
Abstract
When children are seriously ill, being able to be cared for at home with the family is valuable, but community nurses are often not trained to care for children. The aim of this study was therefore to describe community nurses’ perceptions of caring for seriously ill children at home. A content analysis was conducted of 11 semi-structured interviews with nurses. One theme, obligation to care, was found, followed by three categories: making an impact, feeling confident, and emotional processing. In conclusion, we found collaboration with paediatric staff in the hospital is important for community nurses in order to gain confidence, which would optimise care at home for seriously ill children and their families.
Keywords
Introduction
The number of children with serious illness being cared for at home is increasing worldwide. 1 When children are living with a life-limiting condition, family time together at home is precious. 2 To be cared for at home gives comfort to the children as well as their families3–5 and it helps them to maintain normality and everyday life.6,7 Continuity of care is important for these families,8,9 yet families often face challenges and parents may need to develop specialised knowledge and skills to manage their child’s care, such as for the technology used when the children need it. It can also be demanding and a burden for parents when the healthcare service relies on them and expects them to provide part of the care.1,2 When children are hospitalised, the parents often struggle to divide their time between being in the hospital with the ill child and at home with the healthy siblings. Guilt is therefore commonly expressed by parents who are unable to devote enough time to their other children10,11 and siblings feel lonely when the parents spend a lot of time away from home.3,12
Children who are suffering from a serious illness face a tough period, which pervades the lives of the entire families.13,14 By using the theoretical model family-centred care (FCC), health professionals can involve the entire family in care, rather than only the ill child.15,16 In a family, members are included in each other’s lives and the life situation of one member will influence the lives of the others. Consequently, it is desirable that the child who is ill and their family are seen as a unit and that the nurse meets them as a unit.17,18
Home-care services can differ in structure but community nurses in Sweden, as well as internationally, are generally trained to care for and predominantly work with adult patients,19–21 which means that they rarely come to care for children. Consequently, it becomes difficult for them to gain the updated knowledge, skills, and experience needed for these patients.7,22 In addition, children who receive home care are a heterogeneous group with a wide spectrum of diagnoses. 20 Besides the professional challenge, this means that taking care of seriously ill children at home can raise strong emotions in the community nurses involved.23–26 Earlier studies in this field have focused on the risk of community nurses becoming too close to the families and stepping out of their professional identity,11,22,24,27,28 and on difficulties regarding community nurses’ experience and education when providing care to seriously ill children at home.7,19,20,22 However, there is still a lack of knowledge about what nurses themselves perceive when caring for these children in geographic areas with no specialised palliative home-care service for children. Therefore, the aim of this study was to describe community nurses’ perceptions of caring for seriously ill children at home.
Method
This qualitative descriptive study 29 was conducted between March and April 2014 in the south of Sweden, in a county with a population of approximately 200,000 inhabitants. Qualitative content analysis was chosen since it is a suitable method for analysing interview data. 30 The inclusion criterion was nurses who had cared for at least one seriously ill child (aged 0–18 years) at home. No medical diagnoses of the child were excluded and no minimum working experience was set.
A purposeful sampling procedure was used 31 to ensure participants had the knowledge and experience sought for. In the sampling procedure, the medically responsible nurses from all eight municipalities were asked to suggest community nurses who fulfilled the inclusion criterion. Seven medical responsible nurses responded, of whom six had eligible nurses in their municipality. Altogether 16 potential nurse participants were identified. The first author then contacted the nurses by telephone to inform them about the study and ask if they were willing to participate. Eleven nurses from six different municipalities gave their oral informed consent and chose the time and location for the interview. Before the interview, they were informed once again about the study and gave their written informed consent.
The included nurses were ten women and one man between 29 and 60 years old (mean 47 years). Four nurses were general nurses and seven nurses were district nurses (one of these was also a specialised paediatric nurse). The nurses had worked in home care for between six months and 34 years (mean 12.5 years), in urban and/or rural areas. They had experience of caring for children suffering from cancer, meningitis, children who had had a tracheostomy, and/or children who were being treated with a respirator at home. The number of seriously ill children the participants had cared for varied from one to several children.
Data were collected through semi-structured interviews. 32 An interview guide with open questions specifying areas to be covered in each interview was developed by the first and second authors. The interview guide was then tested in two pilot interviews, which resulted in some minor corrections to the sequence of the questions to obtain a better flow in the interviews. As only minor corrections were needed to the interview guide, the pilot interviews were included in the study. Initially, the interviewer (i.e. the first author) asked the nurses to narrate an experience of caring for a seriously ill child at home. Examples of questions were: ‘How do you prepare for the meeting with the child and the family?’ ‘How do you experience the contact with the families when caring for children?’ ‘Do you have the possibility to share your experiences with colleagues?’ ‘What do you need to feel good when caring for ill children?’ ‘How do you create wellbeing?’ All interviews took place in the nurses’ offices, were audio-recorded, and lasted between 19 and 45 minutes (mean 32 minutes). The first author then transcribed the interviews verbatim.
The interviews were analysed using qualitative content analysis at both manifest and latent levels. 30 The analysis was performed in several stages. Initially, each interview was read repeatedly to acquire a first understanding, to become familiar with the text and to obtain a sense of the whole. This was followed by analysis of the text where meaning units (i.e. constellations of words that relate to the same central meaning that reflects the aim of the study) were identified. The meaning units were then condensed and abstracted to create codes. The codes were continuously compared to recognise differences and similarities. Based on the codes, categories were developed which represented the manifest content of the text. A further process of discussion resulted in an agreement concerning the underlying meaning, which is the latent content. This was formulated into three categories and one theme, which reflected the community nurses’ perceptions of caring for seriously ill children at home.
Although this description indicates a linear progression it is important to remember that the process of analysis involved a back-and-forth movement between the parts of the text and the whole. 30 During the whole analysis, the first author, who is a paediatric nurse with experience of caring for children in hospitals, regularly took a step back to critically reflect on her own perspective of the data. The other authors, two registered nurses and one behavioural scientist, had no experience in paediatric nursing, but had experience of the research method. The authors analysed the transcribed text individually, and the coding and the theme system were discussed on several occasions to reach consensus about the interpretation of the data.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki 33 and was approved with written consent by the Region Kronoberg Research Ethics Committee Council (case no. EPK 211-2014). Permission to conduct the study was given by seven medically responsible nurses in the municipalities of the county, although only six of them suggested eligible nurses. Before the interviews, the nurses were informed about the aim of the study, that participation was voluntary, and that they had the right to cancel the interview or to decline to answer. Confidentiality was assured. All nurses gave both their oral and written informed consent.
Results
The theme and the three categories with their subcategories.
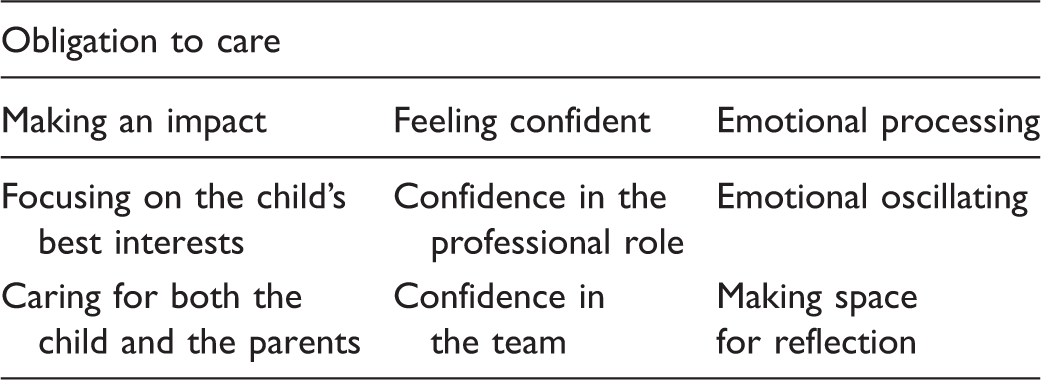
Obligation to care
The nurses felt that it was their obligation to care for seriously ill children in their homes. They experienced a responsibility to provide equal care for everyone, regardless of the age or the disease of the children. They indicated that if adults have the right to receive care at home, children should definitely have the same right too. Care of seriously ill children was a high priority and sometimes other patients had to wait because children were prioritised. There were sometimes even feelings of taking more responsibility for the children’s care than was asked for. Each of the nurses also felt that it was their responsibility to gain the necessary knowledge to be able to provide good care; for example, by going to the paediatric ward in the hospital to watch and learn. I think that if the child wants to be home it should be allowed, regardless of age. That is my opinion. And then it is my responsibility to make it as good as possible. (Nurse 4)
Making an impact
The nurses had experienced making an impact through their caring as well as being able to influence the outcome of the situation. They could make an impact through focusing on the child’s best interests and by caring for both the child and the parents.
Focusing on the child’s best interests
It was important for the nurses to adapt their care individually to the specific child who was being taken care of and to maintain continuity as much as possible. However, the child’s need to go to school and meet friends sometimes clashed with the nurse’s goal of achieving continuity. The nurses often had the opportunity to prioritise their work so that the visits could take as long as needed. They thought that the children were safer when they were cared for at home. To create safety and make the home environment as ordinary and normal as possible was important for the nurses. For the kids’ sake, I think it’s wonderful to be able to take care of them at home where they are in their home environment, where they have friends around, and where they can lay in their own bed, and it becomes as natural as possible for them. (Nurse 8) The toughest thing was when we had that boy who died; it was the worst thing I’ve done, ever. But, I would do it again tomorrow if someone came and asked me. For him and for them, to be able to stay at home. (Nurse 4)
Caring for both the child and the parents
It was important to the nurses that the families could have as normal a life as possible despite the child’s serious illness. The importance of involving the parents and cooperating with them was also emphasised. The nurses reflected on the parents’ involvement and how they should act in the home so that the parents would not feel excluded. And then, above all, I think it’s very important that the parents are involved, that they are responsible for the child, and that we are helping each other. Because I think it’s a risk taking too much responsibility from the parents so they feel insecure in their role later on. (Nurse 9)
The nurses expressed that they had great opportunities to influence and make a difference for the family. These opportunities could involve taking responsibility for the child and giving the family confidence because a nurse was available nearby and could come quickly whenever needed during the day. These could also include taking responsibility for the child’s and parents’ needs and wishes to receive care at home by speaking up against colleagues and people in other occupations who considered that the families could use primary care or the hospital when the child needed care.
Feeling confident
Feeling confident was necessary to be able to communicate a feeling of safety to the children and the parents. Confidence was needed in nurses’ professional role but also in the team.
Confidence in the professional role
The nurses emphasised the roles of experience and competence in being able to feel confident when meeting with children and families. Further knowledge of child healthcare was sought; for example, of pharmaceuticals and of how the environment could be adapted in the best way. The nurses felt secure in handling the technical equipment around the child, such as infusions, but they had a lack of experience relating it to children. In acute situations, and when a child was dying, it was considered a great safety to have a direct number for the paediatric clinic where someone who knew the child always answered the telephone. Long experience in the profession resulted in more confidence in caring for children. We asked what we were going to do and it was just an ordinary thing for us, a subcutaneous venous port, which we were supposed to handle. We were asked to give him intravenous antibiotics, which was something we had done before and therefore felt confident to do. (Nurse 6)
Confidence in the team
The nurses had confidence in other nurses in the group and described how this facilitated care of the children. The nurses described spontaneous reflections with colleagues at work, which increased their self-reliance and helped them to feel safe in their professional capacity and in the meeting with the child. The more experienced nurses supervised those who lacked experience. Working in teams also provided an opportunity to relieve the pressure on each other. The nurses stated that they had a great understanding for each other if someone occasionally had to take a break from a certain visit. Even in small villages this was possible because colleagues from nearby came to help. Only a few nurses had professional counselling. In some geographic areas, it was considered possible to receive professional counselling if needed, whereas in others it was not possible at all. Maintaining competence in the team as well as of the individual nurses was difficult when not caring for ill children regularly. The nurses gave several examples in which competence should be maintained. They wished that more children could be transferred from hospital to home care. They also suggested that there could be a consultative team from the children’s ward in the hospital that could be turned to when information and support was needed. It was perceived to be problematic for the teams in the community that there could be a very long period between the episodes when children were in home-based care. We need to have a routine in the community to find good routines for how to make it work, because I mean, now it can be a year between the occasions when we have a child and I think that’s a pity. (Nurse 8) We work very much together. Having a colleague with you. We cannot always work in pairs but we try to as much as we can. And that’s how we can be updated on each other’s cases because we also have days free. It’s a feeling of safety. (Nurse 11)
Emotional processing
Caring for seriously ill children at home affected the nurses emotionally and they needed to process these emotions. To do this, they oscillated emotionally and made space for reflection.
Emotional oscillating
The nurses experienced grief when they cared for seriously ill and dying children. They expressed feelings of injustice and said that it was difficult not to think that the children had not lived their lives. The nurses tried to think that it was not their own grief but the grief of the families. Several nurses said that they were calm when they visited the families but let their feelings out and cried afterwards. The nurses described how they oscillated between different feelings and roles when they cared for seriously ill children. Well, you enter your role as a nurse, thinking that you must be professional and you check that everything is OK and then, afterwards, you can let go of your feelings, because I mean, you cannot do that with the family, it must be afterwards in that case. (Nurse 3) You see how good it is for those who actually are allowed to stay at home. You feel that they really can be there all the way and they can lay in their own bed and it is not at all as it is in the hospital; it is their home and they are always most safe there. And if I have the opportunity to make it good there, then I feel that it has been good despite it being tough in several parts. (Nurse 3)
Furthermore, joy was reported in the care of seriously ill children in terms of being able to care for them in their homes where the children have their family, friends, and their own belongings. One nurse who had cared for a dying child described that they had laughed together and it had generated positive feelings to be able to give care at home.
Making space for reflection
Having time for reflection was mentioned as being of importance. On days when this time could not be set aside, it was harder to mentally leave work when going home. The work was then processed at home instead. Living and working in the same place also made it harder to relax at home. Difficulties with ‘changing’ and being happy and positive when coming home to their own family were also mentioned. Having some travelling time to and from work made it possible to reflect during the travel. The nurses tried to think that they did a good job and that they helped the family in their current situation. The nurses mentioned that they imagined what it would be like to be in the situation of having a seriously ill child. They thought that they too would have wanted home healthcare for their child. Then, I think that I have always tried to do my best and focused on what went well. I also reflect on what I could have done differently, and then reflect on this with colleagues; what went well and what doesn’t feel good. What do we want to bring to the next time? (Nurse 1)
Discussion
This study provides knowledge about community nurses’ perceptions of caring for seriously ill children at home. The findings showed that the nurses perceive that they have an obligation to care for the children; that is, they consider it their responsibility to care for children as well as for adults at home. The nurses also experienced having an impact on the lives of children and families when caring for them at home. However, to do so, it was necessary to feel confident, both in their professional role and in the team. In addition, the nurses used emotional processing to handle the strain that caring for seriously ill children can cause.
The theme in this study, obligation to care, indicates that the nurses perceived themselves as having an obligation to care for seriously ill children at home. The nurses described a genuine desire to do well for the families and a strong desire to deliver care to the best of their ability, which is congruent with previous research.7,26,34 Feeling personally responsible for providing adequate care 20 can, however, lead to the situation that nurses become everything to everyone, 11 that is, working outside their job descriptions to make create the best possible situation for children and families. In this study, this desire and the prioritising of a seriously ill child could also imply that other patients had to wait for help from the nurses because much time was spent with the child.
This study showed that the nurses perceived that they could make an impact on the lives of seriously ill children and their families. Previous research shows that all family members are affected when a child is seriously ill and in need of care.3,4,6,12–14,35 For parents, having a seriously ill child who requires a long period of care may have a negative impact on their mental and physical health.1,9 When family-centred care (FCC) principles are applied to this care, it can improve the situation for the family. It has been shown in a recent literature review that increased family involvement in the care of ill children can reduce anxiety and increase satisfaction with the care provided as well as improving communication with health professionals. 36
The results highlight how essential it is for nurses to feel confident in the team. The nurses reported that they obtained guidance mainly from their team members and not from the healthcare organisation. Similar findings have been found in previous research that also stresses the importance of supportive professional relationships.19,20,23,26 Furthermore, nurse continuity was recognised as being even more important when a child was being cared for in comparison to an adult. Previous research has found that family members also report continuity of care as being important and this was perceived as key in ensuring that the nurse knew and cared about the child and parents, 9 that is, for example having one special nurse who could remember what happened last time they met.4,8 O’Brien and Duffy stress the importance of continuity and point to positive effects, such as the possibility of building relationships with the family, when the community nurse is involved from an early stage. 2 Continuity and building relationships are important elements in FCC, but to provide effective FCC, health professionals and families need to collaborate as equal partners. 37 However, it has been shown that, in practice, nurses who want to use FCC experience difficulties in implementing this model of care. 38 It is therefore important to educate health professionals about children’s and families’ needs, but it is also important to educate the children and the families themselves. 39
Feeling confident in their professional role was seen by nurses in this study as necessary when caring for seriously ill children at home. The study showed that close relationships between the children and nurses are common when meetings take place in the children’s homes, which could create problems for professionalism. The findings concerning these strong links that are often established between the nurse and the child are in agreement with results from previous studies that all describe challenges to the professional approach when caring for seriously ill children at home.11,22,24,26–28 Several nurses in the present study expressed a wish to work in pairs so that it would be easier to focus on both the parents and the child. This is an important finding as the community nurse often has a lone working role. 27
The present study also highlighted the risk of emotional strain, such as grief when a child is dying. Grief is a commonly described emotion in research associated with caring for seriously ill children at home.13,23–25,27 When a child is dying, Reid reported emotional wrestling and fearful anticipation experienced by nurses. 24 Sandgren et al. identified a strategy called professional shielding that means that, in order to protect themselves emotionally, the nurses strike a balance between distance and involvement in their relationship with the patient. 40 Much resemblance to this approach was seen in the present study in which the nurses described how they used emotional processing and oscillated between distance and involvement.
The present study interestingly identified that nurses also experience feelings of joy when caring for seriously ill children at home. In previous research, joy is rarely described in this situation. However, in a study of nurses caring for children with cancer who were undergoing radiotherapy, joy was described in meeting with the child. This emotion was based on the ability to make the child feel better and on the gratitude of both the child and their parents. 41 Furthermore, the importance of making space for reflection was reported by the nurses in the present study. Earlier studies have also emphasised the need for reflection when working with seriously ill children, in terms of both self-awareness and protection, as a person and a professional.22,42
The majority of community nurses have no education or training in caring for ill children 20 and they may therefore not necessarily have the skills and expertise to manage. 19 Consequently, nurses in the present study expressed a need for team guidance in terms of education, momentary support, and consulting with paediatric staff in the hospital to be able to feel confident in their professional role. This finding is in line with earlier research.2,7,19,20,26 The importance of cooperation between the paediatric ward where the children have been cared for and the community nurses who are to take care of the children at home has been highlighted, 20 as have the children’s and families’ right to expect the nurses to have the knowledge and skills that are required. 2
Methodological considerations
It may be considered a limitation of this study that the medically responsible nurses in the communities suggested nurses for participation; therefore, the sample may not be representative of all nurses in community healthcare. However, the selection process was designed with a view to promote heterogeneity. It is therefore considered a strength that the 11 nurses were recruited from different municipalities. Although there was only one male participant, this is representative of the distribution of gender in nursing. The participants also varied in age and experience, which can be considered as a methodological strength.
To assure trustworthiness 31 the first author strived to be aware of preconceptions arising from being a specialised paediatric nurse and continuous discussions about the analysis took place between the authors. The credibility of the study was strengthened by transparency in the analytical process, with quotations from the interviews being presented with the findings. In order to assess the transferability of the results for the reader, 31 the data collection process has been described in as much detail as possible.
Conclusions
This study highlights how nurses feel an obligation to care for seriously ill children at home while feeling that they can make an impact for both the child and his or her family. It is therefore important that they feel confident in their professional role as well as in the team. Nurses also need to be aware of emotional strain and must make space for reflection. The results confirm previous research that stresses the importance of collaboration with paediatric staff in the hospital in order for community nurses to achieve confidence. To optimise care for seriously ill children at home, more research is needed to explore how children themselves and family members experience being cared for at home by community nurses.
Clinical implications
In order to make home care for children possible on an equal basis regardless of their place of residence, there is a need to support the community nurses who are caring for the children. All community nurses need education in paediatric care to be able to give a patient secure care but they also need opportunities to reflect and to receive emotional support. Collaboration between community nurses and paediatric nurses in hospitals would be likely to benefit the healthcare professionals as well as the families involved. One way to administer this collaboration would be to set up consultative paediatric teams that could support community nurses when required.