
Abstract
Multimorbidity tends to increase with age. Providing care that is individualized and that focuses on the whole person rather than on separate health issues is a challenge for healthcare, due to a lack of coordination and information exchange. In the future, relatives will need to take even more responsibility for their next of kin. The aim of this study was to explore relatives’ views of aspects that create a sense of security and feelings of quality of care related to acute mobile geriatric care for older people in their own homes. Data were collected using semi-structured interviews analysed using content analysis. This study is reported in accordance with the COREQ checklist. Interpersonal factors such as straightforward communication, empathy, having time for the person, a focus on the person, and having a few known caregivers who are easy to contact, rather than more clinical factors, have been identified as central to creating a sense of security and quality of care.
Introduction
Life expectancy has increased in Europe and globally, and the proportion of older people will rise in the coming years. 1 Chronic conditions tend to be more prevalent with old age, and approximately 70% of people aged above 80 years suffer from multimorbidity. 2 Chronic conditions are in this study defined as ‘health problems that require ongoing management over a period of years or decades’, 3 (p.11) and the concept multimorbidity is defined as co-occurrence of multiple chronic conditions (≥2 diseases) in the same individual. 4 The prevalence of multimorbidity increases with age and is more prevalent among women and people in vulnerable socioeconomic situations. 5
Older people living with multimorbidity who experience high symptom burden might experience feelings of frailty and alienation relating to their own body. 6 However, older people who are able to manage their own activities of daily living are more likely to experience good health. 7 Keeping this in mind, it ought to be a major goal in healthcare to alleviate suffering from diverse symptoms, preferably from a holistic perspective. 6 The different needs of older people with multimorbidity are increasingly challenging for today’s healthcare. Traditional healthcare is usually organized into organ-specific care; accordingly, it often fails to meet the complex needs of these patients. 8 In addition, in healthcare there is a focus on ‘single-disease guidelines’ and applying numerous guidelines as separate entities to one individual may increase the risk of, for example, drug interactions. 9
Even though most beds in hospitals are occupied by older people, the healthcare system seems to disregard their specific needs, and there is a widespread understanding that ‘acute care is not the right place for older people’. 10 (p.40) When care for older people with multimorbidity living at home is not dealt with through specialist care adapted for older people, it is often fragmented, resulting in inadequate care, including a lack of coordination and information exchange between healthcare professionals, patients and their families. 11 Supposedly, a fragmented care system for older people with multimorbidity living at home results in them being increasingly more reliant on support from people within their social networks. Thus, relatives will need to take even more responsibility for their older family members living in the community.
The quality and type of relationships between relatives and the older person impact their caring experiences and their readiness to take on the role of caregiver, sometimes as the primary caregiver. 12 Being a primary caregiver has been shown to be related to less choice when taking on informal care. 13 Relatives provide different types of support (e.g. invoices need to be paid, laundry needs to be washed), often over a long period of time. The care might take different forms over time, from anticipatory care (e.g. being there ‘just in case’ the older person needs support) to instrumental care (e.g. helping with personal hygiene) or preservative care (e.g. preserving the older person’s sense of self). 12 Informal caregivers might need different types of support in their caregiving role, such as information, training and relief. 14 , 15
The increasing number of older people with multimorbidity combined with a lack of co-ordination for the care of older people has led to different care forms having been implemented in recent years. One example is that of rapid response teams 16 which were developed in the UK to prevent hospital admissions and support independent living. Other examples are mobile health units adapted for people with complex care needs. 17 , 18 When care forms based on Comprehensive Geriatric Assessments are compared with usual care, there is a reduction in days in hospital and mortality, and increased feelings of security. 18 However, even though the older person is enrolled with a mobile health unit, relatives are usually the primary caregivers who support the person most of the day, and in this context the formal care is complementary to informal care. Subsequently, it is of interest to explore relatives’ views of aspects of mobile health units that create a sense of security and feelings of quality of care for older people in their own homes.
Method
This study has an inductive qualitative design, using individual interviews with relatives that were analysed using qualitative content analysis. Content analysis is a suitable method when analysing a large amount of text data by coding and cluster comparable meaning units. 19 Consolidated criteria for reporting qualitative studies (COREQ) 20 have been followed in the reporting of this study.
Study context
This study is a follow-up of an implementation of an acute mobile geriatric team (MGT). The MGT included geriatricians and registered nurses (RNs), occasionally also occupational therapists and physiotherapists, referred to here as GER-ACT. The main objective of GER-ACT was to develop a care form that gave a sense of security to patients and families and focused on the older person living in ordinary housing. This care form could offer acute care interventions, in collaboration with social and primary care in the community, within a proximity area of a county hospital in the south-east of Sweden. The team, specialized in the care of older people with complex needs, consisted of geriatricians and RNs from a geriatric clinic at a local hospital.
Participants and recruitment
The inclusion criteria were: 1) relative of every third older person admitted to GER-ACT who was living in their own home from 1 December 2016; 2) being able to speak and understand Swedish; and 3) being able to consent to an audio-recorded interview. The GER-ACT provided a list of every third older person who was admitted to the team (of a total of approximately 36 older persons during the data-collection period) and contact information for a relative after receiving consent until 12 persons had been included (Table 1). Two older persons did not have any close relatives and were excluded from the study. No relative declined to take part in the study.
Sample characteristics for the informants.
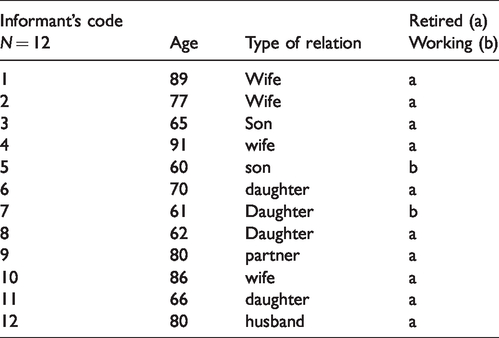
The average age of the 12 relatives in the study was 74 years, ranging between 60 and 91 years. Eight women and four men were included. Of the relatives, six were daughters or sons, four were wives, one was a husband and one was a partner. The spouses (wives/husband/partner) were co-habiting with the older person. The educational backgrounds of the relatives were four with post-secondary education and eight with secondary education. Two were still working at the time of the interview and ten were retired.
Data collection
Prior to the interview, the informant received verbal and written information about the study aim, the procedures and their right to withdraw at any time without explanation. The informants were first contacted by telephone. Written consent was obtained from all informants. The first author conducted semi-structured interviews
21
with the relatives at a place of their choice. Seven interviews took place in the informants’ homes, and five at the workplace of the first author. At one interview, the older person was present, but did not take part in the interview. The interviewer had no previous relationship with the informants. The digitally recorded interviews lasted between 30 and 50 minutes and were transcribed verbatim. An interview guide covering the following areas was used:
Demographic (age, sex, birth, relationship, education, profession/employment) Sense of security and feelings of quality of care relating to GER-ACT. An example question: What is the meaning of sense of security in relation to care at home? Probing question – Could you please give an example?
Data analysis
In this study a conventional content analysis 19 was used for interpretation of the data content. Firstly, the analysis commenced by repeatedly reading the transcribed interviews to get a general impression of the whole data set. Secondly, open coding close to the relatives’ own statements was conducted. The parts of the texts where relatives spoke of the areas of interest related to the study were extracted and examined in order to derive codes. This means that noteworthy units of the text, so-called meaning units, were identified, condensed and coded. In addition, the codes were counted, and this quantification supported the grouping and comparison during analysis. Thirdly, the codes were grouped into sub-categories and after comparing similarities and differences, the sub-categories were merged into categories. In this comparison, six cross-running themes were constructed (please see Table 2 for example of analysis of one of the themes). The first author was the primary coder and the second and third authors acted as peer-debriefers. The whole analysis process comprised an ongoing discussion involving all authors.
Example of data analysis.
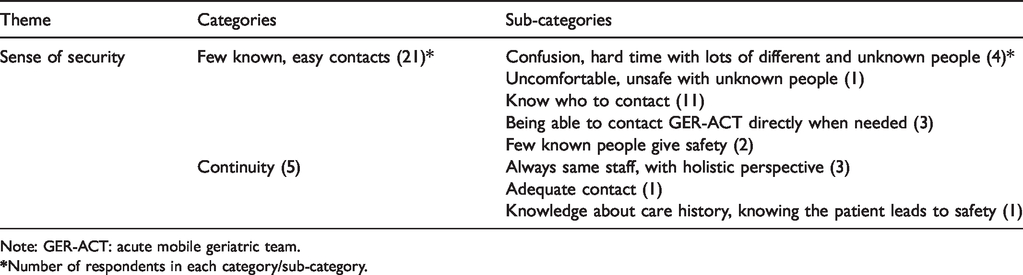
Note: GER-ACT: acute mobile geriatric team.
Ethical considerations
This study adheres to the Helsinki Declaration produced in 1964 by the World Medical Association (WMA) as a statement of ethical principles relating to medical research involving human subjects.22 The study was undertaken with the understanding and written consent of each subject and according to the principles of human research. The study was approved by the Regional Ethics Committee (Dnr 2016/381-31) . All participants in this study were informed both in writing and verbally about participation in the study being voluntary, and that they could end their participation in the study at any time without giving any reason. They were guaranteed confidentiality throughout the process and anonymity in the presentation of the study.
Results
The data analysis identified six themes: Straightforward encounter, Sense of security, The importance of staff, Extended support and help when needed, Impact on relatives’ own lives and Home environment.
Straightforward encounter
The theme Straightforward encounter was found to be most prevalent, in relation to number of codes, for a sense of security and feelings of quality of care among the informants. Aspects such as building relationships based on trust, having time/no stress, and straightforward communication with clear information, answers and responses were important to most informants. Likewise, aspects such as showing empathy, caring and listening, and making patients as well as relatives feel included were talked about. One of the participating daughters talked about how she experienced a ‘straightforwardness’ and appreciated that the team had time to explain things, both for her mother and herself: /…/ they first of all present themselves and take care of all this and sit down to talk. You felt this, that they really cared about the patient when they came home, and my mum who was sitting down next to me, that they even talk to me. That they took the time. This straightforwardness. (8) The most important thing is that they listen to my mother because it’s her that’s sick, and that they actually turn to her and don’t just turn towards me and talk over her head. I think that is important. (7)
Not only how the encounter between the older person was experienced by the relative is of utmost importance, but also the content of the information, bearing in mind that the relative is sometimes the primary caregiver, as with the case of this co-habiting wife: I feel that they aren’t stressed when they come, but they have been open and they look up what they want to and need to, but also answer things I might wonder about. It gives a sense of security! (2)
Sense of security
A few known contacts who relatives easily can get in touch with was perceived by the informants as crucial to enhance feelings of security when it came to care in ordinary housing. Most of the participating relatives described it as being confusing, unsafe and difficult when there were many different and unknown people involved in their loved one’s care. One of the informants said: “Knowing who you can contact and being able to get in contact with them when needed” (6) was important, and this kind of statement was mentioned by the informants in the present study as the single most important factor for creating security and an experience of good quality of care in connection with acute mobile care at home. Eleven out of 12 informants raised this as an important area. One of the participating wives explained that she felt secure when she knew who to contact if she needed support or help: /…/ gained more knowledge about where to turn, because it’s all that, about knowing what I can do if something happens. Because then I know that I might not be able to do that much about certain things, but I know who can come and help me with this. (2) [We had] The same nurse and the same doctor during these contacts, I also thought that was positive and important. That it was the same doctor who did the investigation and the follow-up when [my loved one] came originally. They can relate to the situation before and not just read about it in a medical record, how it was, and it feels more secure when we talk about this. (7)
The importance of staff
The informants emphasized that staff with competence needed for the assignment who undertake thorough medical screening with regular follow-ups were important in terms of ensuring security and quality. Being able to communicate clearly, create comprehensibility and provide care based on needs were other aspects raised by the relatives. One of the oldest informants, a co-habiting wife aged 86 years, put it like this: Competence was shown in that it was both doctors and nurses who came. The fact that both doctors and nurses came provided a sense of security. And you can’t have it any better! (10) Maybe you can’t have good health when you’re 95, but maybe you can get relief and comfort and care that is worth more than perfect medical treatment, but it’s a balance and yes, you can think about it. (6)
Extended support and help when needed
Three of the relatives mentioned the opportunity to get additional help quickly in the event of worsened health as a security factor. Being able to get admitted to the healthcare department immediately with competent personnel and medical equipment when needed and being able to receive extended support at night are areas that were identified as important by the informants. The presence of ‘people and equipment’ (3) is an important aspect of the feeling of both security and quality of care. One co-habiting wife, 89 years old, spoke about when her husband’s health deteriorated: /…/ if they had admitted him that night when he was so ill it would’ve felt like a relief instead of all that worry and stress all night. Yes, I haven’t slept at all. (1)
Impact on relatives’ own lives
Consideration of how the different symptoms and ill health of the older persons affect the lives of their close relatives was emphasized as being important by several of the informants. Their lives were affected in different ways, for example, with problems finding time for their own social lives, and a significant impact on their own energy and health were the consequences described. Informants described difficulties with getting help, support and relief as caregivers. One wife described all the things she had to do for her husband and that she was exhausted: It was this issue with the angina. I don’t know how it happened, but it has built up over the years. Eventually it won’t work anymore. And it’s been a full-time job almost with my husband! So, I think it was enough, I was just finished. And now I can relax a little bit /…/ I feel almost nothing, yes, it’s amazing! (10)
Home environment
The possibility of staying at home in a familiar, calm environment and avoiding having to drive the older person to different healthcare units was highlighted as an important aspect of care by the relatives. One partner described: ‘I could not drive her in our car, so we had to hire transport that she could lie down in every time we went to the emergency room or for an appointment’ (9). Finding suitable means of transportation, having a specific appointment time and long queues and waiting times were mentioned by the close relatives as causing great concern and stress. One informant, a daughter, stated that a familiar, safe home environment reduced the risk of anxiety and confusion for the patient and allowed for greater participation in the care visit. She didn’t have anything else that was life threatening so to say, and it’s much better that they come home because it’s a big deal going away somewhere, especially when she was so tired that she couldn’t stand on her legs. How should we go to the hospital if she sits and hangs like this and says, ‘I’m too tired to stand up’, yes, then it’s just an ambulance, it’s an ambulance and they can carry her out because she cannot walk. So, I think it’s amazing that she can come home, absolutely amazing. (11)
Discussion
The aim of the study was to explore relatives’ views of aspects that create a sense of security and feelings of quality of care related to mobile care for older people in their own homes. In the findings, relatives describe different aspects that could have an impact on senses of security and quality of care, for themselves and for their older relatives. The relatives highlighted interpersonal factors, which might be considered as indisputable in healthcare, such as a focus on the person, empathy, competence and the ease of being able to get in contact with the care team. The informants mentioned earlier difficulties with getting in touch with healthcare involving long waiting times, having to deal with voicemails and many different contacts. The majority want a single contact person or one telephone number to call to get personal contact quickly. This is a vulnerable group of patients who often have significant and complex care needs, and where the older person’s state of health makes it impossible to wait for a long time on the telephone, to have many different ways of communicating for their different needs and to be responsible for the communication between all healthcare providers. In this area, there is a need for healthcare development. This result is also consistent with what previous studies have shown to be important factors regarding quality and security, in which a sense of security is provided by available, accessible and well-known healthcare staff. 15
The analysis in the present study shows that, above all, interpersonal factors rather than more clinical ones have been identified as central to creating security and an experience of quality based on relatives’ perspectives. This is in line with, for example, Van der Elst et al., 23 as shown in their literature review, which further strengthens the results. Based on the challenges faced by healthcare involving a demographic shift towards more and more older people, increasing care needs and limited resources, a challenge can be seen in the development of increasingly close care, often in the patient’s home, which must also take these dimensions into consideration. Self-determination and person-centred care are highlighted by the younger respondents in this study – how should this affect future care developments, as these respondents are the patients of the future? How can and should care be developed towards more co-creation and participation for the older persons and their relatives, while at the same time getting an overall perspective of the individual’s life situation?
Being able to stay at home and receive care in a familiar, calm home environment is seen as very positive by multiple respondents in this study. At the same time, it is important to be able to access the help patients need when they become so ill that the home environment no longer feels safe and secure, both for the patient and for relatives. Creating healthcare structures that enable fast assessments, simple and smooth flows between outpatient and inpatient care, and effective and patient-safe communication pathways, both between care levels and between care and social care, will be central to the future healthcare system.
Methodological considerations
The present study investigates quality and security aspects in connection with acute care interventions at home. One consideration may be whether other dimensions are perceived to be as important in short care interventions compared to long-term care at home. To establish trustworthiness, 23 all the authors read the interviews and the data analysis was discussed within the research team and different approaches considered, until agreement was attained. The first (LT) and last authors (IH) had experience in the field of caring for older people and mobile care of older people in their own homes. The last author has longstanding experiences in qualitative methods. To establish transferability of the present results to other contexts, the procedures, participants, and context of the study have been thoroughly described. During analysis, a summative 19 approach of content analysis was used, not as a quantification per se, but was deemed useful while comparing codes and could help in identifying tendencies in the data.
Conclusion
The research results are expected to provide valuable knowledge for use in the continued development of acute mobile interventions in the home for the older population, benefiting both patients and relatives. In order to tailor programmes for relatives, we need to consider the nuances in experiences related to gender and type of relation. The results of the project are also expected to be important for healthcare’s continued challenges, and developments should meet the needs of the ageing population in terms of quality, organization and economics. Smith and colleagues 24 stress that future research in the area needs to include different perspectives, older persons, relatives and professionals.
Supplemental Material
sj-pdf-1-njn-10.1177_2057158520987048 - Supplemental material for Mobile geriatric team for older people: A qualitative descriptive study of relatives’ views on what creates senses of security and quality of care
Supplemental material, sj-pdf-1-njn-10.1177_2057158520987048 for Mobile geriatric team for older people: A qualitative descriptive study of relatives’ views on what creates senses of security and quality of care by Lena Tö rnfelt, Susanne Roos and Ingrid Hellström in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We thank the Local Health Care Eastern Östergötland who have supported the project.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.