
Abstract
It is a challenge for registered nurses (RNs) to meet children and young people who have a parent diagnosed with cancer. These children often suffer from shock, anxiety, outrage, fear and stress. Recent studies indicate that when next of kin have a professional person to talk to, their wellbeing increases. Moreover, when these children are involved in their parent’s care they also begin to trust the nurse caring for their parent. However, there is little known of how nurses respond to a child’s needs. Thus, aim of this study was to describe RNs’ experiences of encounters with children as next of kin to a parent diagnosed with cancer. A qualitative descriptive study based on semi-structured group interviews, with a latent content analysis was carried out. One theme, ‘sense of security’ including three categories ‘balanced meeting’, ‘de-dramatize healthcare’ and ‘learn from one another’ was identified. Beyond the categories, there are six sub-categories: ‘sense of insecurity’, ‘caring approach’, ‘providing information’, ‘participation’, ‘processing and follow-up’ and ‘increased knowledge’. The findings of this study highlight the importance of strengthening the RN's ability to create a caring relationship with children as next of kin.
Introduction
Having a parent diagnosed with cancer brings strain and difficult feelings to cope with for children and young people, and in turn is a challenge for nurses to meet, as part of family-centred care. 1 Parental cancer has an impact on all family members; the patient’s children included. 2 Feelings of uncertainty and loneliness within adolescents when a parent is diagnosed with cancer are risk factors that need to be identified in order to develop services for families, 3 and children of families with poor family functioning seem to be more vulnerable. 2 Long-term effects could be either posttraumatic growth or adverse consequences. 4
The main problem today is the difficulty for professionals in communicating effectively, 5 as working conditions such as time pressure and medical assessments regarding the parent’s care seem to take precedence over talking with children.6,7 Furthermore, distancing strategies are used, due to lack of knowledge and confidence in encounters with children, even though nurses open up for families to be involved in the care of their next of kin and act as a bridge between the patient and their next of kin. 8 There is a lack of knowledge in guiding parents to talk with their children, 9 as well as lack of guidance to be able to support parents regarding their children’s well-being. 1
Professionals caring for parents with cancer need to ask about the patient’s family, 10 support communication within the family 11 and involve the family in the patient’s care. 8 Parents need information in order to talk with their children, 2 and parents are an important key factor in order for professionals to be able to communicate with their children. 7 Needs of information and support amongst adolescent children are, however, poorly met. 12 In some way, there must be a sort of permission from the parents to talk with the children. 7 On the other hand, it could be that children as next of kin are not included in the nurse’s daily work, due to lack of routines, knowledge and experiences. 13
In sum, little is known about how children as next of kin react when a parent is diagnosed with cancer, less is known about how nurses support parents with dependent children and even less about how nurses respond to these children’s needs. It is therefore important to develop knowledge within this area in order to raise awareness and strengthen the nurses in their role and in their daily work with children as next of kin and their parents. The aim of this study was to describe RNs’ experiences of encounters with children as next of kin to a parent diagnosed with cancer.
Method
A qualitative descriptive study was used and a latent content analysis was performed. 14 In this study the term ‘children as next of kin’ refers to children under the age of 18 years.
Settings and participants
The participants were located at four oncology wards at a larger hospital in southern Sweden. A purposeful sampling procedure was used and initial contact was established with each ward director who received written and verbal information about the study. Information was then presented to RNs at each ward and the RNs who showed interest were contacted by the first authors. The inclusion criteria for participation in the study were: 25–65-year-old RN, with work experience in an oncology ward or similar oncology care over a period of at least two years. Exclusion criteria were: those RNs who had not encountered children as next of kin. A total of nine nurses, eight women and one man, were divided into different interview groups based on which ward they were working at: Group 1, three nurses; Group 2, two nurses; Group 3, two nurses; and Group 4, two nurses. The participants were between 26 and 43 years of age, and their length of experience as RNs in oncology care varied between two and 11 years. The RNs in each group chose the time and place for the interview. The RNs gave their verbal and written consent to participate in the study and no participant withdrew from the group interview.
Data collection
Data were collected through four different qualitative group interviews each including two to three RNs. 15 The first and second authors participated in the group interviews, one as interviewer and the other as an observer and note-taker. The author who observed was also helpful in making sure everyone spoke and now and then the observer asked follow-up questions. The group interview used open-ended questions and in-depth follow-up questions. The main question was ‘Can you tell us about meetings at the ward with children of parents affected by cancer?’. Examples of follow-up questions were, amongst others ‘What happened?’, ‘What feelings and thoughts arose?’ and ‘What did you do or say?’. In each group interview there was always someone who had an Aha! experience because of another participant’s answer. The group interviews were held at the ward where the RNs worked and lasted between 45 and 80 minutes and were conducted during October 2013. The group interviews were tape-recorded and transcribed verbatim.
Data analysis
Analysis process.
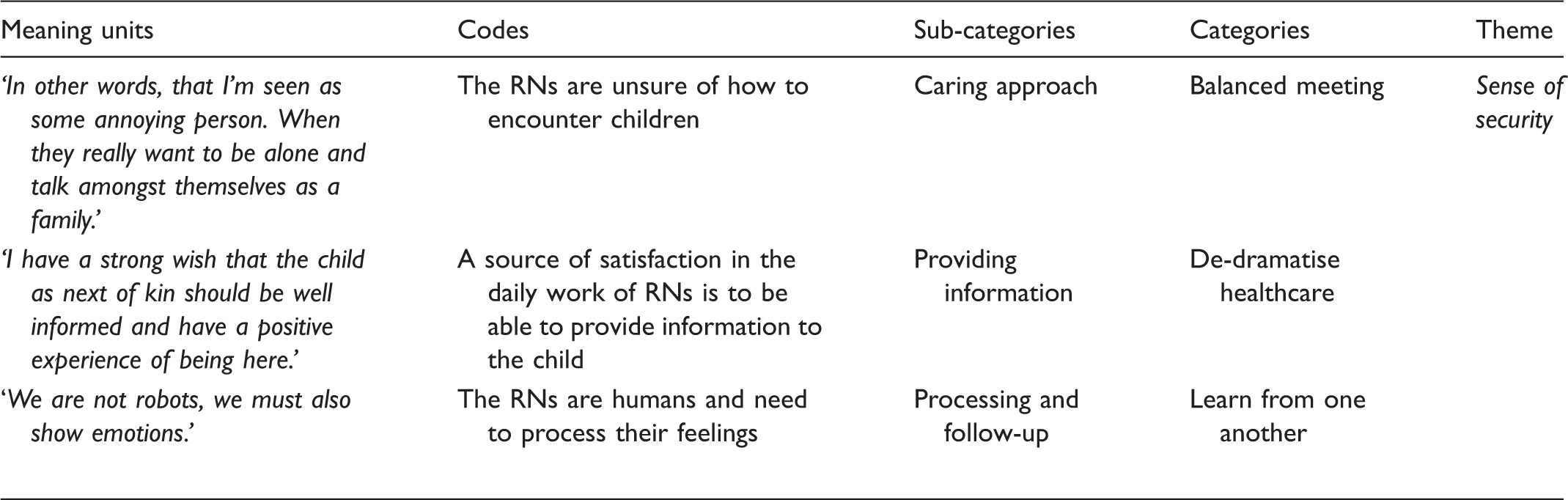
Overview of themes, categories and sub-categories.

Ethical considerations
The study was carried out in accordance with the ethical standards of the Declaration of Helsinki 16 and The ICN code of ethics for nurses. 17 The participants gave verbal and written informed consent and were informed about confidentiality. The participants were also informed of the possibility to withdraw at any time without any form of consequence. The authors had access to a professional person trained in family therapy if any of the participants were in need of support after the interview. To ensure the participants’ confidentiality, each group interview and participant was coded.
Findings
Sense of security
In order for an RN to go from a sense of insecurity to establishing a sense of security, there are needs of creating a balanced meeting, from facing personal fears of encountering children as next of kin to having the courage to open up and be there for them. Courage enables an RN through de-dramatised healthcare to provide information and invite the children as next of kin to participate in their parents’ care. This in turn gives opportunities to learn from one another and increases the RN’s probability of processing and following-up on their own feelings, leading to an increased knowledge about themselves as well as about children as next of kin, which gives a sense of security in future meetings (Figure 1).
Illustration of coherence.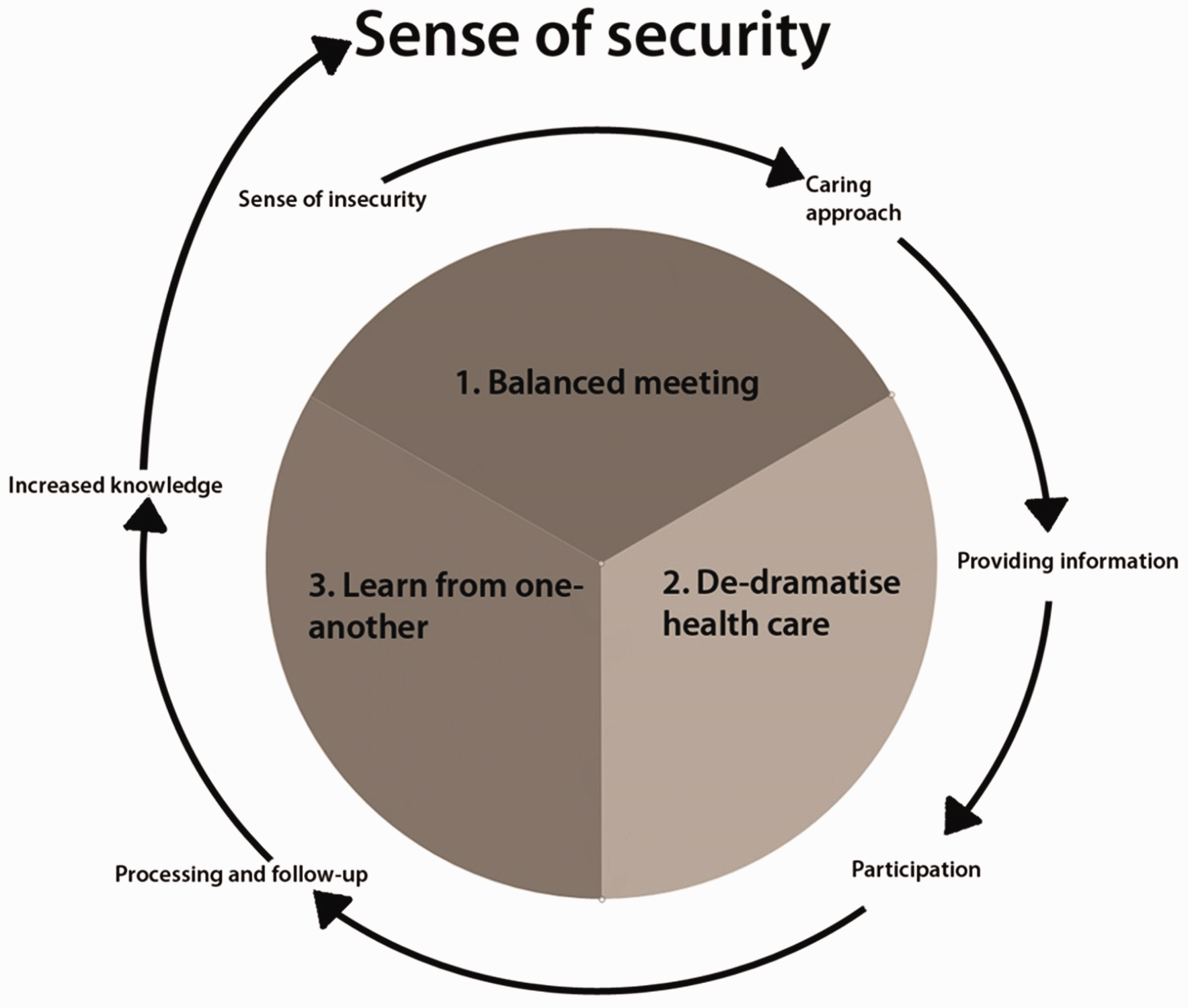
Balanced meeting
To meet children as next of kin in hospitals during difficult situations can be demanding for nurses, and very often RNs feel insecure in those meetings. The difference between what it takes to interact with children in their teens and with younger children is great and it can be challenging; even frightening. The tools needed to create a meeting come naturally to some RNs while others lack the time, experience and security. There is always a balance sought between being there for the children, and also avoiding being intrusive, especially when it comes to children in their teens. A balanced encounter with the children means to exert the RN’s professional approach, see the child, and involve the child according to their age. Through the nurse’s personal qualities, skills and professional approach, reciprocity, security, and trust can be created between the RNs and the children.
Sense of insecurity
There lies a fear and uncertainty among nurses in meeting children. They feel that encounters with children take place too seldom, and therefore that it is difficult to create a routine around the meetings. It requires a certain number of meetings before comfort arises naturally. Registered nurses fear encroaching upon a family, and fear that the family will feel burdened and uncomfortable, especially in RN encounters with children in their teens. Registered nurses often experience that children in their teens remain in closed groups and are difficult to reach. They often come to the ward for a short while and then the nurse lets them spend that time with mom or dad. They come to the department, go to the parent and close the door. It feels hard to justify going in and interfering, it is better to let them have their own time. Registered nurses also experience it as difficult to meet these teens, as they often sit with their phones and are more closed off than younger children. Notably, just because children sit with phones, that does not mean that they are not listening, but nurses experience a difficulty in entering into deeper conversation. For an RN, this gives rise to a risk of ending up in a dilemma between one’s own thoughts, prejudices and the desire to help and inform. Registered nurses also experience a lack of time in their work, which is a major contributing factor in some RNs not establishing contact with children, and this may further enhance their sense of insecurity. The nursing care of the patient is seen as most important; however, nurses realise that children can suffer emotional harm in the future if they are not able to be involved in their parent’s illness. Then I was kind of scared sometimes of the teenagers because they look at me as, who are you? I do not want to talk to you. In other words, that I’m seen as some annoying person. When they really want to be left alone and talk amongst themselves as a family. (Group 2)
Caring approach
The nurses believe that some children see all the staff as a single, indistinguishable person, while other children see the staff as individual people and create relationships. When a nurse manages to be genuine, honest and true to themselves, a relationship towards the child develops. Recurring among nurses is the desire to see the child, and to dare to create contact. No matter how horrible the disease may be, it was stressed how important it is to remind the patient and others that it is okay to laugh and joke. Just because the parent has received a diagnosis, does not mean that one should forget positive things. By daring to go in and meet the children, a nurse shows their individual personality. By affirming the children and giving them a sense of being in context, already at the next visit there is hopefully a more positive image of healthcare. Compared to teens, the nurses experience young children as much easier to meet. What I have experienced is that when you are honest and both tactful and genuine, maybe you can succeed a little bit. (Group 3)
De-dramatise healthcare
The nurses described a concern for those children who build up their own truth that can feel dark and can ultimately create a false picture of healthcare. Although the word cancer has become more common, experiences can still be charged, and feelings about cancer are transferred from adults to children and between children. By reaching out to children early, and by attempting to defuse misconceptions and involve them in the hospital’s role, their concept of truth can be more accurate.
Providing information
Although the nurses see it as a given that children should feel welcome to the ward, it seems nevertheless that the information is not conveyed well enough or is forgotten by patients and their families because there is so much else to learn about upon arrival. There are family days where the ward has an open house, which also is a way to disseminate information and remove some of the possible prejudices held by children. Yet, nurses still sometimes receive phone calls from relatives who wonder if it is okay to bring their children to the department.
In RN meetings with children, there seems to be disagreement about the sharing of information. Some nurses want to offer straight and honest communication while others choose to place the responsibility entirely on the parents. The nurses described a fear of saying the wrong thing to the children and a fear of not being able to answer the questions that could arise. There is an idea amongst some RNs that more information could lead to the children having an even harder time with the information given. A fear of providing information about the ‘wrong‘ thing to the parents in front of children is also present. The important thing is to spread out the information and try to personalise the information for both teens and younger children. The more often a nurse takes the time to provide information to a child, the greater experience it gives her the next time. One example is to go into the room to check a pending drop, mainly to show availability. Then there is an opportunity to gauge the mood in the room and see how the children’s facial expressions seem. Whether they are curious or frightened, the nurse can make adjustments and meet the children wherever they are with their feelings. The nurses also said that knowledge in asking open-ended questions of the children in order to bring out their true feelings is important; a more thought-out question can make emotions easier to express in words. By being educational during meetings with children a nurse gleans better information about the child’s well-being, and she thus satisfies the child’s current needs. I have a strong wish that the child as next of kin should be well informed and have a positive experience of being here. (Group 3)
Participation
Inviting children to participate in their parent’s illness and care creates an understanding of the situation among the children; it helps children process what has happened. When a parent spends much of their time in the hospital, it is important to show children how safe it is to come to visit. This also applies to the importance of letting the children participate in the hospital environment so that is not too alien and frightening. Guiding children to an accurate understanding and having them experience hospital care as something positive is an important role that nurses hold. By explaining and showing the children what is done with Mom or Dad, it helps children gain an understanding. It emerged that there is a difficulty in knowing when children are open for participation or when they rather would play by themselves. The nurses experienced that it was easier to de-dramatise the hospital for the younger children than it was with the children in their teens. Teens are the most difficult; they have so many feelings, one on top of another, they are dealing with boyfriends or girlfriends, your appearance is important, and when you then get a parent being very sick, the whole everyday life becomes very tough. (Group 4)
Learn from one another
As a recent nurse graduate, it is not always easy to keep emotions in control when difficult situations arise. Over time, more experiences are gathered and the opportunity to process one’s feelings occurs naturally with one’s colleagues. The work may take a long time to settle into, and it is therefore important to learn from one another.
Processing and follow-up
One way to process feelings that arise in difficult situations is to be able to cry with the children, to be able to hold them in difficult situations and to be able to laugh together. Not to take work home can be seen as both a weakness and a strength. The risk is that if a nurse closes up and does not talk through things with her colleagues, the feelings will follow her home and could become overwhelming. Nurses feel that it is easy to bring work home early on in one’s career, but after a while they realise that the feelings weigh them down too much. However, every year there are some situations where feelings are not able to stay at work but accompany one home. In those cases, it is almost always a case where a nurse recognises herself in the patient’s situation. Often it is about patients of the same age, patients who remind a nurse of someone dear to them or patients who have young children or children of the same age as the nurse’s own. The important thing is to be able to show emotions, but at the same time to have the ability to pull oneself together. Overall, the staff was described as a major support network for the individual nurse and the work climate allows plenty of space for discussing. It emerged that a follow-up dialogue can be much more open with colleagues, since confidentiality is easier to handle. Although it might seem emotionally difficult to carry tougher events, the nurses expressed that they would not want to be without them. Somehow, through their experiences, the nurses feel that they come to appreciate their own lives in a different way and not take life for granted. Some experiences are useful for other encounters as well. Some nurses, for example, talk with the children as next of kin about death so that it will not be so strange once it occurs in their own family. The idea is not to transfer one’s own belief of death, but rather to prepare for when it will happen. We are not robots, we must also show emotions, and otherwise it will be a very strange situation indeed. You have to work together, of course, but you also have to show emotion as a nurse. (Group 1)
Increased knowledge
The nurses described the importance of respecting and ensuring everyone’s areas of expertise to be able to learn and thus become a better nurse. There are many of the nursing staff in each department who are good at interacting with children and this creates an opportunity for other nurses to look at how they behave and thus gather tips for meeting with children. The nurses who have children of their own feel that it is easier to meet children in healthcare. The nurses experienced a lack of training in nursing school for meeting with children as next of kin. The information that led to the knowledge they now possess has instead been acquired through contact with colleagues. In this way, nurses have become better at meeting with children, compared with when they were recent graduates. The nurses perceive that the first period of time working as a nurse necessitates keeping tunnel vision, so to speak, in order to ensure focused medical attention to one’s patients. With time, this tunnel vision can be phased out, and children as next of kin can be met in a different way. When a patient is in a palliative stage of life, for example, nurses mentioned that they strive to make this last phase of life as positive as possible. For example, showing relatives a little extra appreciation, making oneself visible to the children but at the same time not pushing too hard. After a few meetings with children as next of kin there may even be the possibility to laugh and cry together if the nurse keeps a reflective attitude. With more experience, nurses can handle the work and learn from the emotions that arise in a more balanced way, which also creates a deeper empathy. I cannot go in and solve some huge problems, maybe, or I cannot save lives … But I can at least go in and show myself and show that I am there as a support as well … Try to find the balance where it is not to encroaching … like not run in there too much and take the initiative, but not completely disappear either. Indeed. You have to work together, of course, but you also have to show emotion as a nurse. (Group 3)
Discussion
About the method
The authors followed the criteria of trustworthiness including credibility, dependability and transferability.14,18 To achieve credibility, the participants ranged in age, work experience, different wards and gender. Consistent standpoints have been taken in all phases of data collection and data analysis to strengthen dependability. The choice was made to conduct qualitative group interviews at a larger hospital because of the collective knowledge from a large variety of different cancer wards. In each group interview there was time for participants to engage in dialogue, which also gave an opportunity for them to learn from one another and increase their knowledge. With two interviewers, one was able to register emotions, tone of voice and body language for the findings, while the other focused on what was said, which also was used in the latent phase of analysis. The choice of open-ended questions with in-depth follow-up questions was based on purposeful sampling. 14 By choosing open-ended questions, the participants were able to openly discuss each question. This ensured coverage of thoughts that otherwise may not have been brought up, as well as the possibility of asking follow-up questions. By holding group interviews, a sense of social security was provided amongst the participants and it also gave a balance in dominance. A valid group interview normally consists of four to five participants. However, if a group interview has a specific theme, the number of participants is not of the same importance, and then a group interview might consist of only two participants. 15 Another thing is that some may become silent and withdrawn in larger groups; therefore, the authors selected groups of two to three participants. Usually a focus group includes five to eight participants which could have given more variations of the studied experiences. 15 However, one thing that deepened the interviews was trust and a sense of security between the participants in the group. This resulted in an open climate where participants could speak freely about their experiences and thoughts.
All authors participated in the analysis process and discussed the findings that emerged. The manifest analysis process of reading the material at separate locations and individually was intended to ensure an objective approach because it is easy to make subjective assumptions depending on how one reads transcribed data. The use of latent analysis was made to gain a deeper understanding of the connection between emotions and actions of RNs in encounters with children as next of kin. 14 All quotations are included in order for the reader to understand or recognise the points being made, and to prove the genuineness of the study. Descriptions of the context, participants, data collection and analysis were presented as clearly as possible to address transferability. Due to the small sample size, transferability of the findings must be done with caution. It is the reader’s decision whether or not the findings are transferable to another context.14,18
About the results
This study shows that there is a sense of insecurity among nurses in meeting children with a parent diagnosed with cancer. There is an absence of guidelines and routines in involving children as next of kin in the hospital environment, 13 and distancing strategies are often used by RNs in encounters with children.1,6,7 The RNs in this study describe that they are afraid to interfere and disturb the children, thinking it is better to let them have their time alone with the parent. A key point is that the RNs in this study need to face their own fears and challenge their comfort zone, to have the courage to open up and be there for the children. Making children visible can reduce the risk of them experiencing future problems.2,4,19 This study’s nurses experienced a lack of time which is why some of them did not establish much contact with children as next of kin. Instead they focused on the ill parent. Different strategies were used towards children as next of kin; either nurses believed that the child as next of kin was not their responsibility or that the parents had the main responsibility in providing information and support for the child. It could also be that the nurses worked continuously and systematically to make the child a participant in their parent’s care. According to Golsäter et al., various ways to work with family-centred care could be used such as advising the parents on how to give adequate information to their children. Another was to enable the child to ask questions and have the sense of security to face the questions being asked. A way of enabling children to participate, if they were open to it, in their parent’s care was to give them simple tasks such as providing drinks. 20
Professionals can have difficulties in communicating effectively in their work, and nurses feel an uncertainty about communicating with and responding to children who are relatives. 5 There is an uncertainty because nurses do not have enough knowledge about how to communicate with relatives’ children.1,6 The professionals expressed a desire to acquire more education on the subject of treating children as relatives. 21 However, the more open-minded the RN is toward the child, the easier it gets. In the beginning, it is all about identifying relations and emotions within the family to be able to face them later on. 8 This study’s RNs describe that in order to earn the privilege of being invited into a family atmosphere, one must show genuine interest in being part of it, otherwise there is a possibility that the children close, emotionally. Those RNs who see time as an obstacle make it harder to develop a nursing relationship. Not showing empathy and interest in an encounter means that the duration of cancer treatment might be even harder for the patient, family and the child as next of kin. 8
This study’s RNs describe that if you are open-minded towards the importance of providing information to a child, it is easier to de-dramatise the hospital environment and for the child to feel acknowledged and included. By achieving this, there is the possibility of a child gaining a more positive attitude towards healthcare in general. However, the method of providing information and the caring approach of the RN are sometimes shown to be challenging depending on age of the child as next of kin and the sense of approachability of the RN. In the beginning of the encounter, the RN has a chance to show their personality and has an opportunity of showing empathy. 22 When this study’s RNs distribute information with a caring approach, the child receives a more honest and understandable truth. It becomes possible to face the child’s fears, by providing accurate, individually tailored information at the right moment according to the child’s susceptibility. However, if information is not given properly there is a risk that the child’s fears about the hospital environment could increase, which might harm the child’s psychosocial well-being. If children are involved in their ill parent’s hospital care, it might contribute to the child’s understanding and knowledge. 11 It is of great importance that the child feels welcome at the ward and that the information is adapted to make the child feel included.10,12
Learning how to ask a well-formulated question results in a more informative answer, which in turn lends to better comprehension of the child’s well-being. Despite insecurity, RNs in this study stated a clear difference in today’s encounters with children as next of kin in comparison to when they were recent graduates. However, they request more skill building in asking open-ended questions, which probably would give them a greater sense of security, since communication skill training increases self-efficacy in RNs. 23 When providing information to children, some RNs have a sense of fear or a sense of helplessness. 11 This study’s RNs describe how providing information with a caring approach can be difficult, and doing so while maintaining an individual perspective is even harder. The fear of making things worse by providing too much information that is perhaps not relevant to the individual may cause the RN to keep a distance from the family and let co-workers take responsibility for the situation.
This study’s RNs sense that talking about death with children as next of kin, especially teenagers, is important to prepare them when and if their parent is going to die. It is then important to provide correct information to increase their knowledge and to be supportive of the child’s thoughts and show that even if the parent passes away there is a future for the child. 22 Nurses should personally approach and show interest in teenagers and give tailored individual support to their needs.22,24 This study’s RNs describe that when a teenager has a parent who is very sick their life becomes harder, which is why it is even more important to involve them in their parent’s care. Even small tasks such as providing meals or fluids to their parent or other simple measures can strengthen the bond between child–parent–RN. 25 Younger children as next of kin often tolerate this shift differently than teenagers. 26 During the parent’s treatment at the ward it is therefore important that the RN listens to and meets children’s needs.10,12
Emotional commitment is of importance in oncology nursing, which gives satisfaction in work as well as needs of peer support. 27 The RNs in this study emphasised the importance of being able to process their emotions at work. When doing so, there is no need to worry about confidentiality, and this enables the opportunity for a more detailed description. When at home, confidentiality needs to be considered. However, by processing both at home and at work, the RNs experienced greater well-being. Emotional burdens often impact personal family and leisure activities. 11 Identifying with patients is common, which is why support and supervision are necessary, so nurses feel more comfortable in offering support themselves. 1 The ability to reflect on how to create caring relationships could be developed through supervision. 28 This study’s results show that there is silent knowledge gathered amongst RNs in encounters with children as next of kin. By having continued dialogues with each other, this knowledge may spread to others and increase their sense of security in encounters with children. The more knowledge one possesses, the easier it becomes to encounter children as next of kin. Also, a greater sense of security may result from wider dialogues, and this sense of security will make stressful encounters easier to process and follow-up on. By learning from one another and by processing encounters, the risk of emotional distress amongst RNs may reduce. By constantly reflecting with co-workers about sometimes peculiar and emotionally difficult situations, bonds are strengthened. Also, with constant reflection, one’s professional approach is being acknowledged, which makes RNs more confident.28,29
Conclusion and implications
In order for the RN to move from a sense of insecurity to establishing a sense of security, there are needs of creating a balanced meeting, from facing their own fears of encountering children as next of kin to having the courage to open up and be there for them. Courage enables the RN to de-dramatise healthcare by providing information and inviting the children as next of kin to participate in the care. This in turn creates opportunities to learn from one another and increases the RN’s probability of processing and following-up on their own feelings, leading to an increased knowledge about themselves as well as about children as next of kin, which gives a sense of security in future meetings.
The findings highlight the importance of strengthening the RN’s ability to create a caring relationship with children as next of kin. Aside from supporting parents, each RN holds an important role of giving the children as next of kin support and a sense of being in the context, which in turn would make the parents feel more secure and comfortable. Through being present and showing availability when caring for the parent, RNs will have the opportunity to choose the right time and place for personal, honest information from about the children’s needs. Inviting children to be involved in the parent’s illness and care is central in order to create an understanding of the situation and hopefully a safe haven for the children.
In order to support children as next of kin and by this also the parent, RNs need support themselves. More education about family support regarding children as next of kin to a parent diagnosed with cancer is needed for undergraduate nursing students. Organised mentoring for RNs is needed, especially for recently graduated nurses, to give them more knowledge in asking open-ended questions, foremost in relation to teenagers. A supportive network is needed at the workplace in order to strengthen RNs, foremost an organised collegial support network, in order to go from insecurity to security with a caring approach in encounters with children as next of kin.
Footnotes
Author contributions
Study design: PH, JN, CE, GL. Data collection: PH, JN. Data analysis: PH, JN, CE, GL. Manuscript preparation: PH, CE, GL.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.