
Abstract
Adherence to drug treatment is a multidimensional concept. It is affected by many factors, such as physiological, psychological, family, environmental and social conditions. However, relatively little is known about the relationship between adherence to medication and psychosocial adjustment. The aim was to explore the relationship between adherence to antidiabetic drugs and the psychosocial adjustment of patients with type 2 diabetes mellitus. This cross-sectional descriptive correlational study was conducted between March and June 2018. A convenience sample of participants was recruited from seven internal disease outpatient clinics at a public tertiary hospital, located in a large city that serves as a gateway to nearby rural and urban areas in the north-west region of Turkey. Data were collected using the Adherence to Refills and Medications Scale (ARMS-7), and the Psychosocial Adjustment to Illness Scale–Self Report (PAIS–SR). This study is reported in accordance with STROBE. Pearson’s correlation analysis found a significant weak positive correlation between all domains of the PAIS–SR and the total scores on the ARMS‐7. The participants’ scores on medication refill were found to be significantly and positively correlated with all of the PAIS–SR domain scores except the sexual relationships domain. Psychosocial care could play a crucial role in improving drug regimen adherence among patients with diabetes. Therefore, nurses should integrate psychosocial care into daily practice.
Introduction
Adherence to antidiabetic drugs is essential to ensure optimal glycemic control, which is a crucial treatment target for patients with type 2 diabetes. 1 Unfortunately, patients’ adherence to drug regimens in type 2 diabetes is inadequate both in Turkey and worldwide.1–6 Most studies have reported that the percentage of those not adhering to oral antidiabetic drug treatment is 44.5–71.0% in the USA, and 64.7% in Turkey. Similarly, the percentage of non-adherence to insulin treatment is 41% in the UK, 40% in Germany, 33% in China, and 24.0–40.4% in Turkey.1,4,6 In addition, one study found that 73% of patients do not refill their insulin prescriptions. 2 Non-adherence to drug treatment can lead to increased frequency of hospitalization and diabetes complications.1,4,6 Furthermore, poor adherence is predicted to be related to increased mortality. 1 Nurses need to improve medication adherence to prevent various negative health outcomes in the long term.
Adherence to drug treatment is a multidimensional concept. 7 Patients interact continuously with not only healthcare providers but also their family, social, and vocational environments during treatment.8,9 Patients and their adherence can be affected either positively or negatively by these environments.8,9 For example, family members’ unsupportive behaviors can have a negative effect on the treatment process. 10 Qualitative studies have shown that family members can hinder insulin treatment initiation because of misconceptions such as fear of addiction.12,14 They can also exacerbate the stresses related to the drug regime. 10 Conversely, family members’ supportive behaviors, such as helping inject insulin and renewing the prescription regularly, can facilitate medication adherence. 11 Thus, nurses need to identify the obstacles to and facilitators of adherence to medication regimens, to be able to plan effective education and monitoring programs.
Patients can experience a wide range of treatment-related stressors, such as fear of hypoglycemia, addiction concerns, and needle phobias, which can increase their psychological burden.8,9,12 Patients have also reported problems in their social activities in relation to their treatment.13,14 Previous studies have shown that depression, anxiety, and emotional distress were linked with suboptimal drug adherence.8,9 Understanding the relationship between psychological changes and treatment adherence might help to improve poor adherence.
People with diabetes must regularly inject their insulin or take their other medication in the workplace for optimal glycemic control. 15 Employees with diabetes need blood glucose testing at regular intervals, short breaks during the workday to administer insulin, and a place to store insulin or other supplies. 15 However, patients have reported having no proper workplace environment for treatment management. An inappropriate workplace environment may lead to poor drug adherence. 16 Therefore, nurses should explore how workplace environments impact treatment adherence for adults with type 2 diabetes, to develop a suitable workplace with employers, administrators, and supervisors.
Previous studies have reported that sociodemographic variables and factors related to the patient, diabetes, and healthcare provider influence adherence to antidiabetic drug treatments.8,9,17 However, these studies have focused on the relationship with a single dimension, giving an insufficient understanding of the complex relationship of a wide range of barriers and facilitators to medication adherence in patients with diabetes. On the other hand, the assessment of social and psychological aspects as a whole could provide nurses with the necessary information to enable them to develop culturally appropriate interventions.8,9,17 Therefore, this study aimed to explore the relationship between adherence to antidiabetic drugs and the psychosocial adjustment of patients with type 2 diabetes mellitus.
Method and design
The study used a cross-sectional study design in which the data were collected via a questionnaire and analysed using descriptive and analytical statistics. This study is reported in accordance with strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. 18
Setting and sample
The study was conducted between March and June 2018. A convenience sample of participants was recruited from seven internal disease outpatient clinics at a public tertiary hospital, located in a large city that serves as a gateway to nearby rural and urban areas in the north-west region of Turkey. The inclusion criteria for the participants were being aged 18 years or older, being on diabetes medication(s), and being able to read and write in Turkish. Excluded were those with gestational diabetes, type 1 diabetes, cancer, or a psychiatric diagnosis. A total of 328 patients with diabetes were approached; of these, 28 refused to participate and 83 did not meet the criteria. The questionnaire survey was completed by 217 patients with diabetes.
The sample size was calculated with G*Power version 3.1.2 software. 19 A post hoc power analysis was based on the correlation coefficient between psychosocial adjustment and adherence to medication. A power of 0.90 was determined at a 0.2 effect size and an alpha of 0.05.
Data collection
The Adherence to Refills and Medications Scale (ARMS-7) and Psychosocial Adjustment to Illness Scale—Self Report (PAIS–SR) were collected from the patients during their visits to the outpatient clinics of the university hospital, which took approximately 25–35 minutes.
Adherence to medication was measured using the ARMS-7, which consists of seven items, each with a four-point response scale. The possible score ranges from 7 to 28, and lower scores indicate better adherence. 20 Cronbach’s α of the original scale was 0.814. Test–retest reliability showed a good correlation (r = 0.693). Concurrent and construct validities of the ARMS-7 were achieved by significant correlations between ARMS-7 scales and a theoretically selected study instrument. 21 The validity and reliability of the Turkish version were tested by Gökdoğan and Kes. 20 Regarding the reliability of the Turkish version of the total ARMS‐7, the Cronbach’s α was 0.75. The test–retest reliability was 0.80. The factor correlation varied between 0.57 and 0.84. The factor structure of the Turkish ARMS‐7 indicated satisfactory concurrent validity. 20 The original and Turkish versions of the scale evaluate adherence to drug regimens among patients with chronic disease.20,21 In this current study, the Cronbach’s α coefficient for the total ARMS‐7 was 0.83, and subscale reliabilities (taking medication and refilling medication) were between 0.66 and 0.79 for patients with type 2 diabetes mellitus.
Psychosocial adjustment was measured using the PAIS–SR, which consists of 46 items, each with a four-point response scale (0–3), with lower scores indicating better psychosocial adjustment. Scores of under 35, between 35 and 51, and over 51 are considered to indicate good, moderate, and poor psychosocial adjustment, respectively. The PAIS–SR consists of seven subscales: healthcare orientation, domestic environment, vocational environment, extended family relationships, sexual relationships, psychological distress, and social environment.22–24 The Cronbach’s α for each subscale varies from 0.68 to 0.93. Inter-rater reliability coefficients for the PAIS–SR have ranged from 0.74 to 0.86. 22 The original scale has good convergent, predictive, and construct validity.22,23 The reliability and validity of the Turkish version were tested by Adaylar. 24 The Cronbach’s α was 0.92 for the reliability of the Turkish version of the total PAIS–SR. The Cronbach’s α for each of the seven subscales varies from 0.78 to 0.96. The factor correlation varied between 0.38 and 0.84. 24 In this current study, the Cronbach’s α coefficient for the total PAIS–SR was 0.93, and subscale reliabilities ranged from 0.74 to 0.94 for patients with type 2 diabetes mellitus.
Statistical analysis
The variables were investigated using visual methods (histograms and probability plots) and analytical methods (Kolmogorov–Smirnov and Shapiro–Wilk tests) to determine whether or not they were normally distributed. Student’s t-test was used to assess the differences in psychosocial adjustment and adherence to medication according to sociodemographic variables. Pearson’s correlation was used to assess the relationship between adherence to medication and psychosocial adjustment. 25 Cronbach’s α was calculated for the PAIS–SR and the ARMS‐7 to evaluate the reliability of the measures in this sample. Findings were considered statistically significant at p < .01 or p < .05. 26
Ethical considerations
Ethical approval was obtained from the ethics committee (approval no. 9/6) at Karabük University. Approval (approval no. 98024045/604.02.99) was also obtained from the selected hospital clinics. Informed consent was obtained from each participant. This study was conducted taking account of the Declaration of Helsinki. 27
Results
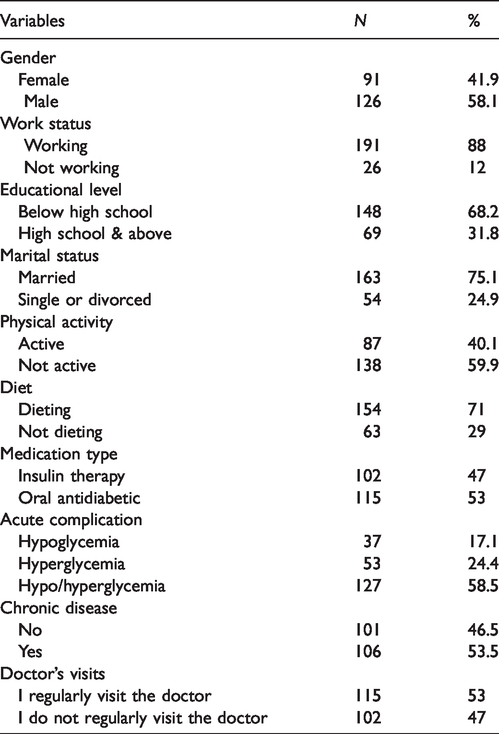
The mean age was 57.28 ± 13.43 years; the duration of diabetes, use of insulin, and use of oral antidiabetic medication were 10.21 ± 6.77 years, 7.52 ± 6.52 years, and 8.43 ± 5.57 years, respectively. The sociodemographic characteristics and health status of the patients are shown in Table 1. More than half (58.1%) of the participants were males. The majority of the respondents was married (75.1%) and working (88.0). Hypoglycemia was reported by 17.1% of patients and 47.0% of patients had received insulin therapy.
Patients’ demographics and health status (n = 217).
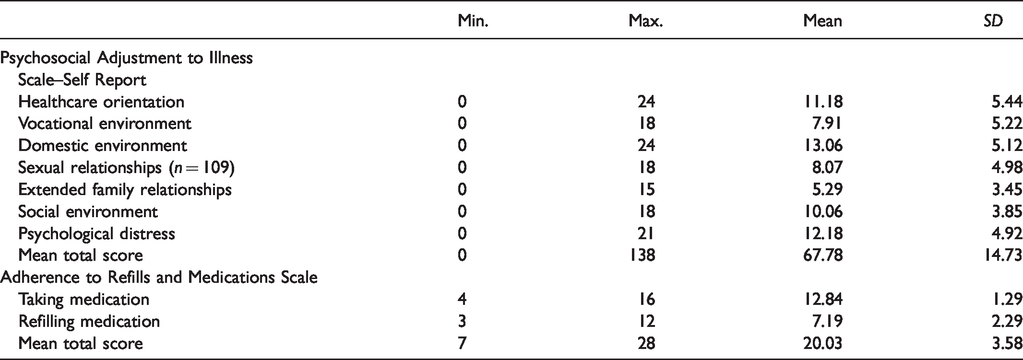
As shown in Table 2, the participants’ mean total score on the PAIS–SR was 67.78 ± 14.73, indicating poor psychosocial adjustment as it was above 51. The three domains of the PAIS–SR exhibiting the greatest adverse effects were healthcare orientation (mean 11.18 ± 5.44); domestic environment (mean 13.06 ± 5.12); and psychological distress (mean 12.18 ± 4.92). The participants’ mean total score on the ARMS‐7 was 20.03 ± 3.58, indicating poor adherence.
Mean scores on the Adherence to Refills and Medications Scale and the Psychosocial Adjustment to Illness Scale–Self Report (n = 217).
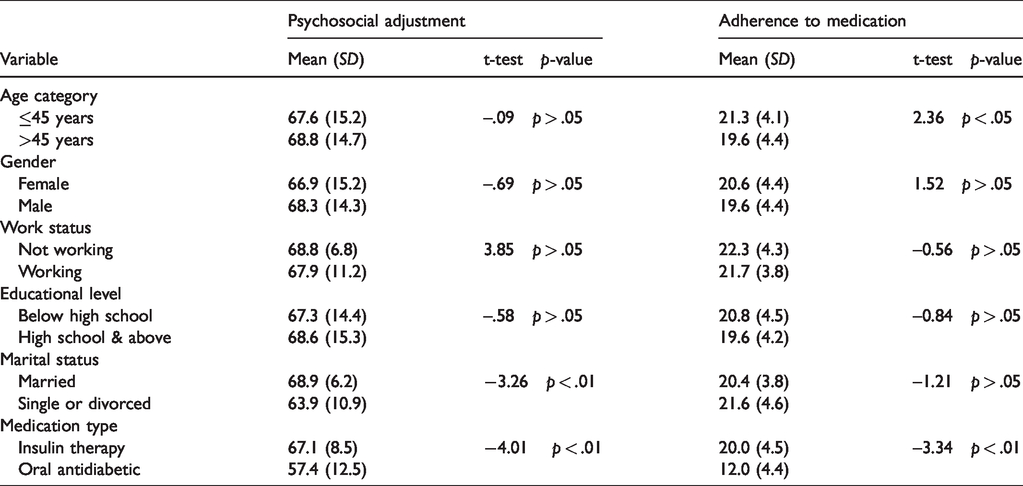
The differences in psychosocial adjustment and adherence to medication according to sociodemographic variables are shown in Table 3. Analysis of the data revealed that psychosocial adjustment was significantly different between married and other participants (t = –3.26, p < .01). Additionally, patients using insulin therapy had worse psychosocial adjustment than those using oral hypoglycemic agents (t = –4.01, p < .01). However, no significant differences were found in psychosocial adjustment according to age, working status, gender, or educational level. Regarding adherence to medication, statistically significant differences in age were found between the two groups of patients (t = 2.36, p < .05). Additionally, patients using insulin therapy had poorer drug adherence than those using oral antidiabetic drugs (t = –3.34, p < .01).
The differences in psychosocial adjustment and adherence to medication according to sociodemographic variables (n = 217).
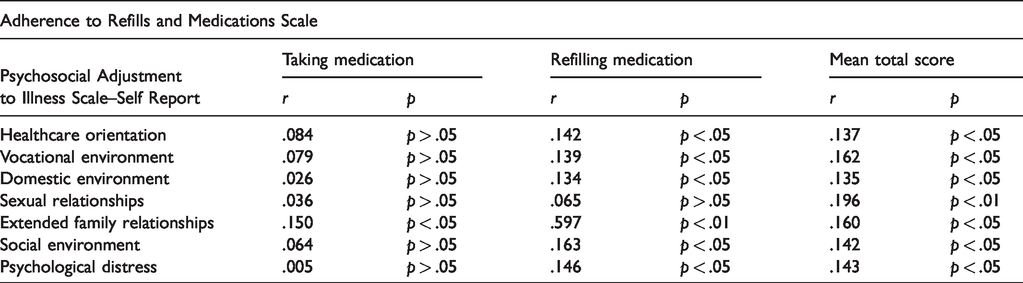
As shown in Table 4, Pearson’s correlation analysis indicated a significant weak positive correlation between all domains of the PAIS–SR and the total scores on the ARMS‐7. This means that participants with worse psychosocial adjustment, such as in family relationships, sexual life, psychological status, and vocational, domestic, and social environment, had poorer adherence to medication. Similarly, the participants’ scores on medication refill were found to be significantly and positively correlated with all of the PAIS–SR domain scores except the sexual relationships domain. However, no significant relationships were found between the taking medication subscale score and the psychosocial adjustment domain scores, except the extended family relationships domain.
Correlation between psychosocial adjustment and medications adherence (n = 217).
Discussion
This study analyzed the association between psychosocial adjustment and drug adherence among Turkish diabetes patients. We found that patients using insulin therapy had poorer drug adherence than those using oral hypoglycemic agents, which was consistent with the results of Krass et al. 1 One possible explanation for this might be that, compared with oral medication, insulin injection is relatively complicated in terms of skill and knowledge. This indicates that nurses should comprehensively assess patients’ barriers to insulin use regularly and prepare educational interventions. Similarly, patients using insulin therapy had worse psychosocial adjustment than those using oral hypoglycemic agents, which was in line with the study of Turten-Kaymaz and Akdemir. 28 This may be because experiences of pain and fear of needles can lead to psychosocial maladjustment.
Healthcare orientation is defined as the patient’s attitude to their health, their health knowledge, treatment information, their expectations of the results of treatment, and so on. 23 Healthcare orientation has been assessed using either qualitative methods or different scales in previous studies.12,29,30 Negative attitudes towards drug treatment, denial towards diabetes, lack of knowledge about diabetes or medication, and beliefs that drug treatment is ineffective or harmful have been related to poor adherence to drug regimens.12,29,30 We found that worse healthcare orientation was associated with worse medication adherence, which was partly consistent with previous studies.12,29,30 The results suggest that nurses should assess patients’ knowledge, attitudes, and beliefs about antidiabetic drug treatment. Education about the benefits of drug treatment may help to improve adherence.
The vocational environment is defined as including the patient’s job performance, problems at work, time at work lost, changed job goals, and so on. 23 Few studies have examined the association between drug adherence and vocational environment.31,32 Kearney et al. 31 found that adherence to drug treatment was significantly related to the work environment, which is consistent with the findings of this present study. However, DiBonaventura et al. 32 found no significant relationship between drug adherence and absenteeism (time at work lost). The results of those two studies may have varied because of differences in workplace policies and procedures.31,32 Additional research is needed to understand the relationship between work environment and drug adherence. Our study outcome may contribute to nursing practice towards regulating work environments, such as providing short breaks and a place to store and administer insulin.
Family member attitudes and communication have a significant impact on a patient’s psychological wellbeing, decision to initiate antidiabetic drug treatment, and ability to maintain the drug regimen. 10 Our study was similar to another in which patients with a high level of family support also had a high level of drug adherence. 11 An additional study showing that patients living with obstructive families or who had unsupportive families had low adherence to drug treatment also supports our study. 10 Our study found that patients with diabetes received poor support from their families, which might lead to poor adherence. Poor family support might derive from a lack of knowledge about treatment or families’ negative views and experiences. Including family members in diabetes education by explaining how they can best support the patient in drug adherence could help. 33 Notably, previous studies have focused on drug adherence of patients with diabetes who received support from nuclear family environments.10,11,33,34 Therefore, it is largely unclear whether distant or close relatives provide support around adherence.10,11,33,34 This present study found that better family relationships were significantly related to better adherence to drug treatment. This suggests that nurses can make use of patients’ relatives to improve medication adherence. For example, relatives might support patients with diabetes by filling pill boxes, picking up prescriptions, paying for medications, or providing transportation. 34
The patient’s psychological support is considered a key factor in providing patient-centered care.8,9 Previous studies have revealed that depression, anxiety, and diabetes-related distress were related to suboptimal medication-taking behaviors, which is consistent with the findings of this study.8,9 These results suggest that nurses should monitor any changes in the patient’s mental health status, such as distress, anxiety, or depression, and collaborate with other health professionals such as psychologists or psychiatrists. Additionally, we found that one of the most negatively affected areas was psychological distress. One possible explanation for this might be the lack of either social or domestic environment support.
The social environment can affect negatively adherence to drug treatment.13,14 Qualitative studies have indicated that patients with type 2 diabetes feel embarrassed when injecting insulin at social events, and thus patients report either delaying or omitting injections.13,14,16 Further, a study by Billimek and Sorkin reported that living in unsafe neighborhoods was associated with delaying filling a prescription. 35 Another study similarly revealed that the neighborhood social environment was associated with adherence to oral hypoglycemic agents. 36 The findings of this present study are similar to those of previous studies showing that poor social environment was related to poor adherence to drug treatment.13,14,16,35,36 The public may have misperceptions about using insulin. For example, when patients with diabetes inject their insulin in public, they may be misidentified by others as using illicit drugs. 16 Nurses can prevent misperceptions about using insulin through increasing awareness in society. Additionally, they should help to enhance patients’ confidence and motivation to continue taking their medication at social events. 37 Effective communication between nurses and diabetes patients could improve these factors.
Methodological considerations
According to the post hoc power analysis, this study had adequate power to detect statistical significance. Moreover, the statistical analysis indicated that the scales were suitable and reliable for measuring the relationship between psychosocial adjustment and drug regimen adherence.20–24
However, the study has several limitations. First, the study recruited Turkish patients with diabetes from one university hospital in a large city in Turkey. Therefore, its generalizability is limited and the findings might not be applicable to other clinical settings or other countries. In addition, this study was descriptive and correlational, and so cannot examine the causal relationship between adherence and psychosocial adjustment. Therefore, developing longitudinal studies of patients with diabetes from diverse ethnicities and larger populations is recommended to examine the causal relationship.
A single measurement method (such as self-reporting) cannot be sufficient to assess drug regimen adherence. Therefore, combining at least two methods can give more reliable results. For example, future research could combine an objective method (such as the presence of the drug or a metabolite concentration in body fluids) and a subjective method (such as electronic monitoring devices, pill count, or self-reported questionnaire). 7
Although a significant weak correlation was found between psychosocial adjustment domains and drug regimen adherence, future research should analyze the mediating role of psychosocial adjustment on drug regimen adherence. Finally, the use of convenience sampling limits this study because of potential selection bias and the representativeness of the sample. Future studies should consider random sampling to give a better representation of patients with diabetes.
Conclusion
Our study showed a weak but significant positive correlation between all domains of the PAIS–SR and the total scores on the ARMS‐7. Additionally, patients using insulin therapy had worse psychosocial adjustment and drug adherence compared with those using oral hypoglycemic agents.
Psychosocial care could play a crucial role in improving drug regimen adherence among patients with diabetes. Therefore, nurses should integrate psychosocial care into daily practice. Nurse trainers can organize education programs to increase nurses’ skills in psychosocial assessment and practice. Future research could evaluate the effect of workplace-based interventions on antidiabetic drug adherence. Another area of interest for future research suggested by this study’s findings may be exploring how the relatives of patients are involved in medication adherence.
Footnotes
Author contributions
Study design: DK, FG. Data collection: DK. Data analysis: DK, FG. Manuscript writing: DK, FG.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.