
Abstract
The aim was to examine the impact on interpreters’ health knowledge, attitudes and self-evaluated skills after they participated in a pilot health introduction course at a university hospital in Denmark. The study was conducted as an intervention study using a questionnaire with both closed and open-ended questions. The questionnaire was distributed to interpreters one week before the six-week course started, and again at one week and at three months after course completion. Level of knowledge was calculated based on the number of answers to 18 multiple-choice questions on common health issues, diagnoses and treatments. Of the 100 interpreters who registered for the course, 86 completed the course, and 61 of these participants (70%) completed both the baseline and the one-week questionnaire. The mean knowledge score increased from 48 (SD 6.9) at baseline to 52 (SD 3.4; p < 0.001) one week after the course and was 51 (SD 7.3; p < 0.001) three months after the course (n = 55). Participants who increased their knowledge score the most were those with the least interpreter experience (p = 0.001). One week after the course, most participants (83–95%) agreed that the individual lessons had been useful in their subsequent interpreting activities and that they had gained useful information. The health introduction course appeared to be beneficial for interpreters. This study highlights the need for greater focus on education for interpreters working in the healthcare sector.
Introduction
The number of migrants and their descendants has increased in Denmark over the last 30 years, and in 2018, 13% of the Danish population were migrants or descendants of migrants. 1 More than 200 countries of origin are represented, and migrants thus speak a variety of languages and dialects. 1 As language helps to describe and shape the experiences of the patient, 2 it is essential that there is a common understanding of principal concepts such as illness, pain, grief and healing. 3 Interpreters’ skills and knowledge regarding language, ethics and confidentiality vary considerably. 4 Ad hoc interpreters such as family members and friends are often used in the healthcare sector, 5 with potentially negative consequences for both the patient and the family interpreter. 6 , 7 Nevertheless, the use of professional medical interpreters is low in many clinical settings.8–10
Both international 11 , 12 and Danish studies 13 have documented the need to acknowledge the interpreter as a staff resource and a potentially powerful mediator between the patient’s personal experience and the health professional’s knowledge. Use of professional interpreters rather than untrained interpreters can significantly reduce medical errors 10 , 14 and may increase the quality of care given to patients with limited English proficiency. 15 A Japanese study found that a three-day training program (20 hours) for medical interpreters could help bridge the gap between health professionals and patients, 16 while an American volunteer medical interpreter education program (80 hours of training) increased interpreters’ skills, knowledge and confidence. 17 An American study comparing the accuracy of translation using professional interpreters, ad hoc interpreters and no interpreter found that hours of interpreter training – but not years of experience – were significantly associated with the number of errors, where those with more training made fewer errors in translating health issues for patients and health professionals. 9 A recent systematic review examining the cost-effectiveness of using professional interpreters indicated improved medical care for patients and either limited additional costs or cost savings. 18
Denmark does not have an official education or certified program for interpreters, 19 and the current law states that it is the treating doctor who has to ensure that the interpreter has the necessary language qualifications. 20 Many interpreters lack knowledge about health terminology and the Danish healthcare system, which has consequences for patients in the form of misunderstandings, mistreatments and in terms of patient safety. 4 , 19 Currently, interpreters acquire their knowledge mainly from lessons taught by external educators at interpreter agencies. 19
The aim of this study was to examine the impact on interpreters’ knowledge and skills after they participated in a health introduction course in a hospital setting. The specific objectives were to assess 1) changes in interpreters’ health knowledge scores, 2) changes in interpreters’ attitudes to interpreting and self-evaluated skills, and 3) their satisfaction with the course. The underlying goal was to reduce inequality in care for patients with language barriers.
Data and methods
Design
This study was conducted as an intervention study using a questionnaire consisting of both closed and open-ended questions. The self-completed questionnaire was used to investigate interpreters’ health knowledge and self-evaluated attitudes and skills one week before, and one week and three months after a pilot health introduction course.
Study participants
Inclusion criteria for the study were interpreters working in the healthcare sector (i.e. hospitals, general practice, and community care) and preferably in the Region of Southern Denmark. To reach as many interpreters as possible, participants were recruited via social media (e.g. Facebook, Twitter) and the region’s webpages. Interpreters who had already participated in the health introduction course were asked to inform their colleagues about the course. Interpreters working only with the police force or legal system were excluded.
The intervention: the health introduction course
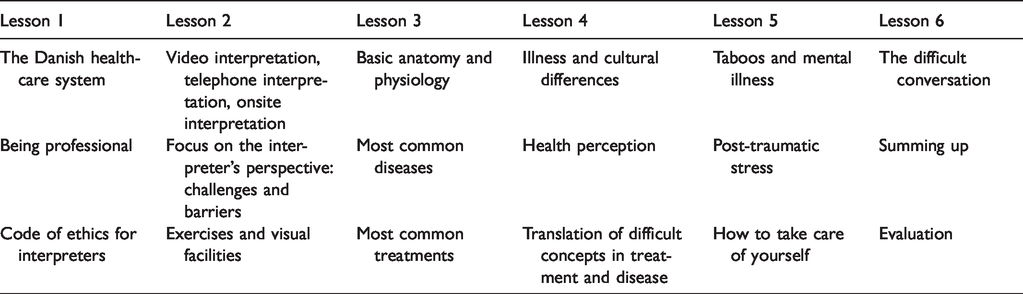
The course was developed by staff working in a migrant health clinic who had over 10 years of experience in transcultural clinical care and treatment. Medical specialists from a trauma rehabilitation department also contributed to the course content. The courses were planned to run for a period of one year and were free of charge. A course lasted six days, each with three lessons, which were held once a week over six weeks. Each course was attended by 10 to 15 interpreters. Table 1 shows the content of the 18 lessons.
Content of the six lessons.
The questionnaire
A questionnaire was developed to evaluate the different aspects of the health introduction course. A group of five specialists (doctors, nurses and social workers) who worked at a migrant health clinic and had many years’ experience of working with interpreters produced a first draft of approximately 100 questions. After further review by the group and other staff at the migrant health clinic, about half the questions were moved due to overlapping and low relevance. The questionnaire now consisted of four sections: demographic information, knowledge about health issues, attitudes and self-evaluated skills, and (for the follow-up questionnaires) an evaluation of the course.
The questionnaire was tested in a face-to-face validation exercise with ten experienced interpreters, who completed the questionnaire and then discussed each question in turn. This resulted in re-wording of some questions and the addition of four questions to the knowledge section. The final baseline questionnaire consisted of 54 questions, and the follow-up questionnaires consisted of 57 questions.
The baseline questionnaire began with 11 items on demographic information and two questions about other interpretation courses. The section on health knowledge comprised 18 multiple-choice questions to test knowledge about health issues, diagnoses and treatments, e.g. post-traumatic stress disorder, cancer, and stroke. Then followed 23 items on attitudes and self-evaluated skills, each answered on a four-point scale: Agree, Neither agree nor disagree, Disagree, or Do not know. These items focused on ethics, handling conflicts, caring for patients and patient confidentiality. The follow-up questionnaires had two additional open-ended questions regarding the interpreter’s overall experience with the course and 10 closed questions about specific aspects of the health introduction course. The questionnaire in Danish is available on request.
Data collection
The questionnaires were distributed via email to interpreters who participated in the health introduction course. The questionnaire was sent out one week prior to the course and again one week and three months after they had completed the introduction course. Non-responders were sent three reminders. The first two reminders were automated emails, and the last was a phone call (or a text message and email if the interpreter could not be reached).
The data were handled in REDCap in collaboration with Odense Patient data Explorative Network (OPEN). 21 To test the online system, the questionnaire was first distributed to the ten interpreters who attended a trial course (these data were not included in the analysis).
Analysis of data
No power calculation was conducted as we intended to invite and include as many interpreters as possible within one year. Baseline characteristics and satisfaction with the course are reported as counts and proportions. A ‘knowledge score’ ranging from 0 to 56 points was derived for each respondent at each time point by assigning 1 point for each correct answer to the 18 items on health knowledge. Another point was allocated for each incorrect answer that was not marked. No points were allocated if the response choice ‘Do not know’ was marked. Knowledge scores are reported as means with standard deviations. Due to the non-normality of the scores, changes between time points were analyzed using the non-parametric Wilcoxon sign-rank test for repeated measurements from a single sample.
The 23 items on attitudes and self-evaluated skills were treated as categorical variables. Due to the low frequency counts of some response options, the answers at baseline and at three-month follow-up were compared using Fisher’s exact test. This test takes into account the changes for individual participants and is more accurate than a chi-squared test in small samples. Significant changes in individual responses may not be reflected in the overall answer distribution if some participants’ attitudes change in one direction and others’ change in the opposite direction. Significance level was set at p < 0.05.
Satisfaction with the course was further investigated by using thematic analysis to analyze the interpreters’ responses to open-ended questions. 22 All open-ended answers were collected in one document, and different themes were identified via coding. A theme was understood as a set of replies that could be grouped because they were part of the same topic, even if they were worded differently.
Ethics
The Danish Protection Agency 17/45557 approved the study, and all data were handled and stored according to Danish laws on data protection and confidentiality. Participants were informed that participation in the survey was voluntary and that by completing the questionnaire, they gave their consent for their data to be analyzed. It was emphasized that their questionnaire responses would be anonymized and that participation or not in the questionnaire study had no impact on their conditions of employment.
Results
Of the 100 interpreters who registered for the health introduction course, 86 completed the course between January 2018 and January 2019. Of these, 68 (78%) completed the baseline questionnaire, 61 (70%) completed the questionnaire one week after course completion, and 55 (63%) completed the questionnaire three months after course completion (Figure 1).
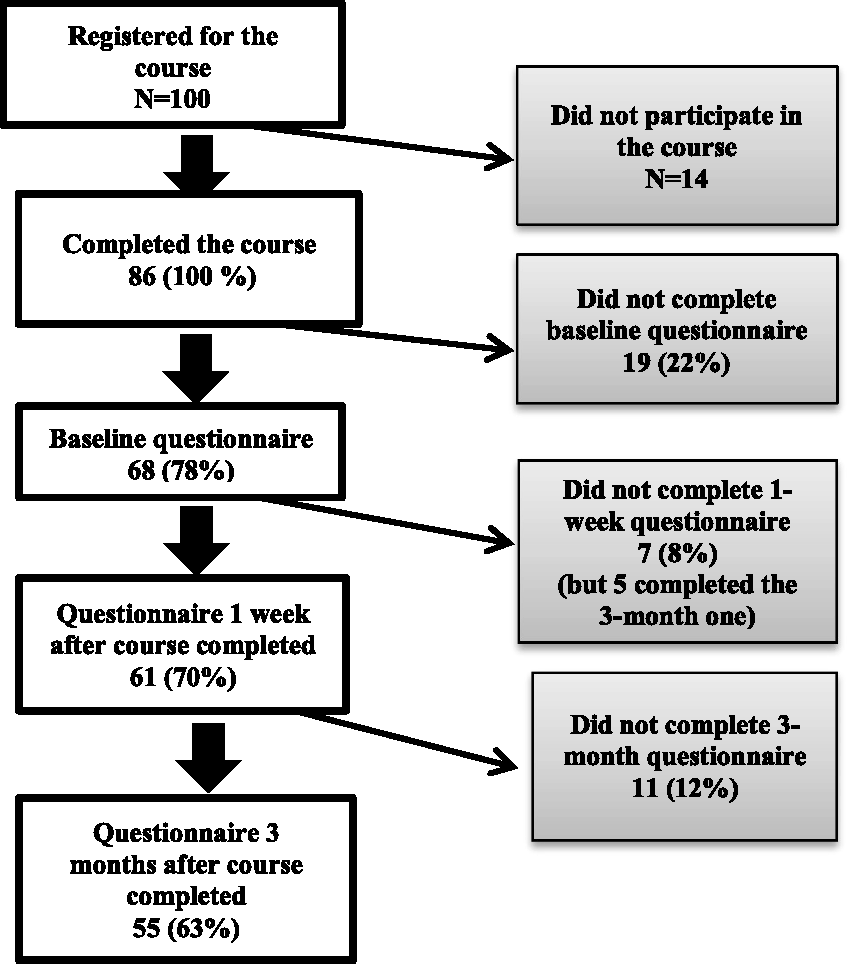
Overview of questionnaire completion by 100 interpreters who registered for the health introduction course.
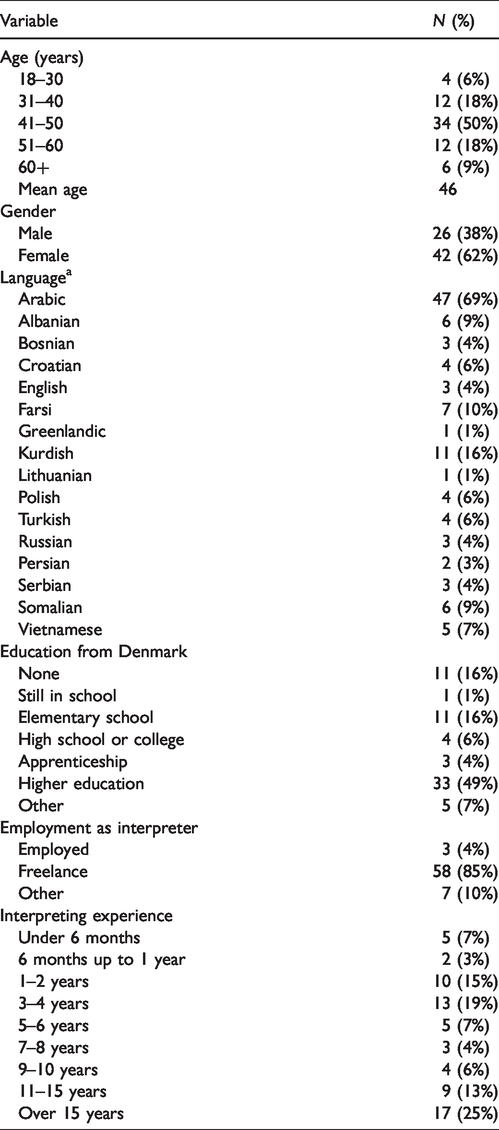
The interpreters who completed the questionnaires (hereafter referred to as study ‘participants’) were aged 24–69 years with a mean age of 46 years, and 62% were women (Table 2). They came from a range of countries and most spoke Arabic (69%), Kurdish (16%), and/or Farsi (12%). While their experience as interpreters ranged from under 6 months to over 15 years, 26 (38%) had over 10 years of experience whereas only seven (10%) had less than one year. They were highly educated, with most (84%) being educated in Denmark, and 49% had a higher education. Most (85%) were employed on a freelance basis. None of the interpreters had a formal interpreter education, but most had participated in short informal courses arranged by private companies.
Demographic data for the 68 interpreters who completed the baseline questionnaire before the start of the health introduction course.
The participants’ knowledge scores
The mean knowledge score at baseline was 48 (SD 6.9). One participant with 19 years of experience scored the maximum of 56 points, and the lowest score was 16 points (one participant). One week after course completion, the minimum score had increased to 38 (one participant) and the mean score to 52 (SD 3.4). The three (5%) participants who scored maximum points had from five years to over 15 years of experience. Three months after course completion, the minimum score had fallen to 16 (two participants), and the mean score was 51 (SD 7.3). The seven (13%) participants who scored maximum points had from one year to over 15 years of experience.
The participants significantly (p < 0.001) increased their knowledge score from baseline to one week after completion of the introduction course, corresponding to a mean increase of 3.7 points (95% CI 2.2 to 5.2 points). The same was found from baseline to three months after completion of the introduction course (p = 0.0003). There was no significant difference (p = 0.461) in knowledge scores from one week to three months after course completion.
The number of years of interpreter experience was significantly associated with knowledge score at baseline (p < 0.001) and at three months after course completion (p = 0.021). Participants who increased their knowledge score the most were those with the least interpreter experience (p = 0.001), where extra improvement of knowledge score for each year of experience was –0.70 (95% CI –1.11; –0.30) points. Participants with fewer than two years of experience increased their score by an average of 6–7 points.
At the three-month follow-up, the mean age was 40.9 years of age; 75% were women, and 56 (82%) were freelancers. Participants with over 15 years of experience only increased their knowledge score by an average of 1.5 points. Compared to baseline, the average score for women increased by 3 points and that for men by 3.7 points, but this was not a significant difference (p = 0.596; and p = 0.128 when adjusted for years of experience).
We found no association between age and knowledge score, i.e. older participants did not have a higher knowledge score than younger participants. Nor was there an association between level of education and knowledge score, and the participants with the highest education level did not score higher than the participants with no or lower education. We found no association between change in knowledge score and type of employment (freelance or employed).
Attitudes and self-evaluated skills
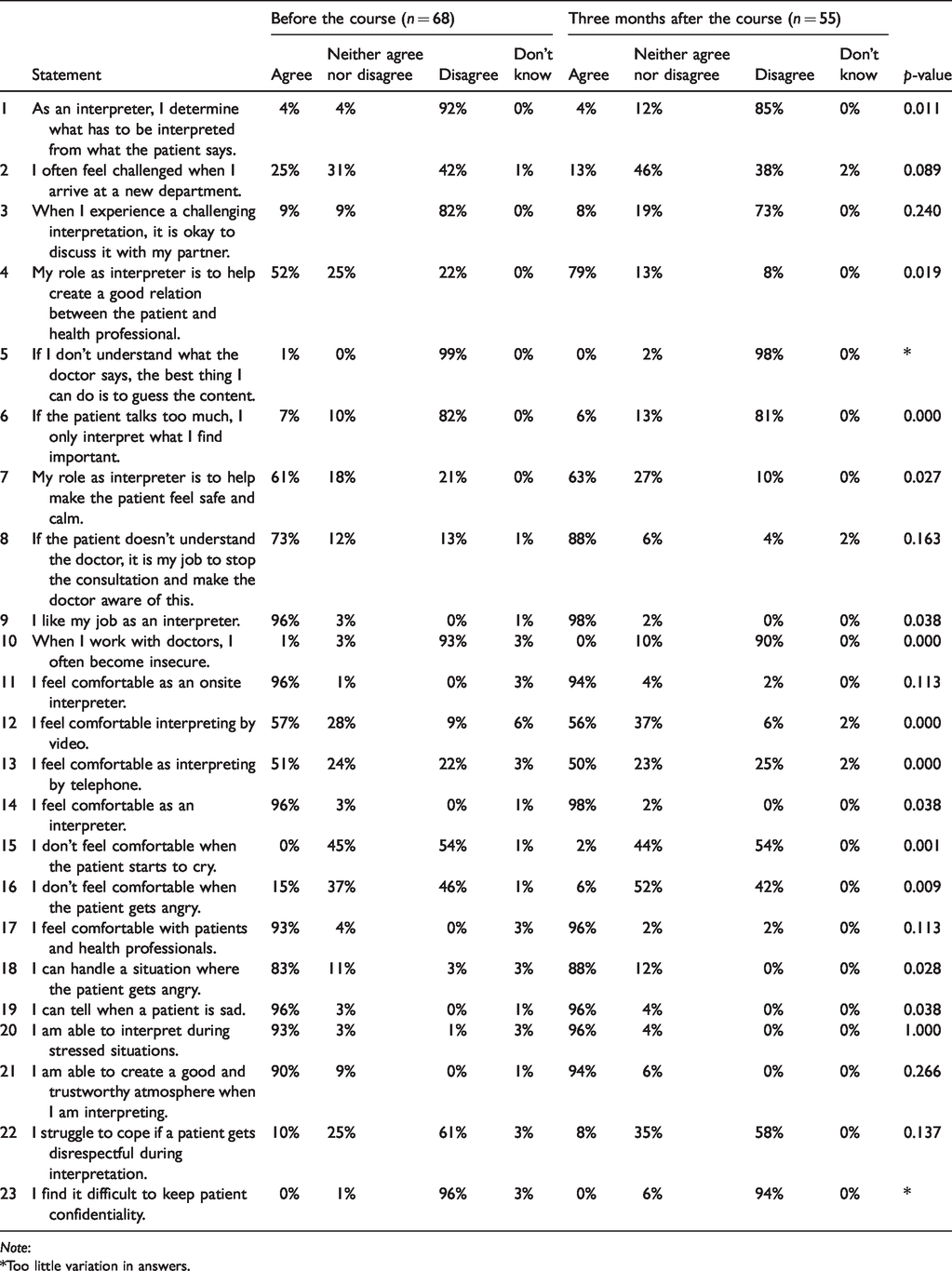
The participants were asked to express the degree to which they agreed or disagreed with 23 statements on attitudes and self-evaluated skills. The results at baseline and at three months after course completion are shown in Table 3. For 13 of the statements, the changes in the participant’s answers were statistically significant. For six further questions, no overall changes were apparent, indicating that some participants changed their attitudes in one direction and others in the opposite.
The participants’ attitudes and self-evaluated skills at baseline and at three months after completion of the health introduction course. Note that the p-values test for individual changes, hence the test can be significant even if some participants change in one direction and others in the opposite direction, resulting in similar answer distributions.
Note:
*Too little variation in answers.
At baseline, 52% of the participants agreed that their role as interpreters was to help create a good and trusting relation between the patient and health professionals. After participating in the course, almost 80% of them agreed with this statement (p = 0.019). Both before and after the course, most of the participants responded that they usually did not feel insecure while working with doctors, (p = 0.000). Before the course, 15% of the participants responded that they felt uncomfortable when a patient became angry while only 6% did so after the course. After the course, none of the participants felt that they lacked the competencies to handle a situation where a patient got angry (p = 0.028). In the open-ended questions, the participants commented that the course had taught them how to be more professional and how to deal with challenging situations, as well as having taught them about their rights as interpreters.
Satisfaction with the course
The participants expressed overall satisfaction with the health introduction course. One week after course completion, 56 out of 61 (92%) answered that they would recommend the course to other colleagues. The strongest argument was that participants felt they had learned about their rights as interpreters and how to handle complicated situations. They also reported that they had learned to be more decisive and to stand up for themselves, and they had obtained insight into illnesses and examinations. Most participants had been satisfied with the opportunity to meet other interpreters and share their experiences. Comments in the open-ended questions included: We as interpreters need a course in healthcare. A good and positive process where you can learn many things from both your colleagues and the professional team behind the course. The course gave me more structure in my work, handling patients, feeling that I am not alone – good networking.
Of the 61 participants who completed the questionnaire one week after course completion, between 83% and 95% (depending on the lesson) agreed that each lesson had been useful for their subsequent interpreting activities. Only 1–2 participants felt that the lessons had not been useful for their interpreting.
Discussion
We found that interpreters who participated in a questionnaire survey before and after attending a health introduction course had increased their knowledge score on health issues, diagnoses and treatments after the course. The greatest improvement in knowledge score was observed in participants with the least interpreter experience. Before and after the course, a higher knowledge score was associated with more years of experience with interpreting but not with the interpreter’s level of education. After the course, significantly more participants agreed that their role as interpreters was to help create a good and trusting relation between the patient and health professional and that they could handle a situation where the patient gets angry.
The health introduction course consisted of 18 hours of training in total. Although it appeared to increase the interpreters’ knowledge about health issues, this does not necessarily lead to a higher quality of interpreting. It is debatable whether such a short intervention can change interpreters’ habits and underlying attitudes to interpreting or improve patient safety. Ono et al. 16 used a randomized trial to test a three-day intervention comprising a total of 20 hours training for interpreters. They found that interpreters in the training group achieved a higher knowledge score than those in the control group. 16 Flores et al. 9 suggested that a requirement for interpreters to have at least 100 hours of training might be of major benefit to the quality of care and patient safety, while Hasbun et al. 17 showed that 80 hours of training increased the skills, knowledge and confidence of volunteer interpreters.
While most of our participants increased their knowledge score after participating in the health introduction course, those with the least interpreting experience increased their knowledge score the most. Itani et al. 4 also found that longer interpreting experience was associated with greater likelihood of having adequate language skills for effective communication. The open-ended questions in our project revealed that some of the experienced interpreters felt they did not gain new knowledge or skills from participating in the course, suggesting a need for an additional course aiming at a higher level of interpretation training. While our participants had a mixture of experience levels (from 0 to 19 years), a course like the current health introduction course appears most relevant to less experienced and newly started interpreters. We did not investigate, however, the effect of having more experienced and knowledgeable interpreters on the course. It is possible that they contributed to the others’ learning by sharing their own experiences and being able to discuss more difficult or sensitive topics.
After the course, we found that many participants had changed their attitudes regarding their role as an interpreter, especially when managing conflicts but also by having a clearer insight into their role. They reported being more aware of their role to build a bridge between the patient and the health professional and of their rights as interpreters. A Swedish study on professional interpreters’ experiences of healthcare encounters reported that interpreters sometimes found it difficult to manage their emotions after consultations that involved delivering bad news, diverse family situations and managing threatening patients. 23 At three months follow-up in our study, more interpreters reported they felt they had more competences in handling situations where the patient are angry or sad. This could further support a need for more training and supervision on how to handle emotional situations.
The high questionnaire response rate suggests that the participants were highly motivated to participate in the study. However, 13 potential participants did not attend the course after registering or only participated in the first lesson (mainly due to illness or unknown reasons). This highlights the advantage of offering such a course several times a year.
There are several limitations to our study. First, the recruitment approach meant that our participants were interpreters with a range of backgrounds and interpreting experience. This made it challenging to provide relevant teaching for all participants and to evaluate the level of learning. Study participants were interpreters who were interested in following a six-week health knowledge course, and they may differ from healthcare interpreters who are not interested in further education. Another limitation is that measuring participants’ health knowledge using self-completed questionnaires does not give a full picture of participants’ level of knowledge. 24 There are several possible biases connected to this methodology. Participants could have looked up the correct answers on the internet, for example, or could have asked friends or colleagues for help in completing the questionnaire. The relatively large number of questions may have deterred participants from proper consideration of their answers. Another limitation was the difficulty level of the heath knowledge items. Although knowledge scores showed a wide range (from 16 to the maximum 46), several participants had high scores already at baseline and we were unable to see any improvement after the course. This relates back to the desired level of training aimed for during the course and the desired level of knowledge to be attained.
This study has highlighted important issues for the training of health interpreters and helping them to develop adequate and relevant skills. The study results have been used to improve the health introduction course, which is now provided 3–4 times a year to newly employed health interpreters in the Region of Southern Denmark. However, we still lack more detailed knowledge about how individual interpreters can benefit from the course, and especially their experiences of interacting with colleagues and applying their knowledge and skills in their future work. Focus groups or individual interviews would be useful for this purpose.
Conclusion
Healthcare interpreters who participated in a questionnaire survey before and after attending a health introduction course showed improved knowledge on health issues, diagnoses and treatments after the course. These results highlight the need for greater focus on competencies and training for interpreters working in the healthcare sector. This is a prerequisite for equality in care and treatment for patients with language barriers.
Footnotes
Conflicts of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contributions
DSN, LSA and MSO: contributed to the conception and design of the work.
All authors: contributed to the acquisition, analysis, and interpretation of data for the work; drafted the work and revised it critically for important intellectual content; approved the final version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
We are very grateful for the funding provided by the Region of Southern Denmark, who supported us with a grant the first year of the study and to Østifterne [18-209] who supported the study with a grant the second year.
Acknowledgement
Thanks to Anders Valentin Johansen for proofreading the paper. We also thank Odense Patient data Explorative Network, OPEN, at University of Southern Denmark for assistance with storage of data, statistic supervision and with formalities regarding our research project.