
Abstract
Older people are present in a variety of nursing settings and have distinct care needs. Evidence about the competencies required is crucial when developing the profession. The aim of the study was to describe competence areas relevant in gerontological nursing. A qualitative, descriptive study design was used with 27 participants included. Finnish gerontological nursing professionals who worked at several healthcare organizations and in education were interviewed in five focus-group interviews. The interviews were carried out between October 2017 and February 2018 and were analyzed using inductive content analysis. The study is reported according to SRQR guidelines. Analysis indicated four main competence areas for gerontological nursing: clinical nursing competence; competence in promoting health and well-being; interaction competence; and ethical competence. Registered nurses (RNs) must possess multiple competencies when caring for older people which should be taken into account in nursing and education.
Introduction
Aging is a universal phenomenon, and the world’s population of older people is growing as life expectancies increase. 1 Age structures in various societies are radically changing because people are living longer than before, 2 while fertility rates have fallen during recent decades and continue to decline on a global scale. 1 The global population of people over 60 years of age is expected to double, increasing from 900 million in 2015 to nearly two billion in 2050. 3 In many countries, like Japan, Italy and Spain, people over 65 years of age will make up 30–40% of the population within the next 20 years. 1 However, other countries, e.g. India, Indonesia, Vietnam and most parts of Africa, are expected to have less significant shares of older people in the future. 1 Also, in Nordic countries, including Finland, the number of older people is growing, and life expectancy has increased and will continue to increase. 4
According to the World Health Organization, an older person is anyone over the age of 60 years, while the oldest age group includes people above 80 years of age. 5 However, recent studies have suggested that the definition should be modified so that an older person would be anyone over 75 years of age who is robust and active. 6 Aging is associated with health problems such as increased illness and dysfunction, 7 while active aging optimizes health, participation and safety to improve the quality of life for older people. 8 However, most age-related problems, e.g. lung disease, memory disorders and obesity, 7 are chronic, requiring long-term and geriatric nursing competence. Furthermore, older patients may be frail because of multi-morbidity, polypharmacy and cognitive impairment, 9 the care of which registered nurses (RNs) play an active role in throughout gerontological nursing. 10 All Nordic countries have the same kind of level of care: primary care for basic treatment and hospital care for specialized treatment. Despite Nordic countries’ goals for active and good aging, it should be noticed that while older age groups increase, treatment and healthcare will face new challenges. 4 Therefore, healthcare organizations must ensure that older people are afforded high-quality care, which includes determining whether there are enough staff who are sufficiently competent at caring for the older person. The aim of this study was to describe competence areas relevant for gerontological nursing based on interviews with professionals in gerontology.
Background
Gerontology integrates physical, mental and social perspectives to examine aging and older adults in a comprehensive and multi-disciplinary way. The American Nurses Association has defined gerontological nursing as an evidence-based nursing specialty focusing on the aging process, health protection, and promotion, 11 which requires patient- and family-centered care competencies. 12 RNs face older people in their work in many different care environments and they must have versatile competencies to manage the various situations they will face. Hence, competence in nursing older people will be especially important in the future. Previous studies of gerontological nursing competence have concentrated on nursing homes 13 and community care environments. 9 In these settings, attitudinal, ethical and interactional competencies are critical. Furthermore, pedagogical, leadership and development competencies, as well as evidence-based practice skills, e.g. treatment, patient observation, palliative care and wound care are needed in gerontology9,14 since RNs are often working closely with multi-disciplinary teams and families. 15
There is a need for healthcare staff who are interested in caring for older people and are highly skilled in this area. This is because today’s RN will commonly encounter older patients in acute care, hospital care, home care and long-term care. Gerontological nursing competence is already relevant in current healthcare settings, and will become even more important in the multi-disciplinary healthcare teams of the future, and registered nurses perceive gerontological nursing as a holistic and respectful area of nursing. 18 This notwithstanding, caring for older people is not a particularly popular field among nursing students 16 and they do not often envision themselves working in the field of gerontology. 17
The minimum educational competencies that must be covered during nursing education at European higher education institutions are outlined in EU Directive 2005/36/EC. 19 In Finland, nursing work is carried out based on legislation covering healthcare and its professionals20–22 and based on ethical guidelines. 23 Nursing competencies include the integration of knowledge, professional judgment, skills, attitudes and values 24 into technical and practical skills, interpersonal skills, the ability to work safely on the basis of evidence and expertise, for example, in the medication process. 25 Competence is a holistic term which describes an individual’s overall capacity or ability to perform a certain task successfully. The general competence of graduating nursing students is often related to professional standards, patient safety and the quality of nursing care. 26 There is a lack of studies that cover which competencies are needed in the field of older people nursing, the educational prerequisites for these competencies, and how gerontological nursing competence can be measured.
Aim
The aim was to produce comprehensive information on the competencies of gerontological nursing. The research question was: Which competence areas do registered nurses, geriatricians and gerontological nursing lecturers identify as important for gerontological nursing?
Methods
The presented research applied a qualitative approach with descriptive study design, since qualitative research is suitable for use when there is a lack of studies found that cover the studies area. This design enables participants to have an active role 27 in sharing their experiences and knowledge during focus-group interviews. The Standards for Reporting Qualitative Research (SRQR) guidelines have been used to report the study. 28
Context and participants
The 27 Finnish participants of this study were registered nurses (n = 21), gerontological nursing lecturers (n = 3) and geriatric physicians (n = 3). Out of the total participants, there were 25 females and two males, and they had at least two years of professional experience in gerontological patient care. The participants were from four healthcare organizations, including a university hospital, primary healthcare hospital and two universities of applied sciences, representing different fields of gerontology in hospital, long-term care, home care and educational environments. The interviews were arranged in participants’ own venues and, depending on the size of the organization, participants were coworkers or did not know each other. The healthcare workers were in their own organizations and lecturers participated in focus groups in three different organizations. The majority of professionals were registered nurses, which was an essential inclusion criteria because of this study’s aim. The physicians were included in the study to bring an interprofessional perspective to the geriatric competence needed in patient care, and lecturers to bring insight from the curriculum perspective. Purposeful and snowball sampling were used during participant recruitment to ensure that a sufficient number of individuals working in a special area were reached. 29 The purposeful sampling utilized contact persons to identify relevant interviewees, while a geriatrician known by one of the researchers initiated the snowball sampling process by introducing another geriatrician who would introduce a third geriatrician. The inclusion criteria for participation were: 1) at least two years’ experience in gerontological patient care; or 2) at least two years’ experience in teaching gerontological nursing to nursing students; and 3) willingness to participate to this research.
Data collection
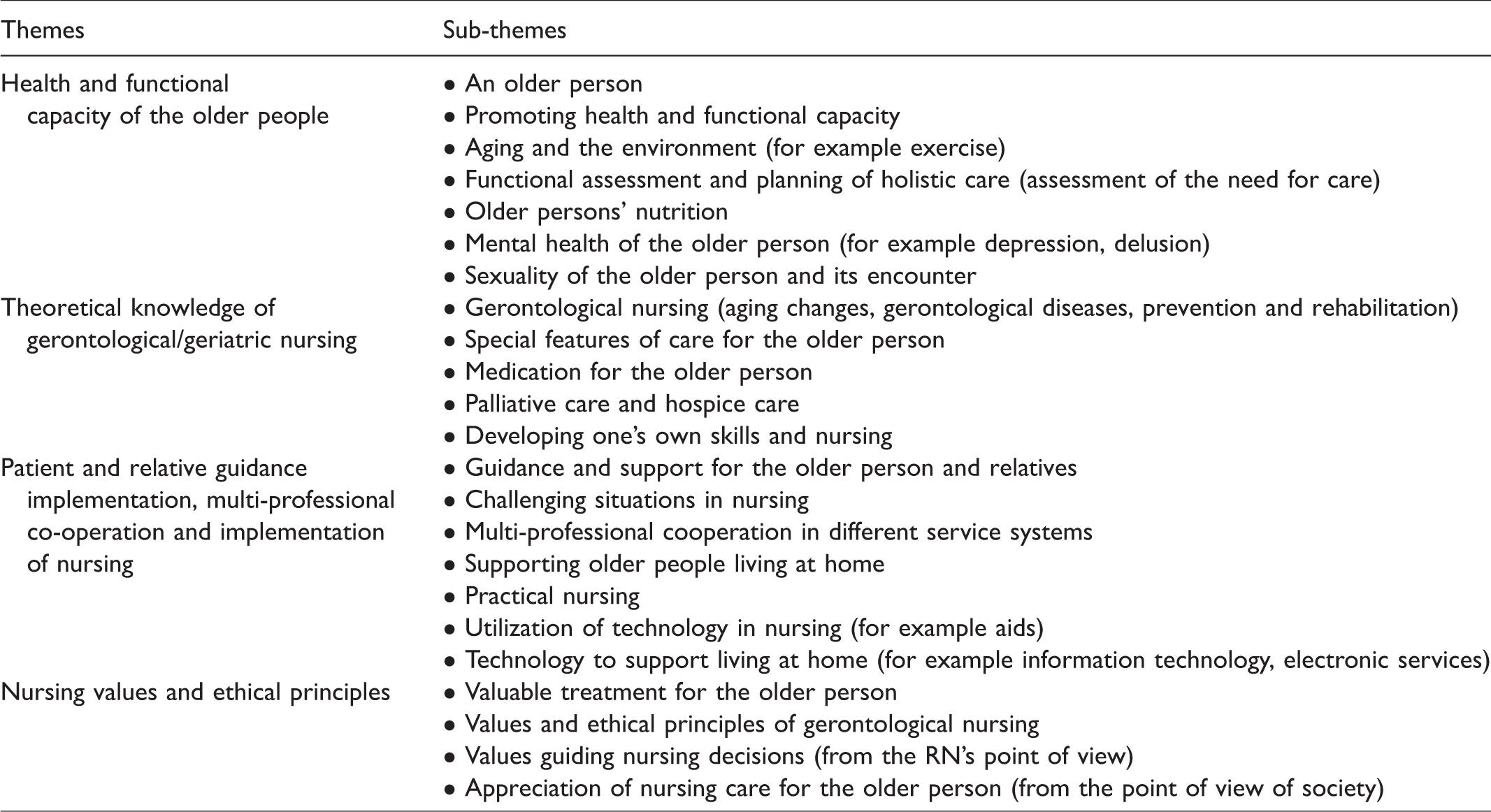
Data were collected by one researcher (AT) between October 2017 and February 2018 with five semi-structured focus-group interviews to understand the phenomenon under study. 30 According to the methodological recommendations, each focus-group interview included 5–6 participants,31,32 from two to three multi-professional groups (RN and lecturer, or RN, lecturer and physician). The interviews were conducted by providing participants with open-ended questions in a freestyle discussion format. The open questions were structured according to the interview themes relating to participants’ personal experiences. The interview themes were formulated from an analysis of current curricula of four Finnish universities of applied sciences and a previous study 33 followed by an evaluation of the necessity and comprehensibility of themes by four gerontological nursing professionals evaluated before interviews. The themes were 1) Health and functional capacity of the older people, 2) theoretical knowledge of gerontological/geriatric nursing, 3) patient and relative guidance implementation, multi-professional co-operation and implementation of nursing, and 4) nursing values and ethical principles (see Table 1). The interviews were conducted according to the framework of the thematic interview, and all interviews proceeded according to the same structure. After going through the themes, participants were asked if they had anything to add, in which case it was further included in data analysis. The contact person at each organization chose an appropriate venue for interviews and invited the participants. Each focus-group interview lasted an average of two hours and was digitally recorded.
Themes for focus-group interviews.
Data analysis
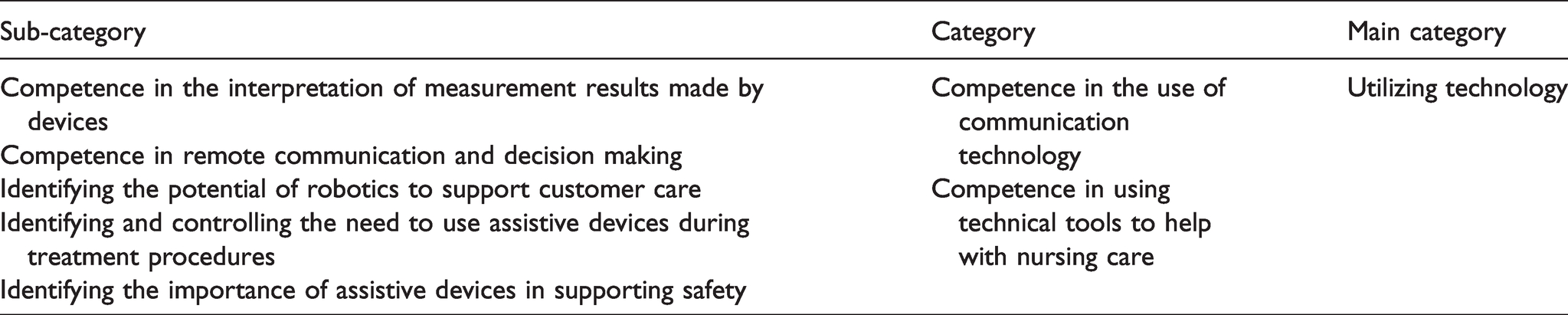
The interview transcripts were analyzed using the following inductive content analysis process. The data were read through several times and organized according to the research question of the study. 34 The analysis focused on subject and context, dealing with the manifest content of the text.35 After condensation, the data were coded into meaning units (n = 221), which were then organized into 95 sub-categories, 35 categories and 15 main categories (see Table 2). The 15 main categories were organized among four themes which represent competence areas that are relevant to gerontological nursing, taking into account that themes may not be mutually exclusive when dealing with quite a large subject.
An example of analysis path under competence area named ‘Competence in promoting health and well-being’.
Ethical considerations
This research was conducted according to the ethical standards of the Finnish National Board of Research Integrity 36 and the General Data Protection Regulation 37 for responsible conduction of research. All four organizations taking part in the study provided research permission and participants, and the information they produced was treated confidentially. The participants were informed about the study’s aim and the voluntary nature of participation before the focus group started, which was confirmed by the signing of informed consent. Informants’ background data, except for gender and occupation, were not collected due to the relatively small sample size and identifiable matters. All data were stored in password-protected computer files, and transcriptions were coded by removing all possible identification of participants. 38 Only the researcher group had the access to the files.
Results
We identified four competence areas that are highly relevant to gerontological nursing: clinical nursing competence; competence in promoting health and well-being; interaction competence; and ethical competence (see Figure 1).

The competence areas relevant for gerontological nursing.
Clinical nursing competence
Clinical nursing competence covered aging changes and geriatric diseases, older people’s medication, nutrition, mental health and end-of-life care. According to the participants, a registered nurse who is competent in identifying aging changes and typical geriatric diseases is able to recognize age-related changes, such as physical aging changes and changes due to sensory impairment. In practice, this consists of identifying normal changes in aging and memory besides the sensory impairment. This competence also requires knowledge of typical diseases and their symptoms, such as memory diseases and fragility syndrome. … aging is associated with the age-related changes, which are taken into account of care. That care for the older person is such an overall process. It needs to be looked at more broadly, not on any particular issue, but on the broader whole. (FG 2, Informant 2) Cutting of drugs is not the most important priority but ensuring that there is everything necessary and nothing unnecessary [for the care of older person]. It is not so much the number of the medicine, but whether there is a purpose for it. (FG 4, Informant 2)
Competence in nutrition included understanding the importance of healthy and energy-rich nutrition, organizing pleasant and functional dining situations, and considering that some older people may require feeding assistance. More specifically, according to the participants, competent RNs need to understand how important correct nutrition is for older people and how aging will influence eating habits. Also, problematic nutritional situations can be faced when RNs must have adequate knowledge of nutritional disorders, e.g. specific diet restrictions, malnutrition, and changes in body performance and composition alongside the importance of the patients meeting their caloric intake requirements. There should be enough meals per day. Not just one good, high-quality main course, but also breakfast, snack, lunch, snack, dinner and evening snack. (FG 4, Informant 2) When new illnesses come in and the ability to function deteriorates, then comes that apathy and, of course, it affects what has happened in the past, whether the spouse has died earlier or there is something else. In nursing, you should have a very sensitive ear. (FG 5, Informant 1)
End-of-life care competence involved nursing a patient who is at the end of his/her life and the ability to face the patient and their family. As such, this competence involved knowledge of symptomatic treatment and good pain management skills. This competence also included nursing skills related to older people close to death, more specifically, abstention from resuscitation, managing terminal care and providing patients a peaceful environment. The ability to face dying patients and their close family members included skills such as providing a warm atmosphere, fulfilling the wishes of the patient and their family, discussing care, and being sensitive to the person’s situation. Let’s take good care of all the things that are left at that moment [for an older person], including a symptomatic treatment, as painless as possible, by providing a warm and humane care. (FG 5, Informant 1)
Competence in promoting health and well-being
This competence included health promotion, evaluating functional capacity, ensuring a safe environment and utilizing technology. Successful health promotion included skills related to support home coping, i.e. offering safe conditions at home and preventive actions. Furthermore, RNs should be able to offer older people a wide range of services, ranging from physical activity to spiritual support, when the need arises. RNs should also be skilled at supporting self-help and holistic well-being; as such, they should recognize when to promote older people’s autonomy, recognize the positive effects of movement and cultural activities, and understand when restrictive actions are necessary. If a person can do something, then we should support them in this activity. (FG 5, Informant 6)
RNs who are competent at evaluating functional capacity know how to make standardized performance measurements using various measurement tools and continuous evaluation of performance. In practice, this means evaluating older people alongside their daily care activities. This includes performing standardized measurements such as following older people’s alcohol use, medication and nutrition. To be competent at evaluating an older people’s functional capacity, an RN must be able to plan the older peoples’ independent living, which includes scheduling preventive health checks, and assessing the home-based services, i.e. understanding the older people’s needs and organizing multi-actor care meetings. RNs must possess a broad understanding of the municipal services to effectively organize older people’s independent living. I would say that ability to function is observed all the time in the care. And that customers’ own operational capability is utilized if it can be utilized. (FG 2, Informant 5) We should also be able to create that coziness in the institution, bring those important objects and belongings into nursing and housing, and not be too institutionalized. (FG 3, Informant 3)
RNs should utilize the best available technology to support their work and ensure older people’s safety. In practice, this mainly involves the use of communication technologies and technical tools such as understanding how to use additional devices, for example, robotics and safety devices, in their work. Telemedicine would then allow this monitoring a little more closely. If the RN goes [to a home-visit] to measure and the doctor makes the diagnosis and prescribes the treatment. Then about these pain pumps, if we get them now sometime, then they would have the digital remote reading capability, … which in turn would reduce home visits. (FG 1, Informant 1)
Interaction competence
This competence comprised respectful encountering of older people, multi-professional cooperation and patient counselling. The respectful encountering of older people included skills related to individual encounters, being attentive, and communication. During individual encounters, RNs implement a peaceful and individual encounter, ensuring the older person has understood the discussion with a customer-oriented approach. Respectful conversations with older people included appreciative, clear speech and valuing the experiences of the person. When we meet older people, we meet adult people and they should be met on an equal footing and not be underestimated. (FG 4, Informant 2) … the multi-professional cooperation could, if necessary, be developed in the ward, and in the primary healthcare even more, between the physiotherapist, the occupational therapist and further with the pharmacist. (FG 4, Informant 3)
Competence in counselling means that a RN can give human-oriented and understandable counselling to older people, family members and nursing students. In practice, this counselling must be clear and understandable, clarify the older person’s needs, and include a clear direction. It takes time to explain [to the patient] and ask if they have understood the instructions and how they can implement it at home. (FG 5, Informant 4)
Ethical competence
This competence area comprised ethical decision making, reflective and analytical competence and ethical behavior towards older people’s sexuality. Ethical decision making included responding to the expectations of patients and relatives in different situations, such as managing the older person’s dissatisfaction with treatment or identifying family expectations. Relatives can assume that when a patient comes to the hospital that the condition improves quickly, and it is difficult to accept that the patient’s condition, however, deteriorates. Then they are dissatisfied with the treatment when they feel that they do not get the help they would expect to get. (FG 5, Informant 6)
RNs need reflective and analytical competencies when processing the matters of learning new competence and being able to explain the development of the industry and the relevance of current competence. This involves identifying their own skills, appreciation of gerontological nursing skills and transferring their own knowledge to others. It also includes skills to acquire new knowledge, such as identifying the need for new learning, and skills to evaluate information sources. Explaining the development includes recognizing the constantly evolving industry and the importance of new knowledge, such as continuing evolution and the meaning of learning new things. It is also an application of different approaches, such as identifying the maintenance of competence and using many ways to achieve the same result. It is important to keep up a continuous development of nursing and maintain our own competence. It requires a RN to be active. (FG 2, Informant 2) It is that holistic existence that human has, the right to be a man and a woman. And there might be the other sex in the future. (FG 3, Informant 1)
Discussion
The continuous growth of the global older population has introduced additional requirements for clinical nursing and nursing education. The results of this study showed four main competence areas for how gerontological nursing competencies should be built: clinical nursing competence; competence in promoting health and well-being; interaction competence; and ethical competence. The diversity of competence areas and multiple competencies showed that nursing staff must possess extensive and versatile competencies to effectively serve the increasing number of older patients that are using healthcare services. The presented findings are relevant to various gerontological settings, from acute and long-term care to home and end-of-life care.
The presented research demonstrated that RNs need clinical nursing competencies to understand the everyday lives of older people. It is pivotal to identify normal aging changes and support healthy older people. 39 Furthermore, it is crucial to know about diseases that older people commonly face; a few specific geriatric diseases, many internal diseases and memory disorders are common with age. 40 In addition to knowledge about which diseases different medications are used to treat and how they work, RNs must consider additional aspects, such as side-effects and polypharmacy, and pay attention to the most recent medical list to ensure that they provide safe care. 25 This study confirmed that RNs need to know nutritional recommendations for older people and pay attention to their patients’ eating behaviors; 41 for example, a patient who is not eating or drinking may have a certain restriction or not like the food. Our findings support earlier studies that pointed out that gerontological RNs need to be familiar with palliative 42 and end-of-life care, 43 having diverse competencies in different levels of palliative care. 44 RNs should also have experience with various pain relief methods, 25 treatment of other symptoms, the provision of psychosocial support and how to face a patient’s family when they are grieving. 45 With aging, people can suffer from several different conditions simultaneously and impaired mental health can be one of them. 46 It is important to identify various changes in mental well-being, as anxiety or depression in older people, for example, increase isolation and loneliness compared to individuals without depression or anxiety. 47 It would be helpful for RNs to be able to discuss meaningful experiences in older people’s lives and to identify the impact of resilience on mental well-being 48 as supportive action. RNs should take into account different aspects of clinical competence to support and evaluate the physical and mental well-being of older people in all its diversity.
In addition to supporting and evaluating physical and mental well-being, the nurse should promote the health and well-being of older people in order to maintain overall health and functioning. Aside from the treatment of diseases, RNs have an important role in promoting individuals’ health 49 to support independent life and living of older people. RNs have to support well-being with their everyday actions and help older patients maintain their functional capacity 50 and, on the other hand, monitor functional capacity to assess autonomy and individual needs of older people. 51 By considering a safe environment and participation, 52 the RNs support the well-being of the older people and recognize an age-friendly environment. 53 Based on our results, RNs should utilize the best available technology in their work for ensuring older people’s safety and well-being. Technology is increasingly used in the care of older people 54 and an RN may be the first person who introduces an older person to some technological solution. Therefore it is critical that RNs understand the functionality of the technology so that they can transfer this knowledge to the patient, which requires organizations to create a positive atmosphere towards digitalization. 55 It is important to evaluate older people’s ability to function and feelings of security, and other factors that make it difficult to live at home and move around, and to be able to recommend and support the use of technological equipment.
This study indicated that RNs’ interaction competence consisted of encounters, cooperation and counselling. Older people should be respected due to their age and life experiences, which RNs can establish with a respectful and caring encounter. 56 Their autonomy and independency should be taken into account by treating them equally and with respect. RNs participate daily in multi-professional teams and cooperating in different fields and organizations demands good communication skills. Multi-professional interventions have positive effects on older people’s physical health and psychosocial well-being, 57 so the RN should take this into account when supporting the well-being of older people. However, the RN is also responsible for counselling the older patient and/or their family when needed, therefore it is important for the RN to be able to implement individual and customer-oriented counseling and guidance for both the patient and his or her family. Individual counseling has been found to be more effective in older patients than group counseling. 58 RNs must be able to carry out a variety of communication with older people in different situations and, if necessary, with different communication support tools. They should also recognize the importance of multi-professionalism in the comprehensive care of older people, and develop their skills for diverse interaction.
Ethical competencies were needed in decision making, doing reflections and facing older people’s sexuality. Healthcare professionals can face dissatisfied patients or family members, varying personalities and/or moods, and abusive behavior. 59 These types of situations are closely linked to ethical competence; for example, RNs should have sufficient knowledge of ethical issues to act correctly when facing an abusive or aggressive patient (i.e. not using restriction). 60 RNs are expected to maintain ethical behavior in every situation, which includes treating and encountering each patient with respect. 56 Moreover, RNs should also understand that it is ethically necessary to develop oneself and improve one’s own nursing skills according to the lifelong learning model. 61 Each RN should be enthusiastic about further developing their skills, and the workplace must afford the necessary opportunities for development. In addition, there is a wide variety of sexuality among older people and it is important that caregivers are able to recognize this and give individuals the freedom to express their own personalities. Furthermore, the ethical approach to sexuality among older patients is to recognize and support different sexual orientations. 62 Strong ethical competence is required for the RN to be able to identify grievances at work, in the treatment of older people and in their own nursing competences, so that the overall well-being of the older people can be guaranteed.
Strengths and limitations
The present study implemented preparation, data collection, and content analysis phases, each of which was carefully documented and performed, to improve the trustworthiness of the research. 63 Furthermore, the study applied the Standards for Reporting Qualitative Research (SRQR). 28 Additional steps were also taken to improve the trustworthiness of the study. For example, the data were de-identified so that the authors would not be biased by answers or background factors. Finally, the chosen sampling methods ensured that respondents who had the best possible knowledge of the research phenomenon were identified to ensure the most diverse understanding possible. As per the usual limitations with relatively small data samples, it is important to state that the main findings need to be further tested in a larger quantitative study if the presented findings are to be generalized to other settings.
Conclusion
RNs working with older people need to be strongly committed to their patients and, for this reason, gerontological nursing requires versatile competencies. Nursing staff need to better involve older patients with implementing holistic nursing, which includes taking into account their life experiences and current situation. We further suggest that the current resources available for gerontological nursing and education need to be critically evaluated to determine whether they are sufficient to ensure that each RN has the competencies required to provide high-quality care for older people. The findings can offer improvements for future nursing and education since basic nursing education should be comprehensive enough to provide a detailed description of gerontological nursing, and continuing education should be readily available to all registered nurses.
Footnotes
Author contributions
Study design: AT, SE, RS; implementation: AT; data analysis: AT, SE, RS, KM and manuscript development: AT, SE, RS, KM, HK
Acknowledgements
We are grateful to the interviewees, who generously shared their knowledge and experience, and thank each organization’s contact persons for their support in arranging the interviews. We would like to acknowledge Sees‐Editing Ltd (![]() ) for improving the language and helping us to communicate our findings to readers of the journal.
) for improving the language and helping us to communicate our findings to readers of the journal.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Finnish Nursing Education Foundation, Finnish Nurses’ Association.