
Abstract
Educational models that facilitate an increased number of students while maintaining clinical education of good quality are needed. This discussion paper presents how peer learning was implemented in a geriatric hospital setting allowing for an increase in student numbers. Conclusively, a stringent implementation of peer learning facilitated an effective way of using existing supervision resources, while maintaining a good quality of clinical education. It is also important that the process is anchored in both educational and clinical settings with a clear division of responsibilities. Finally, all collaborative partners need to acknowledge the significance of high-quality clinical education.
Introduction
The goal of nursing education is to assure that bachelor’s nursing students (BNS) have the appropriate knowledge and skills needed for the nursing profession after completing their studies. It also includes competence in critical thinking, problem solving, communication, leadership, and utilization of research in practice. The care of today and of tomorrow places high demands on well-educated and competent nurses, who, in a patient-safe manner, can meet patients’ complex care needs in a demanding work environment 1 with limited resources. In Sweden, as in other countries, the shortage of registered nurses (RNs) leads to problems such as increased stress for RNs, decreased number of hospital beds and prolonged healthcare queues. 2 As a response, the Swedish government has given directives to the universities to increase the number of students admitted to bachelor’s nursing education programmes. At the same time, the reduction in hospital beds and RN turnover means difficulties in achieving clinical education, securing sufficient qualified preceptors and authentic learning situations for nursing students.2–4 Educational models that allow an increased number of students while maintaining good quality of clinical education and safe patient care must therefore be developed and tested. 5 This challenge is important for both the universities and future employers, and requires collaboration. This paper discusses such a collaboration by presenting how peer learning was implemented in a geriatric hospital setting, allowing for an increase in student numbers.
Setting
The basis for the collaboration project was a clinical supervision model used by Karlstad University and the County Council of Värmland for around 20 years. 6 At the university, 202 bachelor’s nursing students are admitted annually to a three-year under graduate programme. During the programme, all nursing students participate in nine different clinical placements ranging from two to five weeks in primary healthcare, community care as well as in hospital-based surgical, medical/geriatric and psychiatric care. The model is based on person-centred care and implies that the BNS follows the patients rather than the preceptors, thus it is called ‘person-centred supervision’. Students are expected to provide the care for their patients within their scope of practice, including clinical documentation and patient handover. Conclusively, the RN responsible for the patients’ care is also the preceptor for the day and supervises the students during the daily bedside nursing, including reflection, feedback, and evaluation. A main preceptor, with a master’s degree in nursing, has an overall responsibility for the BNS’ clinical placements in cooperation with a clinical nurse lecturer (employed by the university). Together with the BNS they plan and follow up the students’ clinical practice. The main preceptor’s role also includes bedside supervision at least once a week with regard to the curriculum learning outcomes. Further, they are supporting colleagues in their roles as daily preceptors, taking part in assessments of BNS and in formal meetings about clinical education with the university.
Meeting the challenge
As a response to the demand for an increasing number of clinical placements to cater for larger student cohorts we introduced the peer learning educational model as a possible solution3,5,7,8 to the county council in the autumn of 2016. Peer learning is described as learning by interaction between equals, i.e. students from the same level of education learn from and with each other by actively seeking knowledge, problematizing and reflecting on different learning situations. 7 Students who share a common learning experience gain an increased sense of security and understanding of the context, as well as increased opportunities for development of knowledge and skills. The model had shown promising results for student learning in clinical education3,7,8 and in terms of preceptors’ experiences of supervision.3,9 Following decisions made at management level, we started a collaborative project regarding peer learning in the second year of bachelor’s nursing studies during two periods of clinical placements as a means to double the number of students.
Planning the project
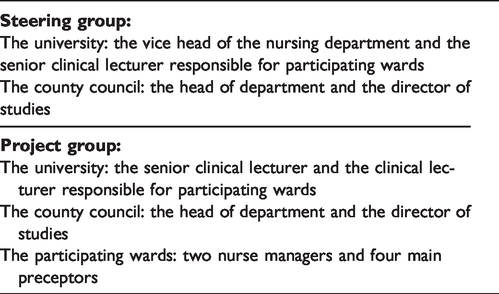
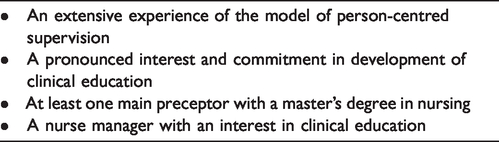
First, in an effort to secure management support, we created a steering group consisting of key persons from the university and the county council (Table 1). We constructed a project plan based on strict quality requirements for wards eligible for the implementation (Table 2) and two geriatric hospital wards fulfilled all the criteria and were thus included in the project.
Participants in steering group and project group.
Quality requirements for wards eligible for the implementation.
Second, we formed a project group (Table 1). During February to August 2017 the group had monthly meetings to agree how to organize the project. We planned thoroughly for 1) redoubling the number of BNS using peer learning (from four to eight BNS in the same ward), 2) revision and production of regulatory documents, and 3) introduction of the project structure and peer learning educational model to RNs and assistant nurses via workplace meetings and a one day launch. We planned for two ways of organizing the students as peers; one group of four BNS had the same peer throughout the whole period of clinical placement (five weeks), and the other group of four BNS changed peer every week. In total, 24 students participated during the implementation. The agreement between the university and the county council gives each main preceptor allocated time with students corresponding to four hours per student a week. Within the project the university provided the main preceptors with an extra 10 percent adding to the ordinary 50 percent of fulltime (38.25 hours work time per week) for supervision of students and support to precepting colleagues. Moreover, a structure for how we wanted to introduce the students to peer learning on their first day of clinical education was developed. The guidelines for the clinical supervision model were updated to reflect the peer learning pedagogical model and included instructions for reflective dialogue according to Gibbs. 10 The launch constituted of one full day for all personnel on both wards. The day started with a lecture in peer learning by the clinical lecturer and the senior clinical lecturer. This was followed by the main preceptors presenting the organizational structure of peer learning supervision. We also clarified the main preceptors’ mandate of organizing the BNS’ and the daily preceptors’ schedules in accordance with peer learning and person-centred care, which was a significant change in relation to the ordinary routines on the wards. The project required a clear structure where the BNS were scheduled as peers four day and evening shifts/week. Changes to these strict schedules were only permitted in extraordinary circumstances and approved by the main preceptor. Finally, all personnel discussed opportunities and challenges with peer learning and the increased number of BNS. Problems identified during the launch were managed and plans drawn up for solutions, i.e. purchase of additional computers and a strict time schedule for lunch break. This prepared the organization for as many aspects of the project as possible.
Third, we planned for evaluation and feedback carried out by BNS, main preceptors and daily preceptors with collection of both qualitative data and quantitative data, which will be reported in a future publication.
Peer learning appears to be a good solution
On the basis of our experiences of the process it seems that the implementation of peer learning allows for maintaining quality of clinical education whilst redoubling the number of students. One concern when we started the project was how the patients would react to the increased number of students. However, our tentative evaluation indicates that the preceptors experienced that peer learning facilitated, and to some extent increased, continuity and patient participation, both core parts of person-centred care. 11 This can be explained by the fact that the students cared for a limited number of patients, enabling the students to spend quite a lot of time with the patients.
We were also concerned that the main preceptors’ workload would be too high. Consequently, two main preceptors with competence in nursing and supervision were assigned to each ward. Because the wards had a large proportion of inexperienced preceptors, the main preceptors were sometimes scheduled as daily preceptors in order to secure the quality of clinical education. The structured scheduling and the strict planning were necessary for the implementation even though it initially increased the workload for the main preceptors. However, by the second period of clinical placement of the project they benefitted from the thorough planning and in some parts reused it. For example, they used the same frame for rostering the second group of nursing students.
The full support from nurse managers who have a sincere interest in clinical education needs to be recognized. They created conditions for a good clinical learning environment for both BNS and personnel, which enabled increased numbers of students. This was also visualized by mandate and conditions for the main preceptors, i.e. time for supervision, support in scheduling, and facilitating development of competence in supervision, together with a positive and permissive climate towards students. The nurse managers strived to make the students feel welcome and as part of the team and they were regarded as future colleagues. This type of support is part of a transformational leadership, which has been proven to decrease turnover 12 and increase work commitment. The personal commitment of the main preceptors and the nurse managers is the key to a successful implementation but can also be a weak point if they change workplaces. To secure a sustainable model, the willingness to supervise students in peer learning needs to be inherent in the ward culture. Moreover, to reduce nurse turnover, main preceptorship should be regarded as a potential career path for nurses.
The ongoing evaluation indicates that a good learning environment is essential for BNS development of appropriate knowledge and skills needed for the profession. The students also perceived that not only the preceptors, but also the entire staff were aware of the structure of their clinical education, probably due to the one-day launch. This is in line with a previous study by Dale et al. 13 concluding that preceptor preparedness is an important part of a good learning environment as it creates a positive start to the students’ clinical education and strengthens motivation. In addition to the one-day launch, continuous pedagogical support from the university was provided throughout the whole process during staff meetings. It consisted of guidance on how to supervise, reflect and provide feedback in peer learning. This support was constructed from earlier experiences of preceptors expressing a need for introduction and aligned to a previous study by McClure and Black 14 showing that nurses are not always fully prepared for their role as preceptors.
Another concern was whether the peer learning pedagogical model prepared the individual students’ professional competence and skills. According to the peer learning model the BNS planned the care together with the patients, bounced ideas between themselves and then informed the preceptor about their intended actions before delivering care. This and continuous follow-up during the day enabled the preceptor to assess each student’s individual contribution to the planning and delivery of care.
To extend our understanding about peer learning we tried two ways of organizing the peers. BNS who changed peers every week seemed to be more satisfied than the students who had the same peer during the whole clinical placement. They more easily perceived their own and their peers’ professional development. Even in cases when they experienced challenges with peer learning, e.g. competition between peers and/or problems with collaboration as earlier described,7,9 the students found it easier to handle and try different solutions to facilitate cooperation, as they knew that the next week they would have a another peer. In this way they developed solutions to facilitate collaboration, which is also a valuable competence in professional nursing.
Since an understanding of each other’s prerequisites and responsibilities needed to be explicit, a sharp timeline and a distinct division of responsibilities as well as working in close collaboration were crucial for the implementation. The project group continued with monthly meetings during the implementation phase, where pedagogical and practical issues and responsibilities were discussed. Adjustments were made in collaboration, and when disagreement occurred participants referred to the regulatory documents for advice.
Conclusions
Conclusively, we suggest that a stringent application of the peer learning educational model created an opportunity for increasing the number of students as well as still supporting BNS’ opportunities to attain the learning outcomes for clinical education. The structure encouraged the students to be responsible for the care of patients, which seemed to create a more person-centred care in the wards with elderly patients often with complex nursing needs due to comorbidity. Although, we assume that to keep up the good quality in clinical education it is necessary that the preceptors and personnel should have student-free weeks to reflect on the learning environment and enable discussion about strategies for further improvements. Critical success factors seem to be: the process should be anchored in both the university and the county council organizations at all levels, a clear division of responsibilities and roles should exist, and all participants should have an interest in and commitment to supervising BNS. Another critical success factor is the competence of both main preceptors and daily preceptors which can pose a challenge to maintain due to staff turnover. To achieve a continuously adequate competence in these key persons the nurse manager needs to establish plans for competence development for both new employees as well as for nurses with inadequate supervision competence and no master’s degree in nursing. To keep up a good quality with this model, both organizations need to have perseverance and continuously perform follow-ups as well as repeatedly reintroduce the model. In a future paper, the experiences of the implementation from both students’ and preceptors’ perspectives will be described using a mixed-methods approach.
Footnotes
Acknowledgements
The authors would like to thank all the BNS, preceptors and staff in the participating wards. The County Council of Värmland is also appreciated for cooperation and the opportunity to carry out the project.
Author contributions
Study design and data collection: CO, EC, CSA and AJE; data analysis and manuscript preparation: CO, EC and AJE; and critical review of the manuscript: CO, AJE, EC and CSA. All authors approved the final manuscript.
Consent to publish
There are no details related to an individual within this manuscript. Presentations is on group level.
Conflict of interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The evaluation of the project was approved by the local ethical review board (Reg. no. C2017/831). All participants in the project have given written informed consent.
Funding
The implementation of the project was not funded. We acknowledge the generous funding for preparation of the manuscript from Alice Lindström scholarship, Swedish Society of Nursing.