
Abstract
Language barriers in the healthcare sector, for example as a result of failure to use a patient’s mother tongue, can lead to misunderstandings and/or care errors, especially when circumstances require that nursing staff or patients speak a language other than their own mother tongue. The aim of this study was to explore the importance of patients receiving care in their mother tongue. A hermeneutic approach was used and the method was inspired by content analysis. The data material was collected through semi-structured interviews with nine adult patients. One main theme and four subthemes were seen. The main theme was that care in a patient’s mother tongue can enhance quality of care. To reduce suffering in care caused by language barriers, nurses’ language skills should be supported and encouraged. Further research should focus on nurses’ perspectives on the significance of minority-language patients using their mother tongue in a nursing context.
Keywords
Introduction
Clear communication in healthcare is important for patients, 1 and nurse–patient communication is crucial to maintaining the quality of care.2–5 When nursing staff and patients do not speak the same language, serious communication problems may arise,6–8 which can also jeopardize patient safety and patients’ experiences of good care.9–16
Background
Human beings create their perceived reality and self through language. 17 In caring situations, because of its important emotional dimension, language is much more than a tool for communication. 18 It is easier to express feelings and emotions in one’s mother tongue than in any other language, because it is considered the ‘language of emotion’.18 Language barriers may lead to impaired caring relationships. 19 Language and culture are intertwined, and because of this there is a need to discuss the concepts in relation to one another. Piller 20 found that culture is a multifaceted concept that can be defined in many different ways, e.g. the essentialist assumption that people have or belong to a culture. Piller 20 also found, when analysing culture-related texts, that a cultural unit formed the scope of each underlying understanding of culture investigated in her work, and thus concluded that the nation can be considered a basic unit of culture. Piller even saw that, ‘intercultural communication is one domain where “culture” as concerned with the specific – and the different – ways of life of different national and ethnic groups is constructed’.20(p.16) Arasaratnam found in relation to intercultural communication that, ‘the determining factor is when cultural differences between the relevant individuals affect the communication exchange in ways which would have been insignificant had those differences not existed’.21(p.136) Arasaratnam 21 also maintained that people who do not share similar cultural values and beliefs do not communicate within the context of shared assumptions, and not sharing such a context can easily lead to misunderstandings. According to Piller, 22 multilingualism, a related concept, can be considered an umbrella term that encompasses an extensive range of linguistic contexts and practices. In today’s multi-ethnic society, it is essential to be able to communicate with people from different countries, and consequently intercultural communication is highly important. 23
Information asymmetries arise in healthcare when one party has skills and knowledge that the other party does not have but needs, 24 and Alpers 25 maintained that all healthcare staff–patient relationships are more or less asymmetric. Even greater asymmetry is seen when there are linguistic and cultural differences between healthcare staff and patients, e.g. patients’ dissimilar understanding of illness anthologies may make them even more vulnerable in care. 25 Such differences can make the building of a trusting and positive healthcare staff–patient relationship difficult, especially with ethnic minority patients. 25
The capacity to exhibit cultural sensitivity is also important for nurses,26,27 because such sensitivity enables nurses’ understanding of patients’ various needs. 28 A culturally competent nurse strengthens the caring relationship and patients’ positive experiences of care. 29 For nurses and patients with different cultural backgrounds, intercultural caring is the core of caring work. 30 Nurses’ experiences of minority language issues, or if they belong to a minority themselves, can impact how they treat patients from cultural minorities and how they understand language or communication difficulties. 28 Cultural problems that can emerge when nurses and patients do not have a shared language include confusion, misunderstandings, prejudice, negative attitudes, anxiety or misconstrued care instructions. 31 Likewise, the language used for communication may be perceived as being terse or rude or an impasse may arise in the caring situation. 18 Language barriers between nurses and patients in care can also result in dangerous situations and risks related to medication, pain treatment, diagnosis, the communication of risks and/or emergency situations. 32 To support healthcare staff, it is important that language barriers be adequately detected and reported. 32
Professional interpreters can help eliminate the risks that can arise as a result of language barriers and can help maintain the quality of care.29,33–35 Professional interpreters can be used to overcome linguistic, cultural and knowledge barriers, but they are not always available in healthcare settings.28,36 According to Roberts et al., 37 in bilingual countries nurses who belong to the linguistic majority population and have the country’s majority language as their mother tongue are often willing and capable of speaking the country’s minority language, provided they have mastered this language, when talking about everyday matters with patients who speak the minority language. Still, Roberts et al. found that nurses prefer to use their mother tongue when providing patients with important information about, e.g. medication. Other researchers have found that when healthcare staff speak to a minority language patient they use a ‘basic’ or simplified version of the majority language, which can lead to nurse–patient misunderstandings. 28 Bilingual patients often switch between languages, as they are unable to express themselves equally in both languages, and also tend to revert to their mother tongue when expressing strong emotions. 17
Researchers have found that nurses’ positive attitudes toward a minority language are important, because this indicates that the nurses use the minority language which in turn encourages minority-language patients to use their mother tongue. 37 While everyday discussions can help build good nurse–patient relationships, when caring for minority-language patients it is also beneficial that healthcare staff provide instructions in the minority language, although this requires good proficiency in the language. 37
Still, nurses’ positive linguistic attitudes tend to change when they experience problems in practice, and consequently practical courses on how to use professional interpreters in healthcare would be useful. 37 Jones et al. 38 found that healthcare staff underutilize professional interpreters, even though researchers and policy-makers alike recommend using such services. Practical courses 39 or education and training 40 have been found to possibly improve healthcare staff’s negative attitudes toward professional interpreter services.
If the patient’s right to a professional interpreter has not been taken into account, it can lead to serious consequences32,40 and thereby affect the quality of care. Using alternative means to communicate when professional interpreter services are not available can lead to misunderstandings, misinterpretations or even inferior care. Language brokers, i.e. non-professional, informal interpreters such as a patient’s next of kin, are sometimes used. 40 Yet researchers have found that language brokers often are dominant and excluding in their roles and often ‘speak as themselves’ rather than accurately transferring information.41,42
Aims
The aim was to explore the importance of patients receiving care in their mother tongue.
Theoretical perspective
A language policy perspective was assumed in this study. According to Thomason and Kaufman, ‘languages are a product of, and a vehicle for, communication among people’.41(p.4) The Office of the United Nations High Commissioner for Human Rights (OHCHR) 42 stated that language is key to social inclusion and can be seen as the centre of human activity, self-expression, identity and culture and must consequently be protected and respected. 42 Henderson et al. 43 found that because communication entails context and interaction, language skills are complex and socially constructed.
There are an estimated 5000–6000 languages in the world, yet according to Piller only 15 languages account for the overwhelming majority of Wikipedia entries: of these there are 2.5 times more entries for the first-most frequently used language, English (4,948,736), than for the second-most frequently used language, Swedish (1,974,655). 22 In the European Union (EU), language diversity and aspects of societal and individual multilingualism have been given rather high consideration, 44 and minority languages are seen as a valuable part of the cultural and linguistic heritage of the EU. 45 The European Charter for Regional or Minority Languages (ECRML) was drawn up in 1992 46 with the intention to preserve linguistic diversity throughout the EU and call attention to language planning concerns at the highest level, 45 even though its underlying purpose is nevertheless considered to be cultural. 47 In the ECRML it is stated that, ‘the protection of the historical regional or minority languages of Europe, some of which are in danger of eventual extinction, contributes to the maintenance and development of Europe’s cultural wealth and traditions’.46(p.15) Also, ‘the charter sets out to protect and promote regional or minority languages, not linguistic minorities’.46(p.16) In 2003 the European Commission launched the Action Plan 2004–2006, with the purpose of promoting language learning and linguistic diversity and this, along with other initiatives, has been considered one of the most important processes in the EU’s history and a turning point for the EU’s language policy. 45
The promotion and protection of the identities of linguistic minorities is perceived as being central to the rights of minorities, and as such is also important with regard to a person’s private life, identity and dignity.
45
According to the OHCHR, ‘“language rights” and “linguistic human rights” are human rights which have an incidence on language preferences of or use by state authorities, individuals and other entities’.42(p.4) Arzoz,
47
referring to Foucher, found that the idea underlying the recognition of language rights was to protect specific linguistic minorities, not every linguistic minority, and/or secure equal status for specific languages, not every language. While various recommendations for how the linguistic rights of national minorities can be secured exist, one can nevertheless conclude that, despite some differences, there are norms; the recommendations are all comparable and include central principles with regard to the language rights obligations of state authorities.
42
According to the OHCHR, the private sphere is one of the most significant areas of language rights, ‘where individual freedoms and other rights in international human rights operate to guarantee linguistic freedom in private matters’.42(p.10) Researchers have found that even the most indigenous language minorities in the EU still face losing linguistic ground in relation to the surrounding majority language, no matter how active said minorities are.
48
Some ‘old’ minority languages are solely used in a single European state, e.g. Welsh, and such languages can be considered ‘unique’, historical minority languages.
44
Other minority languages are used in more than one European state, with some languages being a minority language in one state yet a majority or national language in another state (or vice versa), e.g. Swedish, Dutch, French and German.
44
Some researchers have maintained that the minority or majority status of a language community depends on a specific (political) context.
49
Arzoz maintained that language rights, according to Green, can be perceived as: … special guarantees accorded to citizens as a ‘natural’ dimension of state-building or re-building, or as part of a legitimacy bargaining a post-dictatorial or post-racist state needs to make: if the state wants to have citizens’ trust, it has to provide for language rights. Thus, language rights are compromised rights of a fundamental sort.47(p.23)
In Finland, for historical reasons, both Finnish and Swedish are official languages. If one looks more closely at the Constitution of Finland, with regard to a citizen’s right to language and culture, it is stated under ‘Basic rights and liberties’ that: 1) The national languages of Finland are Finnish and Swedish. 2) The right of everyone to use his or her own language, either Finnish or Swedish, before courts of law and other authorities, and to receive official documents in that language, shall be guaranteed by an Act. The public authorities shall provide for the cultural and societal needs of the Finnish-speaking and Swedish-speaking populations of the country on an equal basis.47(p.29) Even if formulated as fundamental rights, constitutional language rights are not accorded for the sake of freedom and equality of all individuals and groups living in the state, but for the sake of basically protecting certain language communities (for instance, Swedish- and French-speaking citizens in Finland and Canada respectively).47(p.31)
Method
Study design
This was a qualitative study with semi-structured interviews. A hermeneutical approach in accordance with Gadamer 50 was used, and the researchers analysed the data with openness to reveal the subject matter. The data were analysed through content analysis inspired by Graneheim and Lundman. 51
Participants
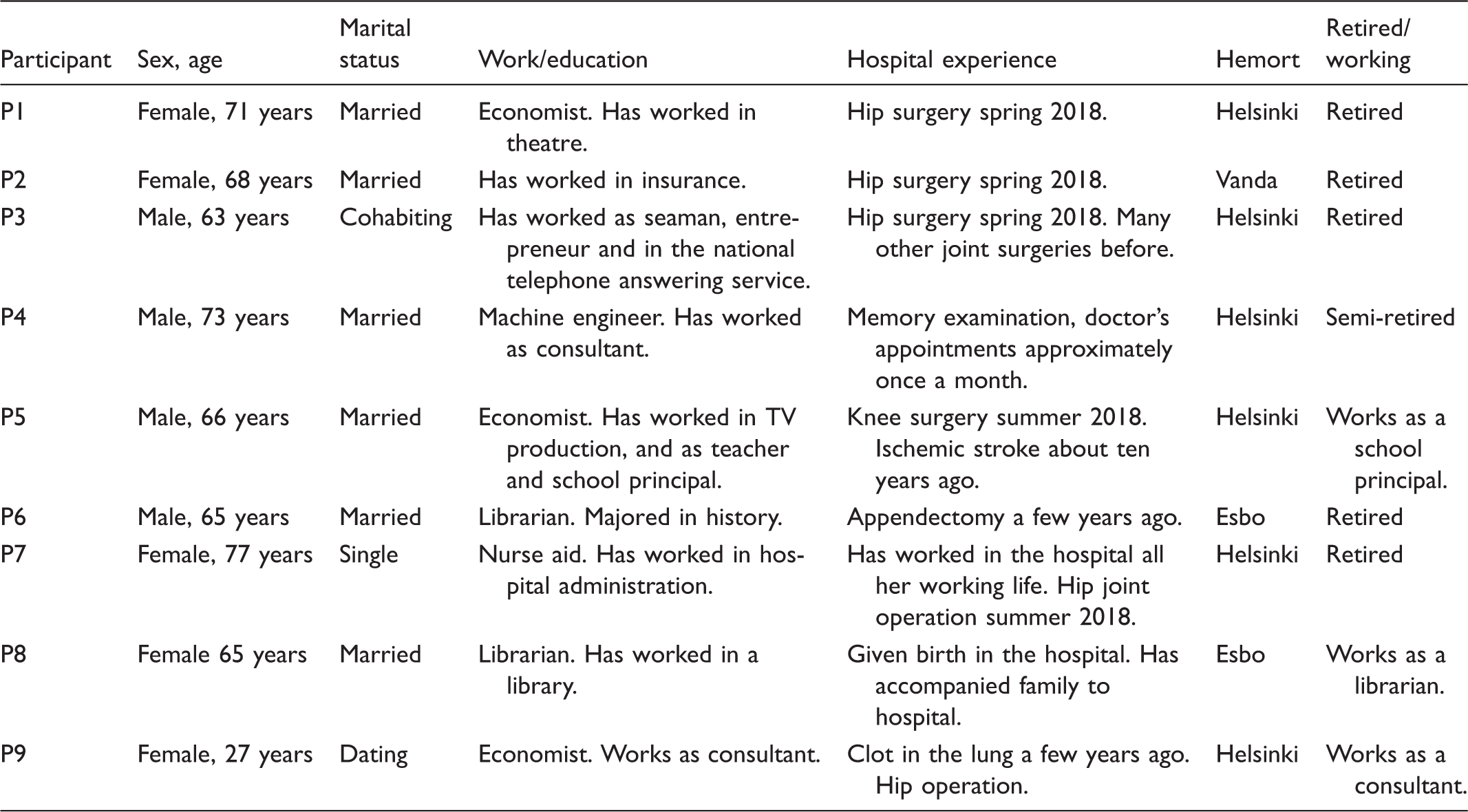
Characteristics of the participants.
In 2018 the total population of Finland was estimated at approximately 5.5 million. The two main official (national) languages are Finnish and Swedish, even though Swedish-speaking Finns are classified as an ethnic minority. Finnish is the majority language, and 4,835,778 individuals were registered in 2018 as having Finnish as their mother tongue. 52 In addition to Finnish and Swedish, several other languages are spoken in Finland, e.g. Russian, Arabic, Estonian, English, Somalian and Kurdish. 52
Swedish-speaking Finns constitute a significant portion of the population, numbering approximately 300,000, and are classified as an ethnic minority. 53 They form the largest minority group in the Nordic countries. In contrast to many other ethnic minorities, Swedish-speaking Finns are seen to be healthier, more prosperous, and have greater life expectancy than the majority population. 53 Because Swedish is an official language, Swedish-speaking Finns have the right to receive services in their own language. Furthermore, in those municipalities where at least 8% of the population or at least 3000 individuals are registered as Swedish-speaking, state/municipal services in the Swedish language are guaranteed. 42
Patients’ right to service in the national languages of Finland, in accordance with own language (mother tongue) is emphasized in the Language Act (423/2003), 54 the Constitution of Finland (731/1999) 55 and the Act on the status and rights of patients (785/1992). 56 In Section 3 of the Act on the status and rights of patients (785/1992), 56 it is stipulated that a patient’s mother tongue, individual needs and culture must, to the extent possible, be taken into consideration during care and/or treatment. Furthermore, a patient has the right to use, be heard in, and obtain documents containing decisions in the Finnish or Swedish language as well as the right to interpretation when using these languages or translation if the language of an authority or the language of proceedings is different, rights that are also mentioned in Sections 10, 18, and 20 of the Language Act (423/2003). 54 In Section 6 of the Health care Act (1326/2010), 57 it is also emphasized that local and joint municipal authorities shall make healthcare services available in Finnish or Swedish, with certain provisions made for whether a municipality is considered unilingual or bilingual.
Data collection – individual interviews
Individuals who had received in-patient care in a care unit at a hospital in Southern Finland received a written invitation to participate in individual interviews and were asked to directly contact the researchers. Six individuals indicated their willingness to participate in the study in this manner, and three further individuals were found through snowball sampling. In total, nine participants were included in the study. The participants chose the location for the individual interviews, and all but one interview took place in the respective homes of the participants, with one taking place in a café. The interviews lasted between 30 and 60 minutes and were digitally recorded and transcribed verbatim.
Data analysis
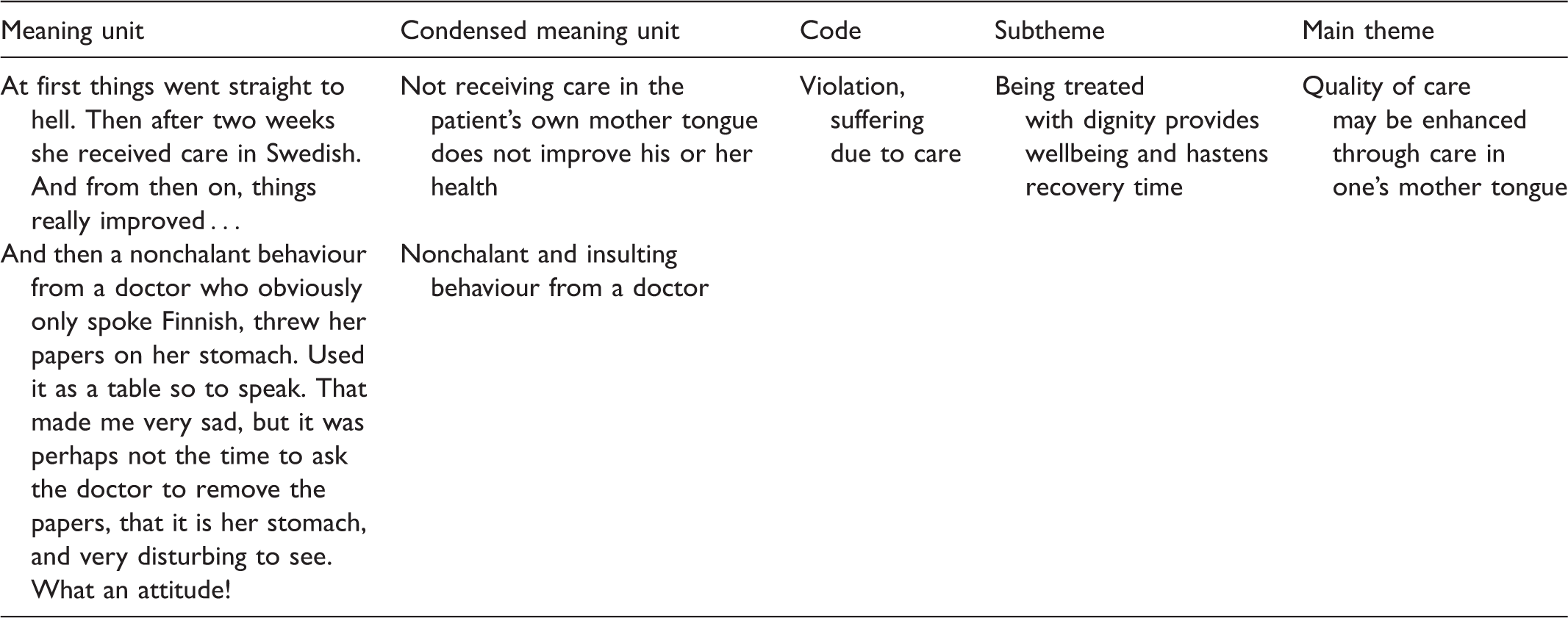
An example of the data analysis process.
Ethical issues
The study has been conducted in accordance with the guidelines delineated by the Finnish National Advisory Board on Research Ethics. 58 Ethical permission to conduct the study was granted by a hospital in Southern Finland. The participants provided informed consent and were informed regarding participation in the study, data storage, and data handling for research purposes. The participants were also informed about the study purpose, confidentiality, and withdrawal of consent. From an ethical perspective, it was considered defensible to carry out this study because it might reasonably provide participants with new insights into their experiences of care.
Results
Main theme and subthemes.

Quality of care may be enhanced through care in one’s mother tongue
As expressed in the main theme, the quality of care may be enhanced when care is given in a patient’s mother tongue. Being able to use one’s mother tongue facilitates communication, making it easier for patients to express anxiety or worry or describe feelings of pain in greater detail, which facilitates pain management. The risks associated with not receiving care in one’s mother tongue were expressed by one participant as: ‘… one misses important parts that can both make the situation worse and improve it’ (P9). Another participant perceived that when one spoke one’s mother tongue there was better contact with nursing staff and that it was also much easier to establish good contact with nursing staff, which is a prerequisite for good quality care: ‘You feel more understood and the end result is better [when you speak your mother tongue]… to be sure I have had good contact with [Finnish-speaking] doctors as well but with Swedish speakers it is always much easier’ (P4).
Being understood and understanding in a caring situation provides an increased sense of security
Being understood in a caring situation is an important condition for feeling safe and for preventing care errors. When ill or weak, patients may find it difficult to communicate in a secondary language, and miscommunication can result in patients feeling unsafe or the occurrence of care errors. One participant mentioned an emergency healthcare situation, where he as a patient waited several hours for a doctor who spoke his mother tongue to come to speak to him. While waiting for the doctor there had been several misunderstandings and the patient, not understanding what was happening, began to panic and feel as if he were receiving inadequate treatment: I had misunderstood the situation. It was later revealed that I had a [blood clot in my lung] and they talked a lot about how it went through the heart and so on. So I misunderstood where it was. (P9) I felt very weighed down by this, very sad. The circumstances of the illness had already made me nervous and then not understanding what was going on … it tends to make you a little nervous. Not understanding everything does not exactly make you calm. (P9)
The participants maintained that when they were ill or in critical condition, they often lacked the strength to actively demand good care, because they were in a vulnerable situation and did not wish to compromise their relationship with nurses by insisting on care in their mother tongue. One participant mentioned that language problems lead to her feeling unsafe and becoming worried about the quality of care she received: … being in a vulnerable situation such as in the hospital you do not want to make your position worse in relation to doctors and so on. I felt unsafe and it was not like they were mean or anything, but you know that they do not really want to speak [my mother tongue, Swedish] and if they have to do it in certain situations you wonder if they do their best or not. (P9) It is always a question of a sense of safety, and certainly it to be sure gives you a greater sense of safety if you know that you can communicate in your own language. (P5)
Being allowed to be oneself eases the patient’s cultural existence and strengthens communication
It is important that patients be allowed to be themselves and experience mutual understanding in the caring situation. The participants equated the experience of being allowed to be oneself with a sense of relief and feeling of satisfaction that in turn eased the patient’s existence. The participants also mentioned that not needing to translate words associated with their condition allowed them to fully focus on themselves and own feelings of, e.g. pain. As one participant noted: Yes, relieved! You feel relieved. And when you are ill you want your mother tongue even if you know the other language equally well, but at that time you want care in [your mother tongue]. It feels good. (P3) Yes, and it is not just a question of words, but our whole culture, what we do not express in words but still communicate to each other. (P1) A thorough discussion is easier in your mother tongue and it is easier to remember to raise specific issues [about your health] in your mother tongue. (P4)
Being treated as equal decreases suffering related to care and gives the patient strength
Perceiving that one is treated as equal in the care relationship is important, because it decreases suffering related to care, and being able to speak one’s mother tongue helps create the sense that one is ‘equal’. The participants expressed that they could experience a sense of inequality in the care relationship when using their mother tongue, if this coincided with them expressing themselves using the minority language. Patients whose mother tongue is the majority language or who possess sufficient proficiency in the majority language can ask more questions, discuss the care situation in more detail and enquire about alternative care methods. When nurses speak their patients’ mother tongue they demonstrate dignity, even if their language skills are somewhat lacking, which in turn can instil patients with a sense of calm and safety: Then I would say that you become much calmer just by receiving that understanding, that, OK, I do not know much [of your mother tongue] and you do not know much [of my mother tongue] but that we try to get it right is important. (P9) I have sometimes encountered doctors who wanted to practice their Swedish with me and this shows a positive attitude, but it comes to nothing and then I switch to Finnish. (P1) … to be treated as ‘difficult when you come here and speak Swedish’ does not make things better. And then you start to wonder if you have a big problem or what is the cause. (P9)
Being treated with dignity provides wellbeing and patients feel they recover faster
Receiving care in one’s mother tongue increases patients’ wellbeing and decreases recovery time. When nurses speak their patients’ mother tongue, they see each patient as a whole human being and demonstrate kindness and dignity, which can positively influence patients’ recovery because patients then experience that they are seen. Care in one’s mother tongue results in fewer misunderstandings and patients can more easily ask relevant questions, which simultaneously increases patients’ sense of being treated as equal. The participants maintained that receiving care in one’s mother tongue also affected how they experienced their hospital stay and could make them more positively disposed toward care. When patients do not have proficiency in the majority language, they can experience that they are not taken seriously as individuals, which is the antithesis of person-centred care. When patients receive care in their mother tongue, how they perceive the quality of the care they receive can be influenced: I was really happy [to have a physiotherapist who could speak my mother tongue]! I met her already before the surgery, and it made my attitude toward this whole surgery very positive … It made my stay there much better. (P1) At first things went straight to hell. Then after two weeks she received care in [her mother tongue]. And from then on, things really improved … (P1) And then a nonchalant behaviour from a doctor who obviously only spoke [the majority language], threw her papers on [the patient’s] stomach. Used it as a table so to speak. That made me very sad, but it was perhaps not the time to ask the doctor to remove the papers, that it is [the patient’s] stomach, and very disturbing to see. What an attitude! (P8)
Strengths and limitations
One limitation might be the limited number of participants (nine). Strengths, however, were that the participant group was heterogeneous and the participants were willing to share their experiences in face-to-face interviews, which yielded rich data and a nuanced picture of receiving care in one’s mother tongue. Validity was ensured when both researchers first individually conducted an initial analysis and then reached consensus on the final abstraction and final analysis.
Discussion
The aim of this study was to explore the importance for patients of receiving care in their mother tongue. We found that receiving care in one’s mother tongue was connected to quality of care. Receiving care in one’s mother tongue was crucial for patients’ sense of safety and eased their cultural existence, and the realization of such presupposed nurses’ cultural and ethical competence. 28 We saw that patients’ sense of safety and trust in the care being provided increased when nursing staff accommodated patients in their need to receive care in their mother tongue, even if the nursing staff’s proficiency in the patients’ mother tongue was lacking. It is essential that nurses express themselves in a language that patients understand. 59 Patient trust in the care being provided is important with regard to whether patients accept the care being offered, and over time this can contribute to the quality of care. 18 Nevertheless, Sze-Mun Lee et al. 39 emphasized that there are risks (e.g. misunderstandings, care errors) associated with nursing staff using simplified language with patients, which often occurs with minority-language patients, and even vice versa, when patients use simplified language with nursing staff. 39
Researchers33–35 have found previously that the use of professional interpreters can generally be considered a good, cost-saving and care-improving measure and that using professional interpreters is even better than nursing staff using limited language skills. Still, we maintain that the use of professional interpreters might not be solely positive in contexts similar to the context seen in this particular study: a country with two official languages and where majority and minority language speakers are afforded equal language rights. 47 While patients can receive care in their mother tongue either via nursing staff or professional interpreters, this does not guarantee or even imply that minority-language patients then receive advanced care in their mother tongue. We maintain that the optimal situation would include the provision of care by nursing staff who are proficient in both the majority and minority languages and who possess specialized language skills. Other researchers have found that if only a few nurses or a single nurse possess both specialized language skills (context-specific and which facilitate communication with minority-language patients) and advanced nursing skills, this can affect the nurse-to-nurse care relationship in a unit. 9 We therefore recommend that arrangements be made so as to ensure that several such specialized and highly skilled nursing staff are working at all times.
We saw that the participants perceived that it could be necessary to not speak their mother tongue and instead speak the majority language used by nursing staff, e.g. when nurses’ knowledge of the minority language was insufficient. The risk of misunderstandings increases when patients use a language other than their mother tongue.18,21,60 Previous studies have shown that the more serious the illness the more important it is for patients to express themselves in their mother tongue.18,61 When there are time pressures and it is difficult to find the right words, patients can feel unsafe and their anxiety can increase. Misdiagnoses can also increase when nurse–patient communication is compromised. 61 Not being understood and not understanding can be considered suffering related to care, where patients feel unsafe, sad, shameful and alone. 62 Suffering in care can, in turn, lead to a worsening of patients’ symptoms of illness. 53 When patients feel that their mother tongue is respected by nursing staff, patients’ feelings of loneliness and alienation can decrease. We saw here that the participants often experienced suffering related to care and could feel that their rights were compromised when they did not receive care in their mother tongue. Language barriers can result in patients perceiving a person speaking another language as being terse or rude, 18 because language touches upon a significant emotional dimension and helps preserve personal and linguistic identity.42,47 The participants in this study maintained that they could experience a sense of not being equal in the care relationship when using their mother tongue and that nursing staff did not take them seriously when a lack of skill in the majority language, which the nursing staff spoke, was admitted.
Patients in Finland have the right to service in the national languages of Finnish and Swedish, in accordance with their own language (mother tongue), as emphasized in the Language Act (423/2003), 54 the Constitution of Finland (731/1999) 55 and the Act on the status and rights of patients (785/1992). 56 In the healthcare context in Finland this includes more than the right to receive information about one’s care in one’s mother tongue (often via professional interpreter), as is seen in other countries where minority languages are not granted ‘official language’ status. Finland presents a special case because of its two official languages: while Finnish-speaking healthcare staff are not required by law to speak Swedish with Swedish-speaking patients, Swedish-speaking Finns have the right to speak Swedish with all healthcare staff.54,56 Therefore, not receiving care in Swedish can lead Swedish-speaking Finns to perceive that their rights are being compromised and that they as human beings are not being treated with dignity, when they are misunderstood, not taken seriously or not treated as equal to those who speak the majority language. 47
Overcoming linguistic difficulties by using professional interpreters is, in a setting such as seen in this study, therefore problematic. Granhagen Jungner et al. 40 found that translating and transferring information is problematic, because cultural issues can lead to cultural misunderstandings and clashes. Also, acting as a neutral interpreter in a situation where a cultural link is needed is difficult, because interpreters may ‘context adjust’ their translations. 40 Moreover, Bischoff et al. 6 saw that interpreters also take into account wider cultural and political contexts rather than solely translating word-for-word. In a healthcare context, interpreters must have the understanding and ability to handle cultural divergences between staff, patients and families. 40 Bischoff and Hudelson 63 suggested that language services should be integrated into healthcare organizational routines to address any eventual problems that clinical staff may have with regard to interpreters.
The caring relationship is compromised when patients perceive that they have been treated in an offensive way, seen in this study as next of kin perceiving that they needed to ‘demand’ that nursing staff provide care for patients in the patients’ mother tongue. Patients can experience shame if they cannot speak the majority language sufficiently well, which, in turn, causes suffering related to care. Patients can also begin to question their condition and even whether they need care at all, which, at worst, can lead to hesitation in seeking help, so as to avoid language problems and shame. The harmful experience of not being treated as equal in the caring relationship has a profoundly negative effect on patients’ wellbeing and health, and nursing staff should recognize that minority-language patients are vulnerable in the caring relationship. Alpers 25 found that discrimination in healthcare occurs and that it can lead to racial and ethnic health inequities that negatively affect health outcomes.64,65
Allowing patients to receive care in their mother tongue helps preserve patients’ identities and can ease patients’ cultural existence. Patients can be themselves when speaking their mother tongue and be seen as a whole human being, which in turn strengthens communication in the caring relationship because it helps patients express themselves and their needs more precisely. When patients are allowed to speak their mother tongue, non-verbal communication is also supported and more evidently contributes to understanding. Sze-Mun Lee et al. 39 saw that non-verbal communication can easily lead to misunderstandings because, e.g. a gesture can mean different things depending on cultural context. Also, Züllich et al. 66 found that when nursing staff and patients share the same mother tongue and linguistic culture, the patients’ culture is taken into consideration and nurses’ non-verbal communication is more understandable for patients.
As seen here, speaking one’s mother tongue allowed patients to feel recognized, seen and as though they were equal. It allowed them to to experience dignity in the caring relationship, which positively influenced their recovery and improved perceived quality of care. Not receiving care in one’s mother tongue could cause discontent, worry, and a sense of feeling unsafe. Taylor et al. 31 found that when an individual is subjected to stress, he/she often finds it difficult to understand and remember instructions. Consequently, when nurses cannot speak a patient’s mother tongue, a personal and loving presence becomes even more meaningful. 62
To improve the quality of care and ensure that patients can receive care in their mother tongue, those who employ nurses should consider language skills to be an important attribute. Truong et al. 28 suggested that it would in certain instances be appropriate to hire healthcare staff from various ethnicities and minorities, because such employees can possess valuable knowledge of their own culture and consequently better understand patients from the same culture. If nurses have good knowledge of a minority language, this can imply that they also have a positive attitude toward that particular language. 37 Healthcare organizations should support nurses by organizing for them language courses in a country’s minority language, because such courses are useful in positively changing negative attitudes toward a minority language. 37
This study also shows that patients were made vulnerable and that their autonomy was compromised when their next of kin were asked to act or acted as language brokers. According to Sze-Mun Lee et al., 39 having next of kin as language brokers may be problematic in caring situations, because confidential and sensitive matters may be revealed which would compromise confidentiality and patients’ right to dignity. Also, if language brokers are dominant and excluding in their roles67,68 or ‘speak as themselves’ rather than accurately transferring information,67–69 they can have a negative effect on the caring relationship.
Receiving care in one’s mother tongue entails being treated with dignity and seen as a whole person. 62 Being included by health professionals can instil patients with courage and inner strength 70 as well as confidence and trust. 71 Respectful treatment, where caregivers are kind and create space for patients and their next of kin to participate in care, results in patient satisfaction with care. 72 According to Eriksson, 73 poor treatment or lack of eye contact may extinguish a patient’s last spark of joy. Being forced to translate or search for words in a second language is tiring, especially if one has a serious illness. Earlier research shows that even if nursing staff can only talk about everyday matters in a patient’s mother tongue, this helps create a good nurse–patient relationship. 37 Related to this, a new finding was seen in this study: that patients’ next of kin also experienced it as being tiring when patients did not receive care in their mother tongue.
As seen in the results, quality of care may be enhanced through care in one’s mother tongue. The participants clearly perceived that care in one’s mother tongue provided a sense of safety, improved communication and understanding and contributed to patients’ wellbeing and strength. Also, we saw that using patients’ next of kin as language brokers should be avoided, because this can compromise the wellbeing and dignity of both patients and their next of kin.
Conclusions
Receiving care in one’s mother tongue leads to the perception of quality of care for patients and their next of kin, and the realization of such presupposes nurses’ cultural and ethical competence. Supporting nurses’ language skills and encouraging them to use these in care are important means whereby suffering related to care resulting from language barriers can be reduced. Further research should focus on nurses’ perspectives on the significance of minority-language patients using their mother tongue in a nursing context.
Footnotes
Acknowledgements
The authors would like to thank the individuals who participated in this study.
Author contributions
Jessica Hemberg contributed to the study conception and design, data analysis, discussion, and drafted the manuscript at all stages. Emilie Sved contributed to the study conception, data collection, background and discussion.
Conflict of Interest
The authors declare that there is no conflict of interest.
Ethical approval
The study has been conducted in accordance with the guidelines delineated by the Finnish National Advisory Board on Research Ethics (2012). Ethical permission to conduct the study was granted by a hospital in Southern Finland. The participants provided informed consent and were informed regarding participation in the study, data storage, and data handling for research purposes. The participants were also informed about the study purpose, confidentiality, and withdrawal of consent. From an ethical perspective, it may be defensible to carry out this study because it might reasonably provide new insights for the participants from reflecting on their experiences of care.
Funding
The Swedish Cultural Foundation in Finland has generously provided financial support for this study.