
Abstract
Nurses need versatile competence to care for older people in care home settings. A modified Delphi study was conducted to identify competencies registered nurses and licensed practical nurses need to care for older people in care homes. A total of 38 panelists consisting of experienced professionals in clinical and managerial roles were recruited to identify types of competencies these nurses require. In total, 80 competencies for licensed practical nurses and 81 competencies for registered nurses were identified as necessary. This study has shown that licensed practical nurses are required to have similar competencies to registered nurses in care homes. Nurse managers, nurse educators, and policy makers should pay more attention, to nurses’ work requirements, especially for licensed practical nurses, and support nurses to meet the needs of older people living in care homes.
Introduction
In many countries, older people are provided with care in their own homes for as long as possible, resulting in highly dependent and frail older people entering care and nursing homes. Older people living in these facilities need assistance with activities of daily living, and cognitive impairment and multi-morbidity is common. 1 Care and nursing homes are special living and working environments where many daily ethical dilemmas present themselves.2–4 In these facilities, nurses often have to rely on their own competence since there is not always a physician or nurse colleague available for consultation.2,5 A holistic approach and versatile competence is required of nurses to ensure the wellbeing of older people in care and nursing homes. 6
Competence is composed of knowledge, skills and other components. Agreement about these other components is lacking; however, attitudes and values have been suggested to be ingredients of competence. 7 The application of complex combinations of knowledge, skills, values and attitudes is required in nursing practice and a definition drawing on the holistic conception of competence should be utilized; nursing competence should not be perceived only as either a behavioural objective or a psychological construct. 8 Clinical competence in nursing manifests itself in two dimensions. An ontological clinical competence refers to the inner meaning of nursing and is quite independent of clinical practice, while a contextual clinical competence shows different contextually dependent variations of ontological clinical competence. Clinical competence is both a stage and an ongoing process. 9
The core competencies that all health clinicians should possess include patient-centred care, interdisciplinary teams, evidence-based practice, quality improvement, and informatics. 10 The American Association of Colleges of Nursing (AACN), in collaboration with the Hartford Institute for Geriatric Nursing, has developed recommended competencies and curricular guidelines for geriatric nursing to ensure that nursing students are competent in caring for older adults across all settings. 11 In addition, a European competence framework for health and social care professionals working with older people has been developed. 12 These frameworks should be given attention across different settings. In addition to these descriptions, it is essential to be aware of required characteristics, especially in the context of long-term care, such as in care and nursing homes. While all healthcare professionals benefit from the development of geriatric core competencies, the fact remains that nurses in nursing and care homes face a very different environment than those in acute care.
Interest in research on the role of a nursing home nurse has grown with the emphasis on the work of registered nurses (RNs). Promoting dignity, personhood and wellbeing of nursing home residents and enhancing quality of life are the most important responsibilities of RNs in nursing homes. 13 For example, competence in resident safety, personal care, dementia care, and managing long-term conditions is required of RNs, according to earlier studies.13,14 In addition, there is a list of other competencies essential for RNs working in care homes. 14 Future desirable competencies for baccalaureate-educated RNs working in nursing homes include non-traditional nursing roles, e.g. being a team leader and coach within the nursing staff. 15
There is a lack of differentiation between RN and licensed practical nurse (LPN) roles in some nursing homes.16,17 According to survey findings from the United States, LPNs are sometimes engaged in activities outside their legal scope of practice in nursing homes because of the unavailability of RNs. 18 The most relevant competence categories for all nursing staff in nursing homes and home care services are: health promotion and disease prevention, treatment, palliative care, ethics and regulation, assessment and taking action, covering basic needs, communication and documentation, responsibility and activeness, cooperation, and attitudes toward older people, according to a study by Bing-Jonsson et al. 19
The research context
Our study was performed in Finland where long-term care for older people is primarily provided at home, or, if residential care is needed, in intensive sheltered housing (also known as intensive service housing). 20 The national aim is that 91–92% of people over 75 years of age are living at home and 13–14% of people aged over 75 receive regular home care. 21 In this study, the focus was on nurse competencies in intensive sheltered housing. These units provide both short-term care (e.g. interval care) as well as long-term care. Licensed nurses are available and provide care around the clock. The most dependent and frail older people enter these units; multi-morbidity and cognitive impairment is common. Intensive sheltered housing is non-institutional care, but it differs from institutional care on the basis of the payment source rather than the client population. The resident pays a separate excess share for rent and medicines in addition to the client fee. 22 In Finland, intensive sheltered housing units are often informally called nursing homes or care homes. In this article, we use the phrase ‘care home’ to refer to these intensive sheltered housing units.
In this study, we focused on the work of both LPNs and RNs. Licensed practical nurses are the largest professional group working in Finnish care homes. The Vocational Qualification in Social and Health Care, Practical Nurse education programme includes 120 credits. 23 However, some nurses working in LPN positions are practical nurses who have completed an older education programme dating from before the start of LPN education in 1995. Registered nurses have different education titles, since RN education has evolved over the years. The current education programme for RNs (Bachelor of Health Care, Nursing) includes 210 ECTS (European Credit Transfer and Accumulation System) credits. 24 There is national guidance on staff accountability, duties, and task allocation related to the provision of pharmacotherapy in social care and healthcare units. 25 Otherwise, the current legislation allows a great deal of freedom for care homes to define the duties and task allocation locally.
Aim
The competence of nurses influences nursing home residents’ and their relatives’ satisfaction with care. 26 A poor staffing skill mix may contribute to resident transfers from nursing homes to hospitals. 27 Information is needed about required competencies in competence management, including recruitment and competence assessment and development. 28 Nurse educators also need information on the requirements of nursing practice in the care of older people, in order to ensure the competence of nursing graduates. The aim of this study was to identify competencies RNs and LPNs need in order to care for older people in care homes. A modified Delphi study was used to identify necessary competencies. We sought to gain consensus regarding two issues: 1) what kind of competencies RNs need in order to provide nursing care to older people in care homes, and 2) what kind of competencies LPNs need in order to provide nursing care to older people in care homes.
Methods
Design
A modified Delphi study design was applied. The Delphi technique was chosen since it is a particularly useful method for achieving consensus on issues where none has previously existed.29,30 The classic Delphi study begins with an open, qualitative first round to facilitate idea generation. However, in the modified Delphi Round 1 the panellists are provided with pre-selected items, within which they are asked to consider their responses. 31
Ethics
The University of Eastern Finland Committee on Research Ethics (statement 8/2015) gave a favourable opinion of this research. Participants were informed of the voluntary nature of their participation, so that they could withdraw from the study at any time without explanation. Responding to the survey was considered as giving informed consent. Delphi panellists were reassured that responses would be confidential and that respondents’ identities were known only by the first author. Only ‘quasi-anonymity’ could be guaranteed for Delphi panellists; questionnaires included an identification code. 32
Data collection
A purposive sample of 38 panellists was recruited. 31 The group comprised professionals who worked in Finnish care homes as LPNs (n = 13), RNs, (n = 9) and nurse managers (n = 7), or who were directors (n = 9) of care homes or municipal care services for older people. To be eligible, participants were required to have at least two years’ work experience in intensive sheltered housing as a nurse, manager, or director. A longer work experience in this context was not required since aged care services are currently being redesigned in Finland.20,21 Until recently, institutional care units for older people have been converted into intensive sheltered housing in some municipalities. The Delphi panel members were recruited by sending an email to directors of care homes or administrators of aged care services. Some of the directors or administrators were willing to participate in the Delphi panel themselves. In addition, they informed LPNs and RNs in their units about the study. Nurses who were willing to participate either contacted the researcher directly or their names were put forward by the directors.
Organizations were identified via internet searches and from the Register of Institutions in Social Welfare and Health Care, which is a public register maintained by the National Institute for Health and Welfare (Finland). The aim was to find units from different parts of Finland and from the public and private sectors. In total, 59 care home care providers from the private sector were contacted. Some of these organizations had more than one unit. Permission to undertake the study was granted by 13 private care homes. In addition, the directors of aged care services of two cities were contacted, and permission to conduct the study in their intensive sheltered housing units (n = 9) was obtained.
Two Delphi rounds were undertaken. The questionnaire was in paper–pencil format to encourage participation compared to a web-based version.33,34 The cover letter and questionnaire were mailed to panel members, with the return date being three weeks from when it was sent out for the first round and four weeks for the second round because of the holidays. Reminders were not sent to non-respondents. Round 1 was conducted in October 2015 and Round 2 was conducted from December 2015 to January 2016.
Round 1
The panellists were provided with pre-selected items drawn from an integrative literature review in Round 1.31,32 The review was performed to discover what kind of competencies are required for licensed nurses in care facilities for older people. Since the review did not reveal information from Finnish care and nursing homes, the first author’s experience in clinical practice and management in care homes was also included in the formulation of items. In addition, the research team discussed the formulation of the items and the questionnaire. The holistic conception of competence was utilized; the items were formulated as ‘abilities to do something’ requiring knowledge, skills, and attitudes since the aim was to identify necessary competencies and not to list tasks. 8
In Round 1, panellists’ background information was collected through demographic questions on education, current position, and work experience as a nurse and/or manager or director in intensive sheltered housing units. Panellists were asked to rate the importance of items (n = 60) to assess what type of competencies RNs and LPNs need to care for older people. The 60-item instrument consisted of five competence categories: attitudinal and ethical competence (7 items), interactional competence (12 items), evidence-based care competence (28 items), pedagogical competence (5 items), and leadership and development competence (8 items). A five-point Likert scale was used (1 = not important at all, 2 = not very important, 3 = quite important, 4 = important, 5 = very important), since the scale relates to agreement and consensus. 32 The questionnaire also included open-ended questions concerning the understandability and comprehensiveness of the items.
Demographics of panelists (n).
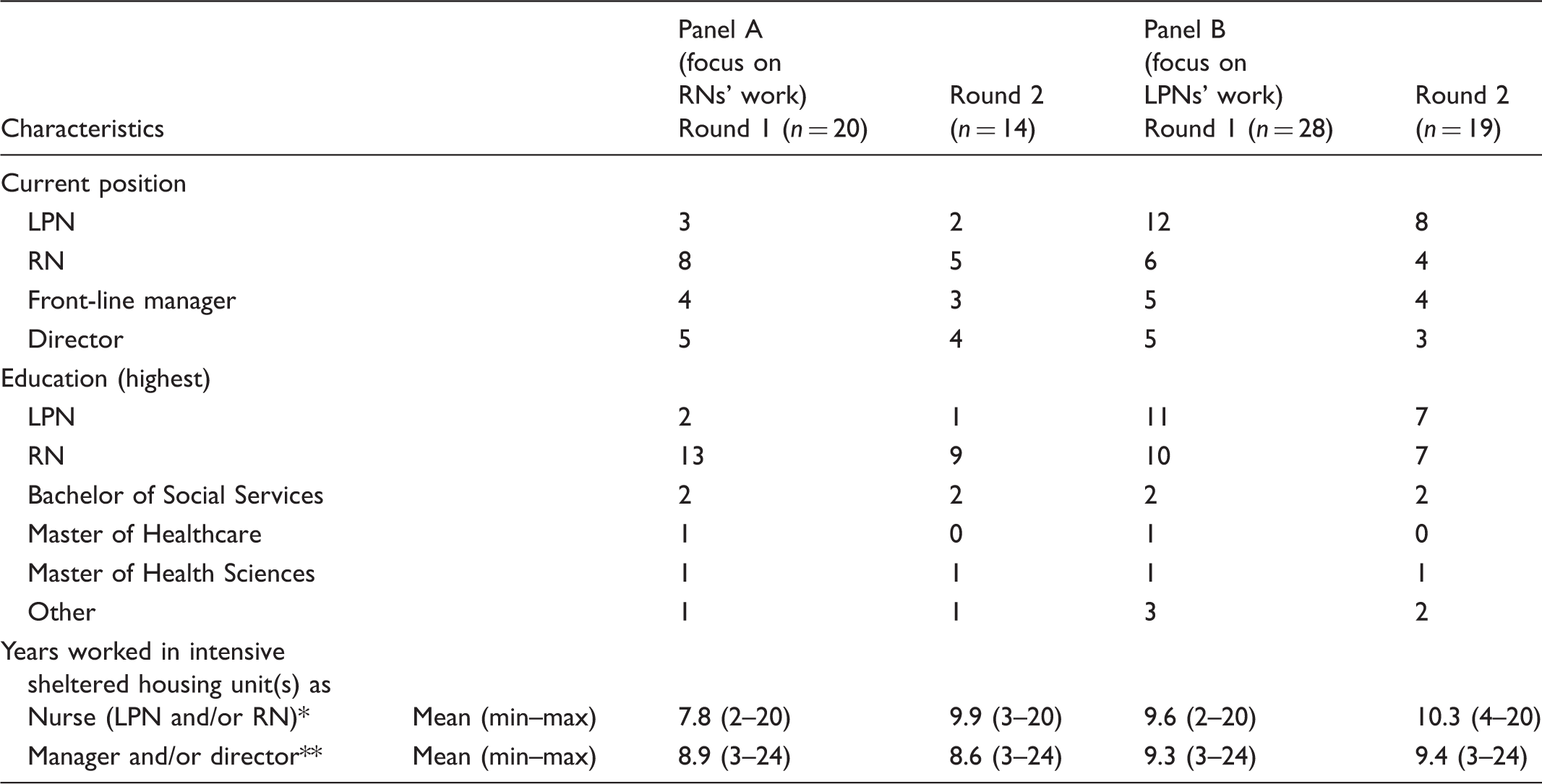
LPN: licensed practical nurse; RN: registered nurse.
Includes only nurse participants’ information.
Includes only managers’ and directors’ information.
Round 2
Round 2 questionnaires consisted of items in which consensus was not reached during the first round, as well as new items that were formulated based on answers to the open questions from Round 1. It also asked for the understandability of the new items, and provided feedback from the first round.
Data analysis
Content analysis and descriptive statistics were used for data analysis. We set the cut-off for consensus in advance as > 85 % agreement on scores ≥ 3 for each item. 30 Options 3 (quite important), 4 (important), and 5 (very important) reflect necessary competence and our aim was to identify all competencies that are needed, not only the most important ones. Quantitative data were statistically analysed using IBM SPSS Statistics 21 software (IBMcorp, Armonk, NY, USA). Open-ended questions were analysed using qualitative content analysis. 35 Meaning units were expressed with words and sentences reflecting knowledge, skills and/or attitudes needed in the care of older people. These meaning units were condensed and then further grouped together into subcategories. 35 Subcategories were then compared with items represented in the first round’s questionnaire to find if they already existed in the list. New items were placed under the appropriate competence category.
Results
Competencies needed in the work of registered nurses (RNs) and licensed practical nurses (LPNs) who provide nursing care for older people in care homes – final results after two rounds.
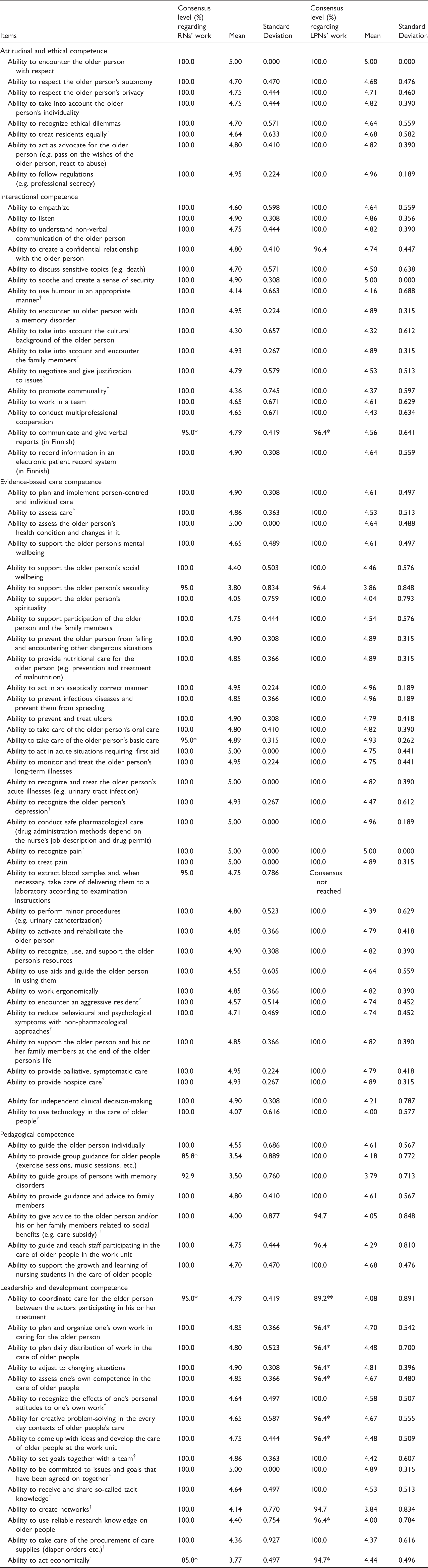
Scale included options: 1 (not important at all), 2 (not very important), 3 (quite important), 4 (important) and 5 (very important). The consensus level was calculated to include options 3, 4, and 5.
One missing value.
Two missing values.
new items generated in Round 1.
In Round 1 the participants were asked to assess the understandability of competencies (n = 60) represented in the questionnaire. The items were well understood, but some comments discussed the multi-dimensional nature of a few items. For example two participants had commented that the ‘ability to respect the older person’s autonomy’ is important, but included the fact that nurses are sometimes forced to act against a person’s will to protect the wellbeing of a person with memory disorder. Two respondents commented about how they perceived the content of ‘ability to support the older person’s sexuality’ as if they were uncertain about the accuracy of their interpretation. Items were not revised during this study. In panel A (n = 20), where the focus was on the work of RNs, consensus was reached on 59 of the 60 items. The item that did not gain consensus was: ‘ability to provide group guidance for older people (exercise sessions, music sessions, etc.)’. In panel B (n = 28) where focus was on the work of LPNs, consensus was also reached on 59 of the 60 items, but the item that not reached consensus was: ‘ability to extract blood samples and, when necessary, take care of delivering them to a laboratory according to examination instructions’. Participants commented that some LPNs take blood samples, but it is not required of all LPNs, and in some units only RNs take blood samples. In total, the consensus levels were very high in most of the items in both groups.
In Round 1 the participants were also asked to assess the comprehensiveness of items (n = 60) represented in the questionnaire. A total of 27 panellists of 31 commented on the comprehensiveness of items. Of these, 26 suggested competencies they thought were missing, and one panel member commented that the questionnaire was so comprehensive that she was not able to add anything. Some of the proposed competencies already existed in the questionnaire, and some did not relate to nursing care of older people (e.g. housekeeping duties), but new items were also found. Qualitative content analysis yielded 21 new items under five competence categories: attitudinal and ethical competence (1 item), interactional competence (4 items), evidence-based care competence (7 items), pedagogical competence (2 items), and leadership and development competence (7 items). Items are presented in Table 2.
In the second round, participants were asked to assess the understandability of new items (n = 21). One panellist pondered whether she had understood the content of three items correctly. During the second round, panel A (n = 14), which focused on the work of RNs, reached consensus on all items. Panel B (n = 19), which focused on the work of LPNs, reached consensus on 21 of the 22 items. The item on which panel B did not reach consensus was the same item as in the first round: ‘ability to extract blood samples and, when necessary, take care of delivering them to a laboratory according to examination instructions’. The research process is illustrated in Figure 1.
Research process.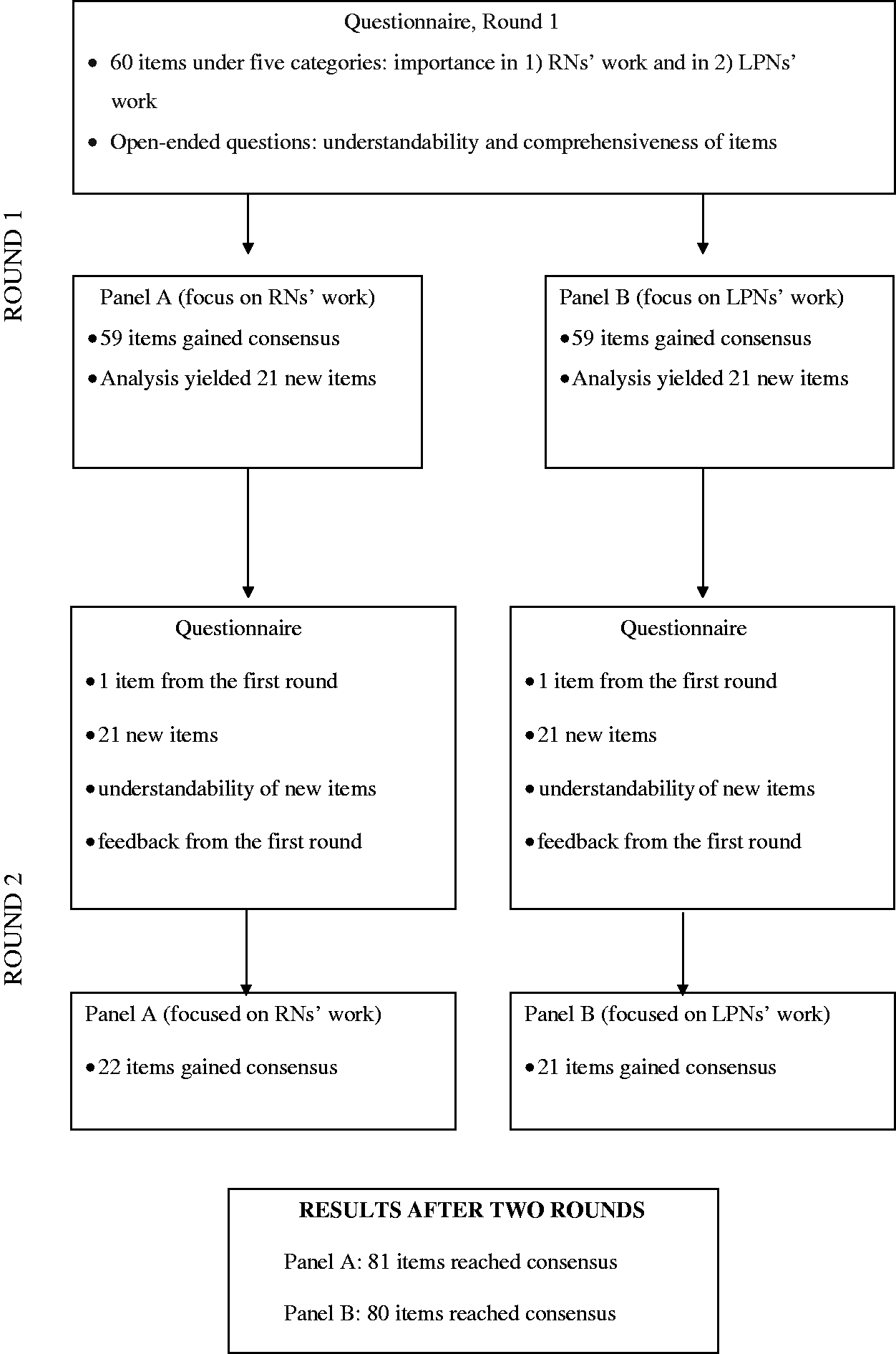
Discussion
Home care has become the predominant care setting for the aged in many countries, 36 and the needs of older people living in long-term care facilities are more complex than ever before. 1 According to our study, versatile competence is required in the work of both RNs and LPNs in care homes. In total, 81 competencies for RNs and 80 competencies for LPNs were identified as necessary.
Our results show that ethical competencies are significant for nurses working in care homes. Ethical dilemmas are common in care homes and residents are often frail and unable to uphold their rights.3–4 Our results are partly consistent with the Delphi study by Bing-Jonsson et al., which is related to the nursing care of older people in nursing homes and home care services. 19 However, some items represented in our study under the ethical competence category are not represented in the instrument developed by Bing-Jonsson et al. 37
In addition, the conceptualization of competence differs from the competence evaluation tool developed by Bing-Jonsson et al. 38 In our study, items are abilities requiring both knowledge, skills, and attitudes, while in the evaluation tool of Bing-Jonsson et al., items are divided into three categories. They are either ‘knowledge’, ‘skills’, or ‘personal attributes’.37,38
Another important finding was the need for interactional competence. Nurses are required to interact with residents, team members, other professionals, and family members, while in the instrument of Bing-Jonsson et al., communication between professionals and between professionals and family members is strongly represented. 37 The majority of residents in Finnish care homes suffer from memory disorders and have difficulty verbalizing, requiring skilful interplay between the nurses and residents. Results revealed some items that specifically reflect the characteristics of the care home context, such as the ability to promote communality.
Our results showed that pedagogical competencies are important in the work of LPNs and RNs in care homes, which was not represented in the study results of Bing-Jonsson et al. 37 This may be explained by the fact that our study focused on the work of LPNs and RNs, while the previous study focused on an entire nursing staff (including assistants). Our study demonstrated that the abilities to guide and teach staff in the work unit, and to provide group guidance for older people are necessary in care homes.
A wide range of evidence-based care competencies are needed in care homes since multi-morbidity of residents is common. Preventive work and end-of-life care are part of nursing care for older people in these units. These requirements are applicable to both LPNs and RNs. The present findings are significant in recognizing the need for a holistic approach in care homes. Physical, mental and social wellbeing, as well as the need to support the older person’s sexuality and spirituality, were represented in our study; thus, the focus is not only on the physical wellbeing of residents. On the other hand, some items under ‘advanced procedures’ in the instrument developed by Bing-Jonsson et al. 38 are not represented in our study findings, such as ‘use of central venous catheter’ or ‘handling ECG’. The items under the leadership and development competence category demonstrate that the work in care homes also requires competencies not traditionally associated with nursing expertise, which is in line with international experts’ visions regarding the work of baccalaureate-educated RNs in nursing homes. 15 In addition, our study results are in line with the list of competencies essential for RNs in UK care homes. 14
The current study found that the competencies RNs and LPNs need to care for older people in Finnish care homes are mostly similar. This can be explained by the fact that in Finland, LPNs often work alone in care homes during night shifts, and RNs are not always available at weekends. LPNs must be able to make independent clinical decisions, and they frequently need to rely on their own competence. In addition, the current laws and regulations in Finland do not precisely define tasks and actions that LPNs are permitted to undertake, except tasks related to the provision of pharmacotherapy. The employer is responsible for task allocation in the care home.
According to international experts, it is necessary to create a long-term care home environment in which the RN role is differentiated from that of other team members. 39 Otherwise, there is a risk that RNs do not operate at their full scope of practice and LPNs end up performing tasks they are unprepared to perform. On the other hand, it is evident that RNs already have a different role, though it may be little difficult to recognize. For example, they guide and teach other nursing staff and are role models in their work communities. Our study identifies the competencies that are necessary in the work of RNs and LPNs and it does not explore how in depth the knowledge and these skills need to be in the identified areas. It can be expected, however, that more in-depth competencies in these required areas are necessary to perform the duties of an RN compared to the duties of an LPN.
It is notable that this study was undertaken to identify nurse competencies required for LPNs and RNs who provide care for older people in care homes; the aim was not to get an overall picture of all duties and required competencies. For example, LPNs’ duties in Finnish care homes can include housekeeping, which requires other competencies aside from the ones represented in this study.
Strengths and limitations
During the first round of this Delphi study, the panellists were asked to provide responses to pre-selected items.31,32 They were also provided with the opportunity to raise new issues regarding the competence needed to provide nursing care to older people in care homes. However, it should be noted that this kind of procedure can introduce bias by psychologically pressuring participants to alter their views based on items already existing in the questionnaire. 30 The procedure may also reduce participants’ ability to freely express their opinions. 40 However, asking participants to generate all items by themselves would have been very time consuming and challenging, since a wide range of competencies are needed. In this study most of the participants (26 out of 31) proposed at least one item they felt was missing from the list of items. The Delphi method does not allow participants to discuss issues; however, a possible disadvantage of face-to-face discussion is that certain individuals can dictate the direction of the discussion. 29 The study avoided this disadvantage, which is important, since there were nurses, nurse managers, and directors in the same Delphi panel.
Representativeness related to a Delphi study is assessed on the qualities of the expert panel rather than its numbers. 29 A purposive sample was recruited. There are about 1300 care homes for older people in Finland and panellists in this study represented only 22 care homes. However, according to earlier studies, there are more similarities than differences in Finnish public and private care homes’ organizational culture.41 Nurses’ work differs mainly during night shifts, when nurses’ actions in public care homes focus on nursing, while nurses’ work in private care homes includes other duties (such as housekeeping duties) in addition to nursing. 41 In addition, the resident population in all Finnish care homes consists of the most dependent and frail older people.
A Delphi study offers a snapshot of expert opinions which can be used to inform practice or theory. 31 This study is one step in the process of developing a measure to evaluate nurse competence in care homes. The identification of required competencies is an essential step towards high-quality care. The transferability of the study results to care and nursing homes in different countries may vary, since the resident populations, 42 as well as RN and LPN practices, can vary between care and nursing homes in different countries.
Conclusion
Multifaceted competence is required in the work of RNs and LPNs in care homes. Competence requirements in care homes should be recognized during recruitment. They should also be recognized in nurse education to ensure that graduating LPN and RN students can meet the needs of older people living in care homes. Continuing education is important throughout the nurse’s career. Policy makers’ attention to competence requirements in care homes is warranted. For future studies, more attention needs to be focused on LPNs’ preparedness to meet evolving competence demands, without dismissing research regarding RNs’ work and competence requirements.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research was funded by the Finnish Nurses Association and OLVI Foundation.