in groups. PBL differs from more ‘traditional’ approaches as the participant is encouraged to use self-directed learning. The key elements of PBL are a person’s ability to seek out and assimilate relevant information to solve a problem at hand; to analyse, formulate and prioritize key learning objectives within the context of the problem; and collect whatever information is needed to address the problem. It is crucial for PBL that learning takes place in a group setting and that each member contributes to the learning experience. 10 Several studies have focused on students’ experiences with SBL and found the students are motivated and gain self-confidence.11–14 Thus, the perspectives and effect of PBL are complicated. When it comes to skills, there seems to be a consistent positive picture that is immediate and lasting; whereas students who have learned through PBL have slightly less knowledge than those who learned through traditional lectures but seem to remember more of the acquired knowledge.15,16
The focus of this study was to explore students’ experiences with the integration of SBL and PBL, which have not been explored. It is important to illuminate whether the pedagogical intentions and assumptions regarding integration of PBL and SBL match the students’ expectations and experiences to develop and improve the teaching process. The assumptions of this study are based upon our experience from teaching students using SBL and from knowledge drawn from existing literature and studies. Based on verbal statements from students, we expected them to develop a relevant knowledge base leading them to prioritize and to make clinical decisions through PBL and SBL. Further, we expected the students to use responsible self-directed learning and have the ability to identify knowledge gaps.
Research aim
The aim of this study was to explore the learning experience of nursing students when PBL is used as a pedagogical strategy in SBL. The research questions guiding the study were: How does integrating SBL and PBL impact the students’ learning experiences? Which areas need further development?
Research design
A qualitative research design is chosen using semi-structured interviews as we aim to study a human experience related to a certain phenomenon, 17 which in this study is students’ perceptions of the use of SBL and PBL in combination. Throughout the study, researchers have been aware of the importance of being sensitive to participants and the possible changes that might occur during data collection.18,19
Sample
Data were collected during spring 2012 at a School of Nursing in Denmark with an annual intake of 100 students. Interviews were conducted with six first-year nursing students. The students had no prior experience with SBL. There were five females and one male student, with ages ranging from 19 to 30 years. All 25 students who participated in the course were invited to participate in this study by a letter send to their individual mailboxes.
The six students included were the six students who responded to the invitation and may thereby represent the most engaged students. However, the six students had different background in regards to former clinical experiences, level of marks in former assessments, age and gender and we thereby considered them representative for the group of students undertaking the module.
Data collection
Data were collected using a semi-structured interview guide. Questions in the interview guide were extracted based on our experience and knowledge in this area. Interviews were conducted in private and lasted between 30 and 45 minutes. Two of the authors were present during the interviews, but the second author was asking the questions. This format was chosen because the first author was a facilitator during the lectures in SBL.
The specific context of the course is important to clarify. The course consisted of 24 lessons in a simulation lab, divided into four sessions. The overall topic was essentials in nursing. Two academics and three clinical supervisors facilitated the program. Students had no prior experience in simulation and worked in groups of 4 to 6, and medium fidelity manikins were used. Each of the four sessions had a specific focus, clinical assessment related to patients with respiratory problems, circulatory problems, temperature and infection. The degree of difficulty increased with the later sessions, integrating more complex scenarios. Every group had a facilitator giving prompts and hints, and a voice to the manikin. Each group of students was confronted with five different scenarios and facilitators at each session. PBL was integrated with SBL by making the groups responsible for a plan for their actions prior to the scenarios, where they also had the possibility to seek further information by the use of touchscreens placed by each bed and by time-outs where they could ask for guidance by the facilitator as described by Pettersen. 10
In this course, PBL and SBL are used as integrated pedagogical strategies. PBL requires that the students work with problems based in a certain context. This context impacts the way students approach the problem. In this case, the certain context were real-life-scenarios representing patient situations. The course was developed based on the assumption that the use of SBL contributes to a knowledge of real-life scenarios, which is assumed to enhance the students’ abilities to act in a clinical setting.
Trustworthiness and transferability
The trustworthiness of this study is enhanced by researchers giving a clear and distinct description of context and process of analysis. The presentation of the results has been put together with appropriate quotations which is a strategy to enhance trustworthiness of the study. 20
This study took place in only one School of Nursing, which may make transferability to a wider population difficult. However, our findings are supported by previous studies that back its usefulness.21–24
Data analysis
A phenomenological-hermeneutic approach, inspired by Kvale 25 was used to extract meaningful content from the students’ experiences. This analysis focuses on meaning and the technique chosen was meaning condensation, 21 where the meaning of what was expressed by the interviewees is compressed into shorter statements.
The initial meaning condensation starts by the transcription of the interview. 26 Interviews were audio-taped and transcribed verbatim by the first author. To validate the accuracy of the transcription, 21 the second author listened to the tape and read the transcribed interviews. Disputes were discussed until a consensus was obtained regarding what was said.
This analysis was carried out as follows. The complete text was read to get a sense of the whole and each author extracted natural meaning units from the text. The extracted natural meaning units were condensed. To validate the results, each natural unit was discussed in order to create central themes (Figure 1). Interpreting the meaning units in terms of the purpose of the study was done afterwards. The last and fifth step consisted of tying the essential themes into a descriptive statement.
25
This process was carried out manually and no software was used.
Example of condensation analysis.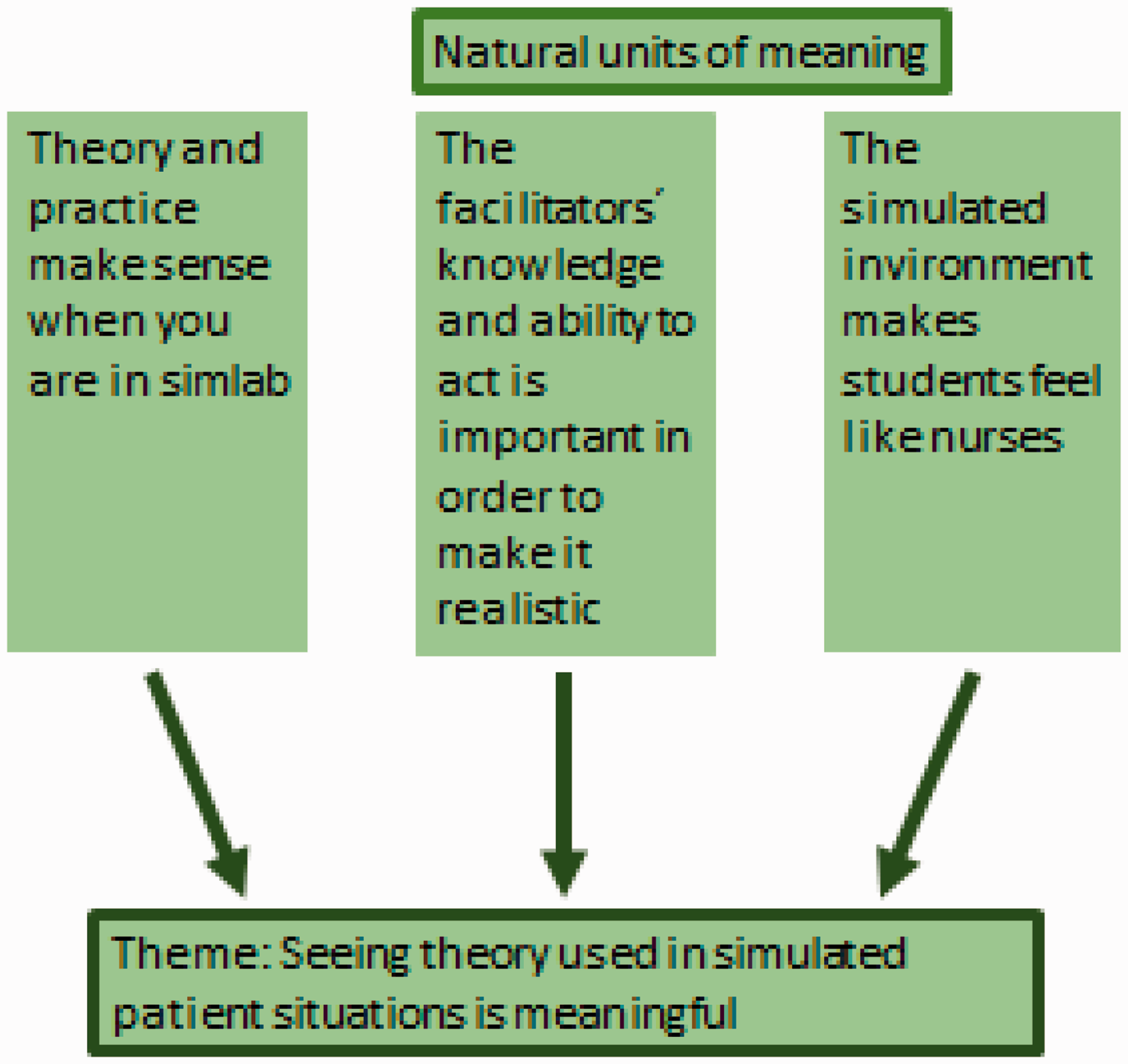
Our findings are presented in Figure 2 as interpreted themes. The researchers discussed and classified the central themes related to the purpose of the study. The essential themes were made explicit in a descriptive statement, as recommended by Kvale.
25
To substantiate the emerged themes, direct citations from the interviewed students are included in the presentation of the findings and in the discussion. Five themes were identified: seeing theory used in simulated patient situations is meaningful, the facilitator’s role is important, teams influence the learning outcome and Bulls eye or not. The data also showed that ‘motivation’ as a theme permeates all other themes.
Themes.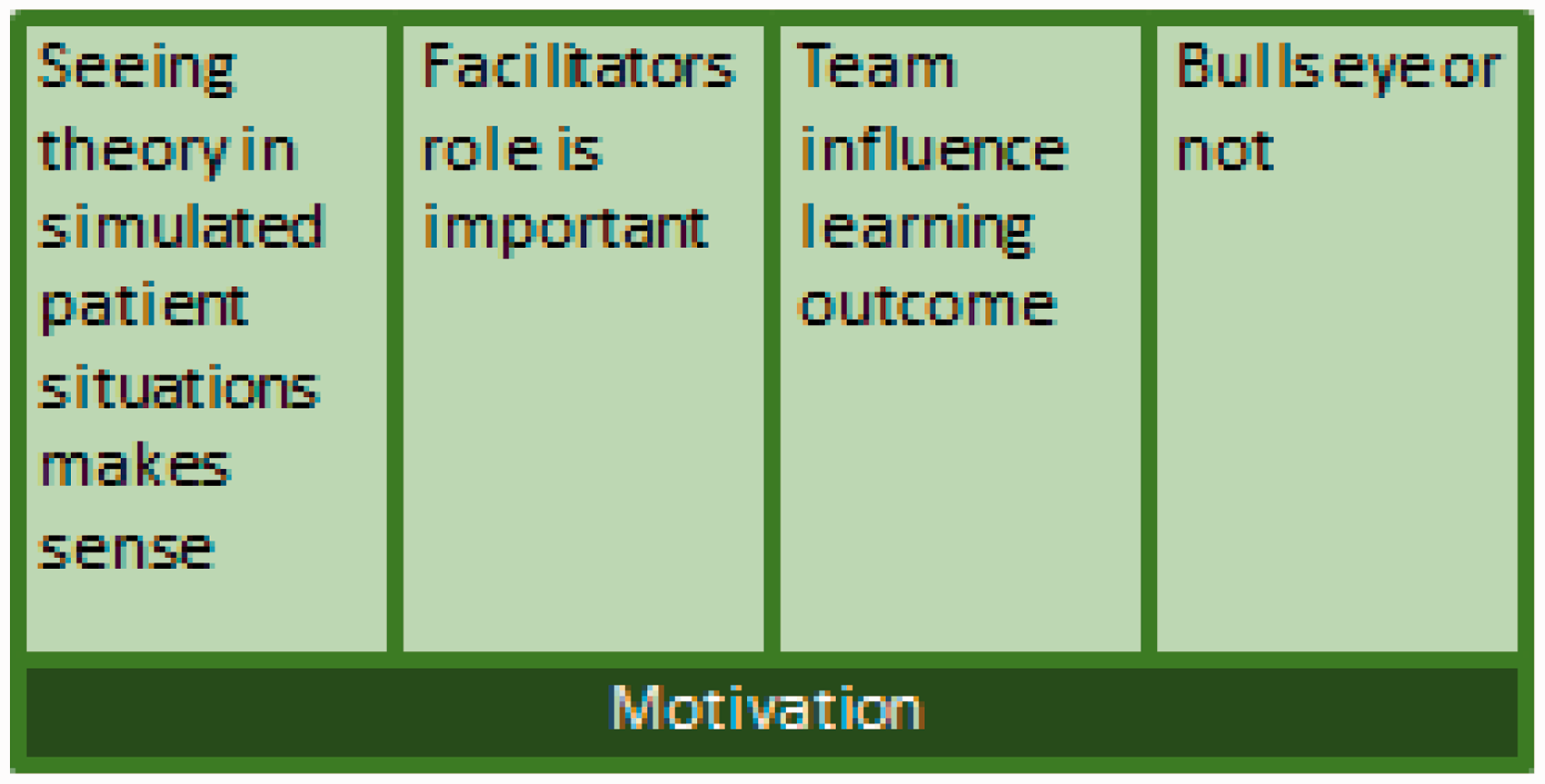
Ethical considerations
Ethical considerations were taken into account throughout the study according to Kvale and the ethical guidelines for nursing research.25,27 The study was approved by VIA University College, Faculty of Health sciences, Schools of Nursing, Denmark. It was not necessary to report the study due to the level of personal information included in the data according to The Danish Data Protection Agency. 28 All participants gave written informed consent. Their confidentiality was assured and researchers made sure that there was no release of identifiable information during and after the study.25,27
Findings
The findings organized in themes are presented in Figure 2. The content of themes will be further elaborated in the following section.
Seeing theory used in simulated patient situations is meaningful
One student put it this way: ‘I think the best way to learn is to have hands on’ and another student said: ‘Well, the best way to learn is like we do in this course, you know, putting my hands into stuff’. The students’ experiences of the course were that it felt different from any other method of learning. They quickly identified that actions have consequences for the patient in the ward, but they feel safe in SBL: ‘ … if you make a mistake it’ll be all right and nothing will happen to the patient. You are here to learn’.
Regarding knowledge students’ expressed that theory and practice make sense. It made sense to see theory from literature used directly in a simulated patient situation. ‘It is possible to read things in books, but you don’t always get it right before you try it in a situation’ said one student. The students felt the course prepared them to enter clinical practice. One student said: ‘It is getting as close to the clinical setting as possible, and you feel safe when you have to enter the clinical setting afterwards’.
A realistic set-up is important to the students’ experiences. One student claimed: ‘Don’t just pretend that you bring a napkin to the patient – go and get it!’ Students not wanting to ‘pretend’ is also related to the role of the facilitator. Students want the facilitator to act in a realistic way. If simulation is realistic, it is also experienced as meaningful.
When asked about ethical and normative aspects, the students’ responses surprisingly all suggested that nursing is defined by human interactions only. Students speak of nursing as something to do with relations between nurses and patients, and the way nurses communicate and approach the patient. One student said: ‘No, I don’t think that these lessons had anything to do with nursing, because we did not get any directions of how to approach the patients’. Another said: ‘Nursing is all about how you talk to the patient’.
It seemed that the students experienced a growing feeling of professional identity when they took the course. One student gained insight into the responsibilities of the nursing profession. ‘I found out that nurses have much more responsibility than I thought, and that is really exciting’. Another student expressed wearing a uniform as important because it contributes to the feeling of nursing identity: ‘It is nice to wear a uniform, you feel a little like a nurse’.
Components of PBL used in simulated patient situations are experienced as meaningful. Realistic scenarios and focus upon problem solving is some of the key factors contributing to this experience.
Facilitator’s role is important
The students also expressed that the facilitator’s role is important. In the analysis, we identified two aspects of the role of the facilitator. One relates to the acting skills of the facilitator and their ability to give the manikin a realistic voice. It was expressed by a student as follows: ‘It depends on which facilitator is by the bed … If they are good at acting or not. But you get a sense of how the patient is getting along’. Another student said: ‘There are big differences. … The facilitator really has to be a good actor to make it realistic’. Another aspect is the knowledge and background of the facilitator. The different professional backgrounds of the facilitators, academics and clinical supervisors from different areas of nursing, was beneficial. One student stated: ‘They might ask about the same thing but they do in different ways, in that way it gives you a lot … ’ and another student said: ‘Meeting different facilitators makes me reflect upon my own identity as a nurse’. It became clear that the students perceived the facilitators as role models. The students felt the professional knowledge of the facilitator had significant meaning. It was expressed in the following statement: ‘You feel safe, because you feel that their (facilitator’s) knowledge is strong, right?’ Students’ perceptions of the facilitator’s role at this point show a need for guidance, which is inconsistent with the aims of the learning strategy.
Teams influence learning outcome
Team dynamics can have either a positive or negative impact on students’ learning experiences. Students felt responsible for the ‘learning possibilities’ of other team members and for them being ‘engaged and active during the scenario’. They talked about having a guilty conscience when they were not prepared for the lessons. ‘Even when you are not “number one” during the scenario you can observe and actually have a better overview. Thereby you can contribute to the discussion afterwards’. One student who was quite negative about the team’s impact on the learning experience put it this way: ‘ … it has been a challenge in SBL because you really have to work closely together’.
A student with a positive perception of team dynamics said: ‘We are different in my team, but it is really good because we complement each other and are able to support each other giving good advice’. Theoretically, weak students find it difficult to raise their voices and to support the team. ‘Evidently there is a great difference in knowledge level among my fellow students, some are really clever and some are not. Then it is difficult to get through, because the clever ones are also the ones to say things fastest’. It was not clear from our data whether the students expected the facilitator to contribute to team dynamics or experienced this.
Bulls eye or not
Some students claim that they learn from mistakes, others that it is of great importance to have the right answers. One student said: ‘The best way to learn is from our mistakes, and that is nice’. The opposite opinion was expressed by this student: ‘I think you remember things better when it has been a success rather than a failure’. Students experienced debriefing as an assessment rather than a facilitated learning situation: ‘These evaluations afterwards they are really assessment-like, I think’.
Motivation
We found that all the themes were related to the students’ motivations. It was evident from data that students found it positive to participate in the course. Students claimed to have fun: ‘We really had fun because we got to try out things with role playing and all that stuff’. Another said: ‘I really like to be in this course … why we can’t have this sort of teaching more often’. There were different reasons for the motivation. Some became motivated because they saw the connection between theoretical knowledge and clinical situations and some students felt like members of a team, and felt safe because they were practicing in a protected environment. It was evident that the students preferred this kind of learning to traditional lectures.
Discussion
Discussion of findings
One of the important findings in this study was that students experienced that seeing theory used in simulated patient situations is meaningful at two levels. One level refers to the student’s ability to make sense of a linkage between theory and practice. The other level refers to students feeling prepared to meet the demands of clinical practice. According to Schön, reflection in action relates to the ability to find connections and describe principles, which seem to work in actual situations. 29 Our data revealed that students felt they could ‘use’ theory-based knowledge in simulated scenario-based situations.
Sometimes students found theoretical knowledge, e.g. anatomy and physiology, hard to grasp, but it made sense when visualized on manikins. This corresponds with the findings of Hope et al., who described that an integration of knowledge takes place when using SBL, 11 and with Leigh who described SBL as a vehicle to move from classroom taught theory to practical action within a safe environment. 23 We found that it was important that students experienced a realistic set up in simulation. This is consistent with the findings of other studies describing that the realism of the set-up has an impact on the student’s perception of the context.22,30 This can also be related to the role of the facilitator. The acting skills of the facilitator were also important. It was not the intention of the learning strategy for the debriefing to be experienced as an assessment. Ziv et al. claims that there must be a balance between being confronted with the mistakes you make and the possibility to transfer knowledge to similar situations in a constructive learning experience. This demands the facilitator creates a learning environment built upon trust, transparency and motivated critical thinking. 31 The course focused on nursing phenomenon related to problems in circulation and respiration. Students were not able to define essential nursing tasks, such as measuring blood pressure, a pulse, or observing the patient. This finding surprised us. When we asked about students’ perceptions of ethical and normative values, their responses were of their perception of nursing in general. In PBL students work in groups, which affect the interpersonal and emotional perspectives. 10
It is expected that conflicts will arise when working in teams, which must be dealt with by the team and facilitator. 10 It is the responsibility of the facilitator to create a pedagogical frame, which provides an environment where students can explore structures and try out new ideas. 32 Students in malfunctioning teams had a difficult time and it was clear to us that it was not sufficient to inform the students that conflicts may arise. The facilitator must take on the responsibility of creating a trustful environment. In malfunctioning groups, egoism and a focus on one’s own interest in relation to the assessments take over. This can result in a lack of learning outcome on the interpersonal level. In well-functioning groups, students felt responsible for contributing to the team. In spite of different levels of professionalism, gender and age, they supported each other and felt like members of a team.
Another interesting finding related to the meaningfulness of simulated patient situations was that students felt like nurses when participating in the course. Professional identity is defined by an individual’s principles and drive, which form through experience. 33 Gaining insight into the nursing profession is an important element of nursing education. Kragh found that the relation between theory and practice is what most impacts the student’s professional identity. Moreover, Kragh sees a tendency that students prefer to have ‘hands on’ instead of theoretical lectures. Development of a professional identity seems to be related to actions and every day practices. 34 It seems that the use of SBL and PBL contribute to students’ perceptions of enhanced confidence with the profession.
The theme ‘Bulls eye or not’ arose because students expressed it was important to give the right answer and do the right thing during the scenarios. An effective clinical nursing practice requires both technical and cognitive components and the use of SBL is a unique opportunity to train both components. 35 An expectation of skills training and action does not fit the learning strategy, where cognitive components are important and the aim is to increase students’ abilities to identify gaps in their knowledge base.
The above does not correspond with the intention that students will become self-directed and autonomous in learning. One possible explanation is that the instructor is teaching in a traditional way rather than facilitating. Another explanation is the students’ perceptions of what and how to learn in SBL. Students expect to perform a clinical skill while being guided and corrected by the facilitator, which is similar to an apprenticeship. In an apprenticeship, students learn by imitation and observation of those who have mastered the activity. 36 According to PBL, 10 it is not important whether students give the ‘right’ answer, it is the process that is considered important along with students self-directed learning.
Students felt SBL was fun. This is consistent with the previous findings that learning using SBL is fun and exciting for students and a good way to practice without harming the patients. 24 Raaheim claims that learning depends on motivation, which is connected to self-image and the ability to cope. Coping is closely related to a feeling of control and the ability to overcome the (learning) task. 37 In this study, the image of becoming a nurse seems to be a motivational factor. Another factor is that when simulation and PBL is integrated it relates directly to clinical practice in many ways, which seems to drive student motivation.
Discussion of methodology
The validity of the findings in this study might be endangered by low number of participants and it can be discussed whether six students is enough to enhance transferability of the findings. According to Kvale, weight is not upon how many informants the study includes when the human experience is explored but whether data is saturated. 25 According to Francis et al., the criteria for what data saturation cover is often unclear. 38 We found that the six interviews were able to answer the purpose of the study but did not specify any other criteria for data saturation which could be considered a weakness.
Conclusion
Our aim was to explore nursing students’ learning experiences when PBL was used as a pedagogical strategy in simulation, and to identify areas in need of further development. Based on the results of this study, we can conclude that the pedagogical strategy of PBL is appropriate in connection with SBL. Students’ do not seem to be self-directed in problem-solving and this need to be taken in consideration when PBL is used as a didactic strategy. It is unclear whether this is related to the students’ earlier learning experiences, ideas of the nursing profession, or the facilitator’s skills. We also found that students in general are motivated when SBL is used, and that PBL integrated with SBL may be a tool for developing professional identity. To develop a course in simulation within the framework of PBL, we suggest making it clear to the students that learning is not all about finding the ‘right’ answer. We also suggest emphasizing that reflection and self-directed problem solving are important. Moreover, the role of the facilitator should be carefully evaluated and explored.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the participants who volunteered to contribute to this work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.