
Abstract
Within the field of neurological disease, it seems that involvement of relatives is of utmost importance since the patients often are affected in several areas (physical, cognitive, and emotional) which impair their ability to participate in decision-making about their treatment and care. This study aimed to illuminate neuroscience nurses’ comprehension of collaborating with and involvement of relatives. Semi-structured interviews were conducted with 19 neuroscience registered nurses. The qualitative data were analyzed utilizing inductive thematic analysis. The COREQ checklist was applied. The analysis identified how collaboration with, and involvement of relatives are perceived as a focus for nursing care and a resource for both patients and registered nurses. Registered nurses having personal experience as a relative find it easier to establish a relationship with relatives. This study emphasizes the importance of the establishment of a trusting relationship between registered nurses and relatives for a positive collaboration and thus involvement of relatives.
Introduction
On 18 March 2020, a temporary restriction on visits to hospitals in Denmark was introduced to reduce the spread of COVID-19. This meant restriction of the physical presence of relatives for hospitalized patients. Exceptions were made for pediatric patients, in labor or postpartum women, patients with severe neurocognitive disability, and patients in life-threatening conditions. The restriction led to changes in clinical practice for registered nurses (RNs) concerning collaboration, involvement, and communication with relatives. Recent studies report changed communication strategies during the restrictions on visits in which remote communication with relatives was achieved by telephone or video conferencing.1,2
This article is part of a larger study that examines the temporary restriction on visits within the field of neurological diseases from the perspectives of patients, relatives and RNs. The temporary restriction is not the focus of this article, but the COVID-19 pandemic gave us a unique opportunity to study RNs’ comprehension of collaborating with and involving relatives in a period in which there was a limited presence of relatives at the bedside and on the hospital ward in general.
Background
A neurological disease has major consequences for patients and their relatives because of its devastating impact on physical, cognitive, social and psychological well-being. These neurocognitive deficits may impair the patient’s ability to participate in decision-making about their own care and treatment and have been shown to place strain on relatives in particular. 3 Involvement of patients with a neurological disease differs from that of many other patient populations by being complex, and an interdisciplinary effort across many settings is often required in which collaboration with and involvement of relatives is important. 4
The involvement of patients and relatives is an important issue on the political agenda in Denmark and is considered a key element in the work of improving quality both internationally and in the Danish healthcare system. 5 It is well documented that relatives’ support and resources contribute to better treatment for patients,6,7 affect the physical, psychological and emotional well-being of patients 8 and ultimately have a positive impact on the safety of patient care.9,10 However, RNs do not necessarily have the same understanding or opinion as to how and to what extent relatives can be involved in the patients’ treatment and the decision-making process. Further, there are many different definitions and terminologies surrounding patient and relative involvement, e.g. involvement, collaboration, shared decision-making and, partnership. 11 Unfortunately, there is little consensus on their meanings and distinctions. Thus, in this article the terminology ‘involvement’ will be applied because it refers to an active doing at the individual level.
Research from the intensive care setting describes relatives as an important source of knowledge for the RNs. Relatives can help paint a comprehensive picture of the patient and thereby assist the RN in delivering individual care for the patient. 12 RNs are most likely to invite relatives to participate in fundamental nursing care, e.g. personal hygiene, assisting eating or communicating with the patient. 13 On the contrary, several studies report RNs expressing resistance regarding the involvement of relatives due to misconceptions of relatives spreading infection, exhausting the patient, and interfering with care.14–16
Existing literature describes several barriers to the involvement of relatives in inpatient care. With respect for the patient, RNs have to balance caring for the patient in terms of protecting the patient's privacy and integrity and meeting the relatives’ need for involvement.17,18 Additionally, RNs try to protect the relatives, fearing involvement may increase their level of stress. 16 Some RNs feel uncomfortable demonstrating procedures in front of the relatives as they are concerned about the way relatives perceive this way of involving them; that they will misunderstand the involvement as an unwillingness from the nurse to care for the patient.16,18 Against this background, the aim of this study was to illuminate neuroscience RNs’ understanding of collaborating with and involving relatives.
Methods and design
This qualitative study has a hermeneutic design. Data were collected through individual semi-structured interviews with 19 RNs working within the field of neurological disease and analyzed utilizing an inductive thematic analysis inspired by Braun and Clarke. 19
Setting
The study was conducted in three different wards at University Hospital Copenhagen, Rigshospitalet in June 2020: 1) a neurosurgical department consisting of 33 beds and a semi-intensive care unit consisting of 10 beds; 2), a neurological department consisting of an acute stroke clinic, two in-hospital stroke rehabilitation units, four acute neurology units, and several specialized outpatients clinics (e.g. headache disorders, dementia, multiple sclerosis); and 3), a 22-bed highly specialized rehabilitation department for patients with severe brain injury (BI).
Participants
The participating RNs were suggested as informants by the ward nurse from the chosen wards. Each researcher informed the RNs about the study and interested participants received verbal and written information about the aim and nature of the study. Then the RNs gave written informed consent to participate. To assure maximum variation in terms of work experience, different age and duty (day, evening, and night shift), and workplace/wards, a purposive sample of 19 RNs was invited to participate in the study. No one refused to participate.
Data collection
To ensure the relevance of the study, a semi-structured interview guide was constructed based on existing literature and questions developed within the research team. The interview guide was pilot tested by conducting one interview each and then it was evaluated. No change was made due to the evaluation. Examples of questions were as follows: Please tell me how it has been to work as a nurse in these special circumstances during COVID-19? Can you provide examples of what has been different under normal circumstances? Do you have any examples of what has been challenging? How have you dealt with the relatives not being present at the ward? The interview guide was reviewed and revised by the entire research team. The interview guide was followed, while, however, still allowing participants space to address their understanding of collaborating with and involving relatives and giving the researcher opportunities to ask extra questions about unexpected but relevant subjects that emerged. A prompting technique was used to create flow in the conversations to make participants feel at ease. The interviews were conducted by all three researchers in the research team individually, thus all researchers were not present at the same time. All interviews conducted in the wards were recorded digitally and transcribed verbatim by the author team. The interviews lasted about 30 minutes each.
Data analysis
The data set was analyzed by performing an inductive thematic analysis inspired by Braun and Clarke, 19 using a computer-assisted analysis: QSR International NVivo version 10. Braun and Clarke's thematic analysis comprises six steps: 1) familiarizing yourself with your data, 2) generating initial codes, 3) searching for themes, 4) reviewing themes, 5) defining and naming themes, 6) producing the report. 19 The analysis process was conducted by all research team members and continued until no new categories emerged and there was agreement on the final three themes.
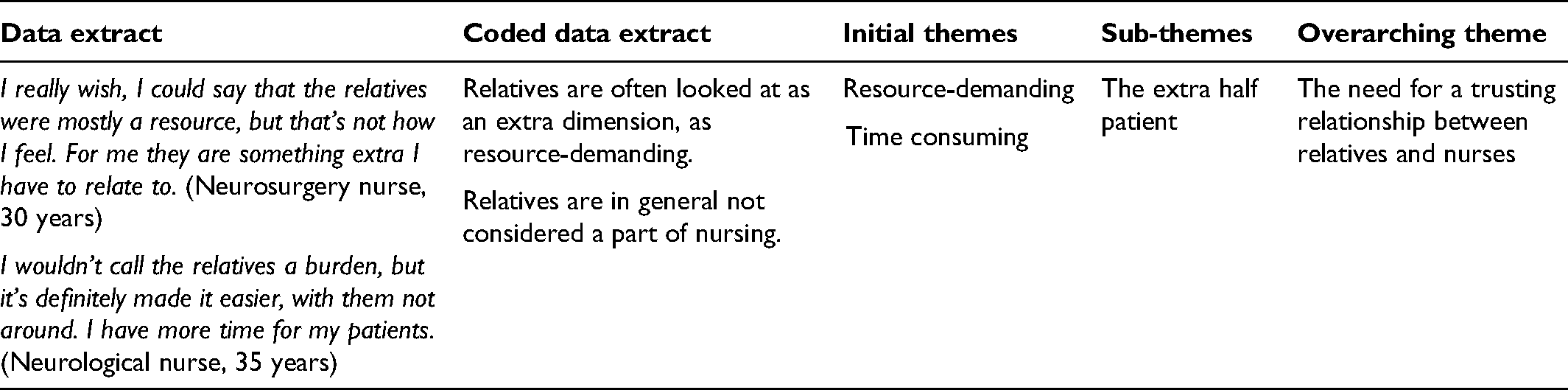
All the transcripts were carefully read by all research team members and all meaningful basic segments were labeled using descriptive codes. The codes describing similar contents were grouped, reviewed, and re-coded if necessary. Subsequently, reduced data from all groups were collated to visualize the emergence of themes. These themes were reassessed to check whether the data were consistent with the research questions and provided enough information. This resulted in some of the themes being subdivided, if their contents were overly broad, or renamed to reflect their contents more accurately (Table 1).
Example of thematic analysis.
Ethical considerations
The study was conducted according to the principles of the Declaration of Helsinki. 20 Written and verbal information was given before obtaining informed consent to participate in the study. Participants were informed of the voluntary nature of the study and that withdrawal from the study was possible at any time with no implications. No participants withdrew from the study. This study received approval from the Danish data protection agency. Data were stored in a closed folder according to the data protection rules and all participants’ names have been changed to ensure anonymity.
Findings
The study participants ranged in age from 26–61 years (median 30), and were all females, working within the field of neurological diseases for 1–30 years (Table 2).
Characteristics of participants.
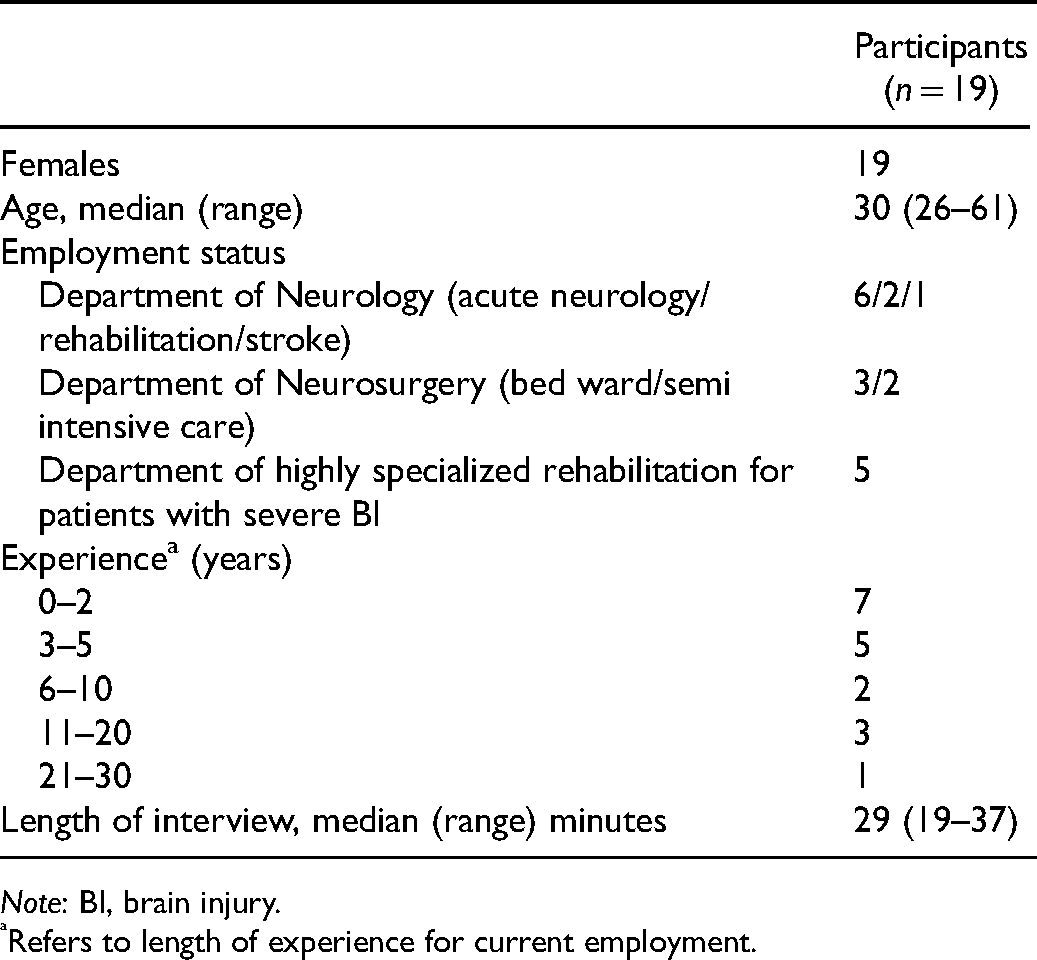
Note: BI, brain injury.
Refers to length of experience for current employment.
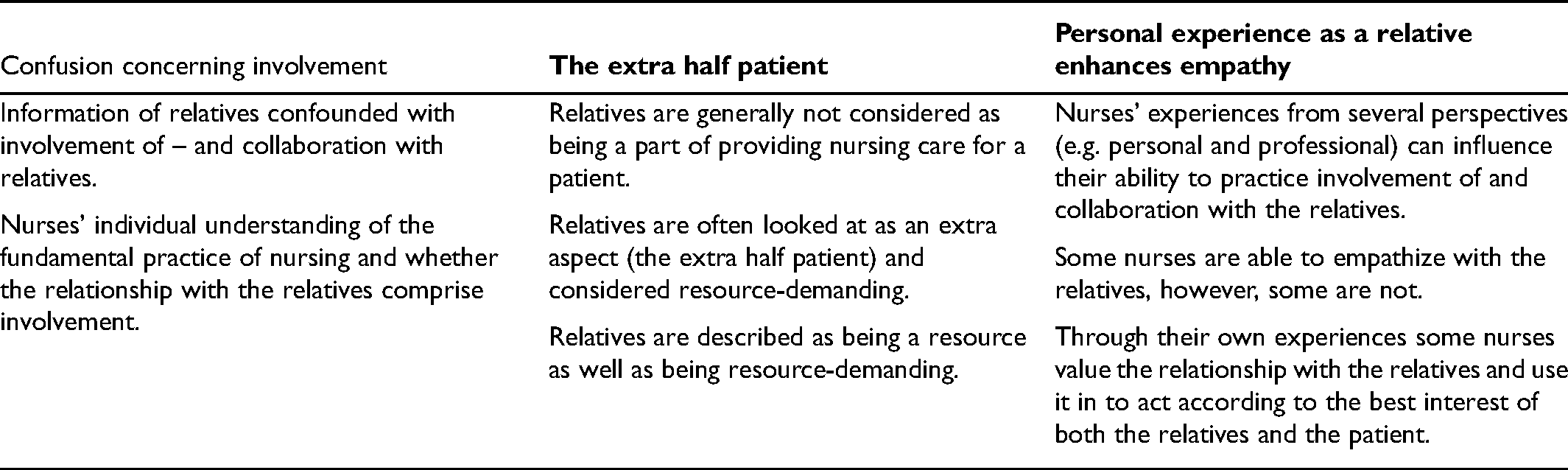
Three themes emerged from the analysis including: ‘Confusion concerning involvement’, ‘The extra half patient’, and ‘Personal experience as a relative enhances empathy’. Each theme illustrates RNs’ experiences concerning our research questions aiming to illuminate neuroscience RNs’ comprehension of collaborating with and involving relatives (Table 3).
Themes.
Confusion concerning involvement
RNs describe very well the overall importance of cooperation and the involvement of relatives. But as they elaborate on the subject an interesting detail emerges. The theme ‘Confusion concerning involvement’ expresses the degree of relative involvement that takes place in clinical practice. A key finding is that RNs seem to confuse information with involvement. It became clear in the analysis that the RNs comprehension of involvement is when the relatives ask questions and the RNs respond with an answer; in other words, when they provide information to the relatives. This was primarily information concerning how the operation proceeded or how the patient's day has been. None of the RNs mentioned that they asked questions concerning the needs and preferences of the relatives or asked how the relatives preferred to be involved from a distance. Few RNs referred to the situation of relatives who customarily take care of the patient at home and the changed situation for these relatives during the patient's hospitalization. This could indicate that the involvement of relatives as intended is not understood by the RNs and therefore not interpreted as one of their key tasks and put into practice. One RN described the fine line between taking away verses relieving relatives of daily tasks with patient care. For the most part, it is not a new situation for them that their relative/the person who is hospitalized needs help with various things. So, if there is e.g. a spouse, I always ask how they do it at home. Have you helped him or her to the bathroom in the past? How do you feel about doing this during hospitalization? They can just answer yes or no, so they are free to choose whatever they want to help with. (Neurosurgery nurse, 28 years)
RNs consider involvement as the repetition of information regarding the daily routines and the doctor's round. The RNs also emphasize that collaboration with relatives involves recognition of and a holistic understanding of the relatives’ situation. Maintaining a good and trusting collaboration also requires consistent open and honest dialogue. Further, the RNs need to recognize the relatives’ need for information and that it often demands an initiative from the RNs: Most of the time, at least, I try to give it [information] a little in advance by calling them [the relatives] myself. I do this by asking the patient, whether I should call his wife or who they want me to call after the ward round. (Neurosurgery nurse, 28 years)
The extra half patient
The theme ‘the extra half patient’ describes collaboration with and involvement of relatives as being double-sided. On the one hand, RNs perceived that collaboration with, and involvement of relatives is necessary as part of a patient's hospitalization and also part of the nursing profession. On the other hand, collaboration with relatives is a part of nursing practice that may be given less priority when time is running short because it is considered time-consuming and as taking away time from their primary task (the patients), as an RN explains in the following quotation: I wouldn't call the relatives a burden, but it is easier, with them not being around. I have more time for my patients. (Neurological nurse, 35 years)
Thus, it may seem that no time or work resources are allocated to the involvement of relatives, despite the desirability of this taking place in clinical practice. Conversely, collaboration with relatives can also free resources which can be beneficial when the relatives reduce the RNs’ workload through their involvement.
Furthermore, most of the RNs agreed that relatives can be both a resource for them and the patient, but they also experience some relatives as a drain on resources.
One RN explained relatives as a resource: Relatives are a great resource in our ward and for our patients. The relatives know the patient best, what the patient likes/dislikes, or what we should be aware of. I believe that it is one of our key tasks to utilize them and talk with them because the relatives are important to us and the patients. (Neuro-rehabilitation nurse, 32 years)
Another RN explains why she considers relatives as a resource when they can help with nursing tasks. This is for practical reasons as it releases time for the nurse to carry out other tasks and take care of other patients: Relatives are a resource for the patient and us. They are a resource when they can assist with food and drinks when it is safe for the patient. In that way, they take some of the burdens for us. (Neuro-rehabilitation nurse, 33 years)
The quotation illustrates that relatives are considered to play an important role in the patients’ hospitalization but are not necessarily seen in this role in nursing practice. In the following quotation, one nurse reflects upon the involvement and how relatives on the one hand are considered as a drain on resources whilst, on the other hand, they are considered a resource for the patient's best. Many relatives are involved and want to know what is happening and be a part of the doctor's round. Some of them are fairly involved and that is nice, but it also means that you have an extra half patient to take care of and follow-up on concerning the ward round and what has been said. It is really good for the patients that more people are listening. (Neurological nurse, 35 years)
This quotation illustrates that the extra half patient can be given lower priority. On one hand, the ‘extra’ indicates that the relative is an addition to the admitted patient in need of care. On the other hand, RNs comprehend the relative as a ‘patient’ that needs to be cared for, in addition to the need to be informed about the patient's condition and prognosis. Thus, the collaboration can be regarded as a balancing act in which the RNs first and foremost must have the patient's care needs in focus, but at the same time must try to meet the relative's needs. In this way, it is a recognition that both relatives and patients are part of the patient's disease and treatment trajectory, and that time must be prioritized for both.
Another finding was that if the relatives are in too much crisis or are too demanding (e.g. asking too many questions), it can be a challenge involving the relatives, and it can have the consequence that they are requested to take a break away from the patient and even away from the hospital ward: Sometimes I have to tell the relatives ‘you need to leave the room now and go get a cup of coffee’. It may cross the boundary because it conflicts with the relatives’ wishes but we have to set limits. (Neurosurgery nurse, 28 years)
Personal experience as a relative enhances empathy
The RNs’ experience, personal as well as professional, seemed to affect their ability to empathize with relatives. The following example illustrates this point: … I have tried it myself; my father got ill and was taken to the hospital by ambulance and I was left behind without being able to do anything. So, I felt this powerlessness and uncertainty. What was happening with him and where could I get information? The lack of information has been the most frustrating for me, and then I have thought what about our relatives, the patients’ relatives? They experience the same. So the fact that I have been in their situation, has provided me with a greater understanding of the involvement of relatives and the importance of involving them in the patient's hospitalization. (Neurological nurse, 27 years)
The quotation illustrates how the nurse uses her own experience to help her to understand the relatives’ situation. The RN’s (personal) experience seems to increase the understanding of the relatives’ perspective, including the importance of and need for involvement and thus, of practicing nursing care that promotes involvement and collaboration with the relatives. This was explained by the RNs as keeping positive and providing encouragement through conversation and giving a little bit of themselves, letting the relatives know that the RNs are emphatic and human beings.
A rehabilitation nurse exemplifies how she reflects upon relatives’ needs and preferences concerning her wants and needs if she was a relative herself: What would I, as a relative, benefit from? They would not need to call me if they had stopped giving a vitamin pill, but would I prefer to be informed myself? I often do that when I am at work. Try to turn it around and reflect upon, what I would prefer. (Neuro-rehabilitation nurse, 32 years)
In addition, an RN expressed that the relatives’ characteristics and prior experience of healthcare environments influence the level of involvement and the way the relatives relate to the RNs: Sometimes it may be affected by a bad experience in the past, which sharpens their attention about what is happening around the patient, and whether they have expectations of and perhaps also an idea of what can be done if you claim your right to some extent. (Neurosurgery nurse, 26 years)
RNs’ understanding of relatives’ situations means that they more frequently start a conversation and in general are more aware of the importance of being the one initiating the dialog.
In summary, the theme ‘Personal experience as a relative enhances empathy’ relates to caring for relatives, as an individual attribute, and a basic human trait. The understanding of relatives’ needs for involvement seems to be influenced by individual judgment based on personal experiences, rather than professional judgment.
Discussion
Our study aimed to illuminate neuroscience RNs’ comprehension of the collaboration with and involvement of relatives. The findings revealed that the RNs’ understanding of these topics had three themes: ‘Confusion concerning involvement’, ‘The extra half patient’, and ‘Personal experience as a relative enhances empathy’. Findings from the study illustrate that if RNs do not recognize the establishment of a trusting relationship with the relatives as a key task, they may not engage themselves in involving the relatives and thereby risk regarding them as a drain on resources.
Having personal experience as a relative, having the required time and the ability to provide nursing care seem to make it easier to strengthen the relationship between RNs and relatives. The healthcare system in Denmark has in recent years had an increased focus on user involvement, first and foremost involvement of patients, but also the involvement of relatives, with the patient's consent. Guidelines have emerged as a result of this focus, presenting an ideal as to what involvement is and how to achieve it. As an example, relatives are expected to be active, knowledgeable, competent, and supportive and be able to navigate the healthcare system. 21 Findings from our study show that this ideal is not necessarily what is practiced and that the intended ideal of involvement does not seem to be present in current practice and nursing routines. This could be because there are competing policies focusing on cost-efficacy, transparency and accountability goals, as these factors affect the way RNs can practice their profession. 22 In this way, involvement can be seen as a theoretical construct or a discursive ideal rather than a practice that is extended beyond information to patients and relatives. There is nothing in the empirical data that suggests that RNs have a disrespectful attitude or behavior; the data imply that the RNs have a positive attitude and a genuine intention and willingness to involve the relatives, in addition to social skills where they meet the relatives with empathy. However, it appears that RNs’ attitudes may not be congruent with their actions and behaviors. Even though RNs find involvement important, lack of time seems to be a hindering factor for involvement. This is in alignment with another study illustrating that RNs struggle to involve patients and relatives within the frame of their work and organization 23 and in addition, there might be confusion around expectations and roles. 23
In our findings, it was evident that RNs’ comprehension of involvement was confused with information. This indicates that involvement is something RNs consider having taken place when they have informed the relatives. With this understanding, the RNs fulfill their obligations, but not in a way that empowers the involvement of relatives. When our findings also indicate that involvement seems to be a theoretical construct rather than a practice, there is something to suggest that it is the RNs’ understanding and attitude, and thus their behavior concerning involvement, that may confound the involvement of relatives. There is a need to address the fact that RNs emphasize time (and other contextual factors) as a barrier to the involvement of relatives because it does not align with routines and rigid organization. There is no doubt that time is a necessary factor to discuss in all relational work because time is spent both on treatment, nursing, interaction with patients and families, tasks, and documentation, but it can also be an excuse for not involving patients and relatives. 24 However, not using time for relational nursing care may be time-consuming in the long run as well as being inhuman nursing care. It, therefore, seems very important that RNs understand the rationale behind involvement, that it is more than just information, and that it benefits both the relative and the patient and is also is in the interest of the RNs.
Our study points to the fact that RNs mostly see relatives as a resource, but also that they associate involvement with an increased workload that takes time away from their primary task, the patient. This is in alignment with a Swedish study that found that relatives were seen as a resource, although demanding, challenging the RNs’ communication skills, taking up much of their time, and trying their patience. 25 Thus, involvement of relatives is not seen as releasing time or reducing the number of tasks in the RNs’ daily workload. This could potentially put the RNs under pressure, meaning that the involvement of relatives only happens when the nurse finds it relevant and helpful or if the relatives themselves request involvement and partnership. One study from 2013 showed that involvement of relatives may be challenged if meetings with the RNs are short, interrupted, or rare. 26 Relatives have different circumstances, opportunities, and needs for being involved in nursing care and treatment. Studies illustrate that patients and relatives, on the one hand, need to help society by taking responsibility for their health and in that way become an asset for the healthcare system and the RNs. On the other hand, if relatives are too proactive, asking too many questions, being too demanding, critical, or taking up too much time, it might result in them being excluded from involvement in the patients’ hospitalization. 21 When relatives are considered resource-demanding, it could be due to the RNs not being able to establish a relationship with the relatives. This can be due to the RNs’ experience (individual and work experience) or contextual factors. The establishment of a relationship with the relatives was perhaps even more difficult during the COVID-19 pandemic. However, if the RNs can empathize with the relatives’ situation, recognizing that it can be hard for them to identify how they could, or would like to, be supported during this time, it can be a way to establish a person-oriented relationship and potentially benefit the patient. Thus, collaboration with and involvement of relatives needs to evolve from an equal, mutual, safe, and trusting relationship with the RNs and needs to be recognized as a part of providing a holistic approach to care, recognizing that the patient is a part of a family. RNs need to engage with their professional expertise and involve the relatives’ expertise, for the benefit of patients with neurological diseases, who might have problems with being involved due to cognitive difficulties. The degree and success of the collaboration and involvement between the nurse and the relatives depend both on the nurse as an individual, and also on the relative as an individual and their previous experience of, e.g. dealing with the disease. It is expected that by building a trusting relationship with the relatives as a basis for involvement would result in more satisfied relatives.25,26 It, therefore, seems necessary to develop an intervention that ensures a systematic mapping of the individual relative's needs and preferences and ensures that the collaboration is not dependent on the individual nurse's competencies or wishes.
Strengths and limitations
The methodological rigor of this study rests on the trustworthiness of four quality criteria as suggested by Lincoln 27 dependability, credibility, confirmability, and transferability. Dependability was assured by having a stable research design, data collection, and data analysis. The research process involved the entire research group, from the development of research questions, interview guide, transcription of data, analysis, and discussion of findings. Credibility was assured by sharing data within the research group and by analyzing the data and reaching an agreement on themes and findings together. Confirmability was assured as data were checked and rechecked throughout the data collection and analysis process by all three researchers. Confirmability was also ensured by including different RNs working in different fields of neurological diseases (surgical, medical and rehabilitation). Finally, transferability was assured by providing contextual data and information about the included RNs.
This study also has some limitations. The first concerns the design of the study and the fact that this study only focused on the perspective of RNs. It could be relevant to illuminate the perspective from both patients and relatives to nuance the findings. A second limitation is related to the participants and the fact that we only included female RNs. However, the majority of RNs in Denmark are women and thus the sample could be argued to be representative of the population. The third limitation is related to the data collection and the timing of the interviews during the COVID-19 pandemic. RNs’ views on the collaboration with and involvement of relatives could potentially have been influenced by their concerns about how to protect themselves and others from COVID-19, lack of personal protective equipment, and changing guidelines. Lastly, a potential limitation of our study concerns the fact that all three researchers interviewed separately. The three researchers did have experience conducting qualitative interviews. However, as we are different persons and after all have different interview experience and technique, this might have resulted in variation of the quality of data collection. However, due to the common analysis process we believe that these variations have no effect on our findings.
Conclusion
Based on 19 interviews with RNs working within the field of neurological disease, we conclude that the establishment of a trusting relationship with the relatives is of the utmost importance for an experience of collaboration and for being able to involve relatives from the perspective of the RNs. Lack of structure including guidelines, leadership, lack of time, and conservative estimates of staffing needs are all contextual factors that can have an impact on the establishment of a trusting relationship, and the way RNs can provide nursing care based on trust, hope, respect, humanity, and compassion. Further, there seem to be other barriers to the involvement of relatives. One of them is the nurse's ability to use her own life experience to establish a relationship with relatives and how to use this relationship to act in the best possible way concerning the relatives’ wishes and wants. Moreover, involvement seems to be an ideological concept, since RNs confuse it with information. Thus, involvement as intended does not seem to be understood correctly by RNs. Finally, findings reveal how some RNs perceive relatives as a resource, while others perceive them as making demands on resources. Further research is needed to elaborate on the underlying causes.
Footnotes
Special thanks are due to all the nurses for their important contribution to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.