
Abstract
In Norway the nurse practitioner (NP) role is still in its infancy. To succeed with implementation of this new role stakeholder involvement is important, and there should be an explicit need for change. The aim of this study was to explore registered nurses’ understanding of how the NP role could contribute to meeting patients’ needs for care in the emergency care context, and nurses’ perceptions about the implementation process. The study is a qualitative interview study. The interviews were analysed by means of qualitative content analysis. Two themes presented themselves: the NP role being an autonomous role suitable for non-urgent patients, and the NP role being diffuse as well as a threat to colleagues and organizational structures. The results indicate that the NP role can make a valuable contribution to meet current challenges in the emergency care context. However, for successful implementation, the management team plays an important role in leading change and engaging co-workers to be part of the process. In further research, it is recommended to evaluate the forthcoming implementation process and, later on, to evaluate the outcomes of NP practice in the emergency care context in Norway.
Keywords
Introduction
Emergency department (ED) crowding and long waiting times are associated with an increased risk of in-hospital mortality,1–4 a higher probability of leaving the ED against medical advice or without being seen1,4 and decreased overall patient satisfaction.4,5 Several factors contributing to ED crowding are not amenable to interventions (e.g. it is unlikely that new hospitals will be built, in-patient beds will be added to hospitals, or that acuity suddenly will decrease). 6 Therefore, effective strategies for the optimization of patient outcomes regardless of crowding status are emphasized, and nurses are seen to have a unique and valuable perspective in identifying safe and effective care. 6 It is suggested that advanced practice nursing can positively impact ED throughput, decreasing ED waiting times and/or length of stay,7–10 and have a positive impact on delivering effective and high quality care,8,11 as well as increasing patient satisfaction.8,9,11
Nursing at advanced level is included in the nurse practitioner (NP) role. According to the International Council of Nurses (ICN) NP/APN Network,
12
an NP is: a registered nurse who has acquired the expert knowledge base, complex decision-making skills and clinical competencies for expanded practice, the characteristics of which are shaped by the context and/or country in which s/he is credentialed to practice. A master’s degree is recommended for entry level.
12
In the Nordic countries, the NP role has already been implemented in some countries since the beginning of this century.13,14 However, research from the emergency care context is scarce. This study is being performed at an ED in Norway, where the NP role is in its infancy. There are in total five master’s programmes in advanced practice nursing in Norway today, with different areas of focus, i.e. geriatric, acute, emergency and family care. However, all programmes have been more or less recently implemented, and thus studies within the field are very limited (see also Henni et al.) 15 Even though there are studies on the implementation of the NP role in emergency care in other parts of the world, it is important to study the role in this new context. This especially as Norway, compared with many other countries, has a somewhat different healthcare system for patients to gain access to emergency care. Patients have to pass a ‘gatekeeper’, meaning that the first contact with the healthcare system is usually through the patient’s regular general practitioner (GP) or an emergency outpatient clinic. Thus, the vast majority of patients entering the ED have been seen by a doctor or the ambulance services, and consequently have had an initial pre-hospital assessment. 16 Further, in Norway the doctor–patient ratio is estimated to be better than that of registered nurses (RNs) to patients; a situation that differs from many other countries afflicted by doctor shortages. 17 However, there is an ongoing national discussion about medical resources not meeting the needs of the population. Further, the management team of the ED in this study have been struggling with problems similar to those initially mentioned as occurring in EDs (i.e. long waiting times and shortcomings in achieving patient satisfaction). Consequently, the management team has made a decision to invest in development and implementation of the NP role; this through taking part in the participatory action research (PAR) project ‘Providing person-centred healthcare – Development of new models of advanced nursing practice in cooperation with patients, clinical field and higher education’.
The project incorporates implementation of the NP role into emergency care in Norway. The project is founded in a participatory, evidence-based, patient-focused process for advanced practice nursing role development, implementation and evaluation, the so-called PEPPA framework. 18 The PEPPA framework recommends, in the beginning of the process, that sufficient data are to be provided to support the need for new models of care and identify priority problems and goals. 18 This is in line with recognized theories and models of leading change (e.g. Lewin 19 and Kotter 20 ). The PEPPA framework further embraces a participatory action research (PAR) approach, which can contribute to closing the gap between theory and practice as practitioners become directly involved in nursing research. 21 Participatory action research aims to enable action, and action is achieved through a reflective processes and participation of all included co-partners. The approach further emphasizes careful attention to power relationships, meaning that power is to be shared between the researcher and the researched. 22
Accordingly, stakeholder involvement is emphasized in the PEPPA framework. 18 Stakeholders may include patients, families, management, advocacy groups or government agencies, and also members of the healthcare team, as stakeholder participation at the outset is reported to be critical for ensuring commitment to and providing support for planned change.18,23 Previous literature reviews show that nurses can be critical of and feel threatened by implementation of the NP role,24,25 and that NPs themselves can initially find the role to have unclear role expectations. 25 To succeed with implementation of new NP models of care, it is thus important to explore the perceptions – both of nurses and of NPs in training – of the need for, goals and clarity of the NP role. The aim of this initiatory study was therefore to explore RNs’ understanding of how the NP role could contribute to meeting patients’ needs for care in the emergency care context, and RNs’ perceptions about the implementation process.
Method
The study is a qualitative interview study based on interviews with RNs working in the ED.
Participants
The participants comprised seven RNs (women, n = 6; men, n = 1), of whom three had attended NP training in September 2015 (interviews were performed in December 2015 and March 2016). The inclusion criterion was RNs working in the studied ED, of whom some should have initiated NP training. The participants were selected through convenience sampling. 26 The management team assisted with recruitment of participants. As there are such a limited number of NPs in Norway and the role in emergency care is new, we have chosen to reveal limited information about the participants and the setting to protect the anonymity of our participants.
Data collection
The plan was to perform focus-group interviews. That proved difficult due to high workload and sick leaves in the ED during the recruitment period. Therefore, of the five interviews, three were performed individually (interview nos. 1–3), and in two interviews the RNs were interviewed in pairs (interview nos. 4–5). The semi-structured interviews covered topics on current problems and unmet needs in the care of patients in the ED, comprehension of NP competences, the RNs’ comprehension of a feasible NP role, and facilitators and hinderances in implementing the NP role. The interviews were performed by one of the co-authors (HÖE) having experience of qualitative data collection in previous studies. The interviews were performed at the worksite of the RNs and lasted between 28 and 85 minutes (mean length 52 minutes). The interviews were recorded and transcribed verbatim.
Analysis
Description of participants.
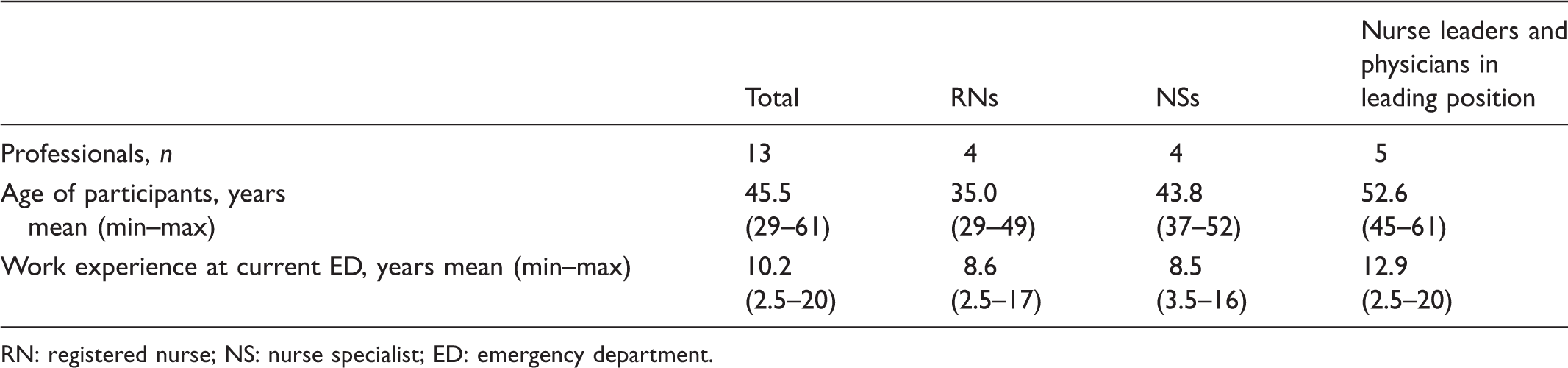
RN: registered nurse; NS: nurse specialist; ED: emergency department.
Ethical consideration
The study has been approved by the Norwegian Centre for Research Data (NSD; Ref. nr. 44387/3). In line with the Declaration of Helsinki, 28 information about the study was given (verbally), together with information about voluntary participation and the opportunity to withdraw from the study. Written informed consent was collected from all participants.
Results
Summary of the results: presentation of themes and categories.
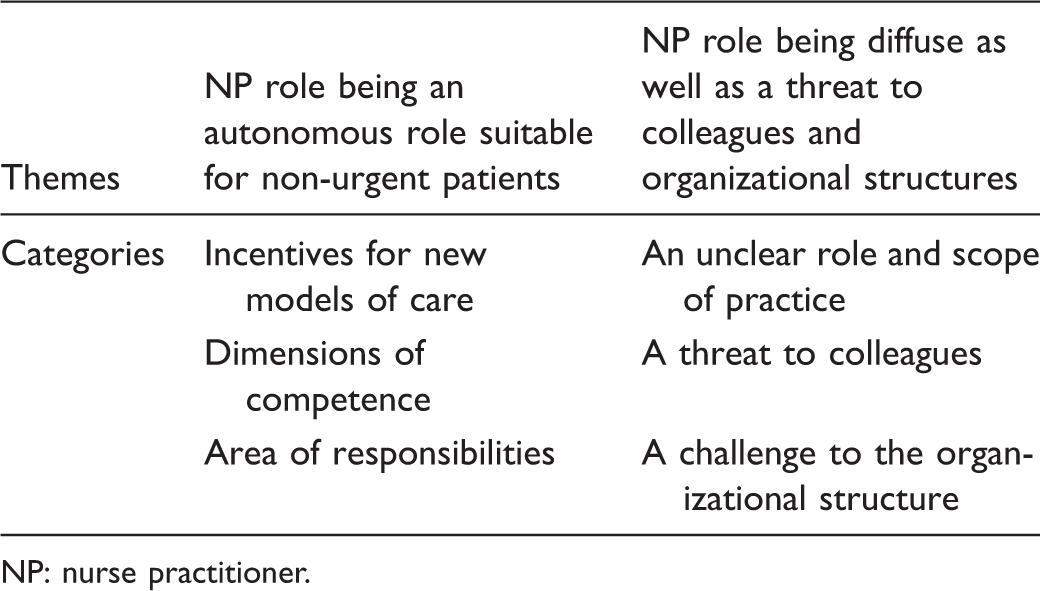
NP: nurse practitioner.
NP role being an autonomous role suitable for non-urgent patients
The theme consists of three categories. The first presents incentives for new models of care, i.e. long waiting times, patients having to tell their story repeatedly and recurrent loss of competence. The second category refers to dimensions of competence, being a mix of deepened but broad competence as a foundation for an autonomous nursing role and offering holistic care. The third category builds on the previous two categories and represents area of responsibilities, i.e. NP role being suitable for non-urgent patients, and a role that should contribute to professional development and should include supervision of co-workers.
Incentives for new models of care
The RNs said that one challenge in the ED is that as the number of patients increases, so do the waiting times. One general obstacle identified by the RNs is the accomplishment of a comprehensive assessment and confirmation of a care plan. In general, an RN admits the patient, assesses vital signs and orders/takes eligible tests (e.g. blood sample, ECG). Next, the patient is seen by a junior doctor who makes a medical assessment. The junior doctor may in turn need a second opinion from a senior doctor. All these steps, presupposed to be carried out in the order mentioned, may contribute to prolonged waiting times. In the interviews it was made clear that this procedure also obstructs admission of further patients, adding to waiting times for those waiting for assessment.
One group of patients mentioned to be especially afflicted by long waiting times were patients with non-urgent care needs, who are triaged as low priority. One RN exemplified: For patients with DVT [deep venous thrombosis] it can take years and days, become winter and spring before they are looked at. (Interview no. 4) … the non-urgent patients occupy an incredible amount of resources and time and space without necessarily needing it … also withholding doctors from doing work where they are most needed. (Interview no. 4)
Nonetheless, the RNs, in general, had a sympathetic attitude toward nurse and doctor cooperation. However, it was questioned whether it is optimal to have the initial assessment of the patients in the ED being carried out by junior doctors, who have limited experience in emergency care medicine. In addition, the placement of junior doctors in the ED lasts for only a six-month period, after which they are replaced by a new group of junior doctors. This was put forward as a recurrent loss of competence and it was remarked that this was not in the best interest of the patients and also stressful for co-workers. One RN said: It is strenuous for everyone having a new group of junior doctors every sixth months, as it at least takes three to four weeks before they get into it. (Interview no. 3)
Dimensions of competence
Among the RNs it was understood that becoming an NP means gaining a deeper understanding; it is about learning more about human physiology, achieving improved competence in observing and assessing patients, as well as in pathophysiology and medical treatment. One of the RNs expected that with the new education and previous experience, one would become able to put into words what was previously only sensed, and thus be able to identify and designate the problem, including knowing when the situation exceeded one’s own competence. It is about making the decision on what should be done, when, why and how – or not. It was declared that previous work experience is of great importance; to be able to be an excellent NP one has to have developed intuition. Competence was further related to quantity of training, and this was emphasized, this as ‘[the NPs] must be good because it is patients, it is not … this is not a playground’ as one RN put it (Interview no. 2). Nurse practitioner competence was further described as being about having broad competence, not being specialized in a specific area, but being ‘a general nurse specialist’. One of the RNs said: The traditional nurse specialist is specialist in one specific area. A nurse with NP education will hopefully have a broader competence … a broader [foundation of knowledge]. (Interview no. 1) After all, they [junior doctors] have another and much longer and more thorough education. (Interview no. 3) [NPs] should add value for the patient … if there is something that concerns the patient … many patients experience a more intimate connection with the nurse … than with other professions that focus more on the problem, the actual problem, but perhaps overlook other issues. (Interview no. 1)
Area of responsibilities
In the interviews the RNs said that NPs could have an important role in caring for patients diagnosed with chronic medical conditions, attributed with a poor general condition and complex and extensive care needs, for example, patients with cancer or COPD. These patients are seldom triaged as critically ill and are thus affected by long ED waiting times. Some of the patients with extensive care needs are also reoccurring in the ED, and the NP could have an important role to go more in to depth into these patients’ problems and hopefully prevent unnecessary readmissions.
It was also suggested that patients with less complicated fractures, minor traumas and minor medical conditions, such as DVT, could be suitable for NP care models. One RN said: As long as one is aware of one’s limitations I think NPs can do quite a lot … especially for ‘outpatients’ … waiting and waiting for a minor measure and eventually perhaps being worse taken care of by a junior doctor than by an experienced nurse, for example in need of replacement of a catheter or some stiches in a fingertip. (Interview no. 1)
With this new competence, the NP role was expected to contribute new knowledge and to supervision of co-workers to improve the professional competence level at the unit. One RN said: I think they should be used as a resource to teach what they have learnt … and I think it would be useful if there were days where … for example I could follow one of them while they teach … there is one thing to be told that one should do this and that, and another thing to learn while you are doing … (Interview no. 4)
The NP role being diffuse as well as a threat to colleagues and organizational structures
This theme consists of three categories. Firstly, there is an unclear role and scope of practice where nurses describe that they are struggling to comprehend the role and scope of practice for NPs in emergency care. Secondly, the NP role is seen as a threat to colleagues. The RNs visualize that implementation of NP models will include task-shifting between doctors and NPs, which in turn will deprive junior doctors of learning situations. The RNs also anticipate that there is a risk for downgrading of other nurses, affecting motivation to work and develop in the ED. Thirdly, the nurses foresee implementation of NP models as a challenge to the organizational structure; a structure that is understood as rigid and hard to change.
An unclear role and scope of practice
The RNs declared that even having an idea about NP models of care, the NP role and scope of practice were seen as unclear. One RN said: I have a hard time visualizing what they shall do and what authority they will have … and I don’t think anyone has tried to explain that for me either. (Interview no. 5) … one has to dear to take the discussion, to get a pragmatic debate, and discussions … also those who are uncomfortable … we cannot expect that NPs will save the world … we also have to reconsider if this is the right path to take … (Interview no. 1)
The level of NP educational degree was also discussed. A master’s degree brings about competence in research and development work; however, it requires quite a lot of effort to develop and retain such competences in praxis. There were also comments on the limited need for nurses with research competence; the majority of nurses should focus on practical patient care. It was anticipated that too many nurses with high-level academic degrees might lead to no one doing the basic nursing tasks. One RN said: There is a limitation for how many we need, because it is a matter of fact that we need to get the patients through the system … We need people who are not afraid to wash, move beds, and I see … I can already now see that it gets like, ‘No, I’m too good for that, and I won’t do that’… That is what happens … it can even be newly graduated nurses saying, ‘No, that is not one of my tasks’… No, but whose tasks are they, then? (Interview no. 4)
A threat to colleagues
The RNs said that the NP role was understood to include task-shifting between doctors and nurses as well as between RNs and NPs. Task-shifting was seen as a threat to other professions. The RNs referred to the current ED organization, having the junior doctors rotating for six months in a structured learning programme. Implementation of the NP role, including task-shifting, was understood by the RNs to deprive junior doctors of learning situations, and this was anticipated to create trouble. If you are going to move yourself into another area of expertise there will be harshness. (Interview no. 1) If I am to work together with an NP and receive an acute abdomen, I'll undress the patient and take vital signs but I should not touch the stomach because NP should do that … I wouldn’t like that. I don’t have a problem working with others, and I do want to learn, but I want to do things myself also, otherwise you lose … Then it gets totally uninteresting for me … Then I would rather be somewhere else where I can do more things on my own. (Interview no. 4) Will NPs take the most exciting tasks away from RNs? Is that morbid to say? (Interview no. 4)
Consequently, there was scepticism regarding the new role, but in the end, one respondent said that general opposition and criticism towards change does not need to be seen as negative. It means that people care about their work.
A challenge to the organizational structure
Implementation of the NP role was further understood to challenge not just other professions, but also the organizational structures. The RNs questioned whether it is possible at all to implement an entirely new role within existing – what were said to be rigid – hierarchical structures. One RN said: I’m a bit sceptical if it is possible to find a place for the [NP] role as the healthcare system is built on such hierarchical structures. I compare with the midwives, when they got the right to prescribe contraceptives, it took many years before that was accepted … (Interview no. 4) It is pioneer work, and pioneer work is hard … You first have to lift the stones, then you have to turn the soil … There is a lot to do before you can sow and plant. (Interview no. 4)
Discussion
This study is part of a larger PAR project developing, implementing and evaluating NP models in Norway; a country where the NP role is still in its infancy. This initiatory interview study in the emergency care context aimed at exploring RNs’ understanding of how the NP role could contribute to meet the patients’ needs for care and RNs’ perceptions about the implementation process. The results are understood to contribute significant information for the project as a whole, as well as for others at the beginning of the process of implementing NP models in similar contexts.
It is acknowledged that to succeed with implementation there has to be need for change (cf. ‘driving force for change’ 19 or ‘a sense of urgency’). 20 The results showed that there is a need for change, i.e. incentives for new models of care emerged. Further, the RNs anticipated that the NP role could meet some of those needs. A patient group that was brought special attention and that was assumed to be suitable for the deepened but broad NP competence, was non-urgent patients with extensive care needs, often reoccurring in the ED. It is known from previous research that non-urgent patients in the emergency care context feel that they are being given little attention and are ‘being a nuisance’, bringing about a feeling of being exposed and powerless. 29 NP practice, including being responsive to patients’ needs and offering holistic and attentive care, could increase patient satisfaction and might reduce the risk of readmission, as well as reducing the occurrence of basic care needs being ignored in the dominant medical-technical culture in the ED (see also Dahlen, Westin and Adolfsson 29 and Kihlgren et al.) 30 Having NPs take on a case management role 12 could contribute to gaining comprehensive assessments and finalizing care plans, as well as avoiding patients having to tell their story repeatedly.
The results revealed that the NP role and scope of practice was found to be unclear, in line with previous research.24,31,32 Thus, this result was not unexpected, especially as the NP role has only recently been implemented in the Norwegian healthcare system. One main mission for this ongoing project is to develop new models of care, and in the spirit of PAR, to co-generate meaning and knowledge with the stakeholders.18,22 Hence, the RNs and the forthcoming NPs have an important say in the development and implementation process of the new role. However, it did not seem that the interviewed nurses were fully aware of their part in the process, but, rather, that they had an expectation that the management team should present an outright plan. Thus, in addition to gaining important information on the aim of this study, we have understood that the stakeholders did not feel included. Therefore, it is recommended to involve the RNs to a greater extent in the process, as stakeholder participation at the outset is reported to be critical for ensuring commitment to and providing support for planned change.18,23,33,34
Further, the RNs in our study expressed a sense of being threatened by the new role. Implementation of the NP role was according to the results expected to threaten the current organizational structure, including depriving co-workers of control over and familiarity with their work. This phenomenon can be viewed in the light of the theory of organizational ownership. From a psychological perspective work can be understood as being a possession (similar to e.g. a house or car). Work plays an important role in the owner’s identity, and offers ‘having a place’ in the greater whole. This ownership can emerge through controlling the target (i.e. workplace), being familiar with it and investing oneself in it. 35 The results of this study give the notion of a threat depriving workers of their psychological ownership of work, as nurses expressed concerns about how the new NP role would affect their own role (and the roles of others). Previous research shows that more experienced nurses initially may feel that NPs take over their roles as mentors and experts,24,25 and this may be an important topic to discuss in the team, in order not to end up with lack of trust and respect within the team (see Andregard and Jangland). 24 Here, the management team, and especially the nurse leaders, have an important role in leading change. If wanting a sustainable change, leaders have to invest in not only leading the process, but also in the relationships and the culture. By doing so leaders create prerequisites not only for change, but also for good patient care.23,34,36 Lastly, it is understood that implementing a new role in the hierarchical healthcare system is very challenging. It is not just about planning and starting a master’s programme; implementing a new role affects both the organization and the people working in it.
Methodological considerations
The number of participants was relatively small (n = 7). However, there are no fixed rules for sample size in qualitative studies, and similar information was reported in the different interviews, indicating data saturation (see Polit and Beck). 26 Nonetheless, it would have been interesting to have a greater number of participants to contrast NP students and other RNs. Nurse practitioner students, not unexpectedly, had a broader view of the NP role and scope of practice in emergency care; however, NP students also expressed uncertainty about the coming role.
In two interview sessions the RNs were interviewed in pairs. Paired interviewing builds on the interaction between participants and leads to the pairs filling in gaps in the narrative, 37 which can be seen as fruitful. On the other hand, a particular concern when conducting joint interviews is that one of the pair will dominate the talk. 38 To avoid this, there were sometimes specific requests for one of the pair to expand on particular responses. It was experienced that all RNs spoke and answered questions freely.
It can further be seen as a weakness that the management team assisted with the recruiting of participants. There could be a risk that RNs were chosen based on having a similar stance to that of the management team concerning the current questions. This criticism can, however, be met with the fact that the RNs had broad points of views covering a spectrum that included both pros and cons regarding the current model of care and the potential NP role and scope of practice. It can also be seen as a weakness that the description of setting and participants is rather vague; however, this to protect the anonymity of the participants.
In line with the qualitative design, the results are not expected to be generalizable. However, it is expected that the results could be similar if the study had been performed in similar contexts elsewhere in EDs in other parts of Norway and even in other Western countries.
Conclusion
The results reveal that there is a need for change in meeting patients’ needs for care in the emergency care context. The results further indicate that the NP role is assumed to make a valuable contribution to meet current challenges, particularly among non-urgent patients with extensive care needs. Nonetheless, the NP role is understood to be diffuse and a threat to other professions and to organizational structures. We encourage the management team to act on this sense of uncertainty and get directly involved in the essence of change; the management team plays an important role in leading change and involving co-workers to be part of the process. In further research, it is recommended to evaluate the coming implementation process, and later on, to evaluate the outcomes of NP practice in the emergency care context in Norway.
Footnotes
Acknowledgements
We would like to thank all the nurses who took part in the interviews.
Funding
This research received funding from the Norwegian Research Council for the project ‘Providing person-centred healthcare – Development of new models of advanced nursing practice in cooperation with patients, clinical field and higher education’ (2015–2018).
Conflict of interest
The authors declare that there is no conflict of interest.