
Abstract
As part of the Health Care Interaction project that was rolled out in western Sweden, home health nurses (HHNs) were called on as first responders to provide emergency treatment to patients, while waiting for the ambulance to arrive. The aim of this study was to evaluate the Health Care Interaction project in terms of the training and preparation of HHNs and the competencies that the nurses felt they needed to develop to feel confident in these assignments. In this qualitative descriptive study, 11 home health nurses from six municipalities that implemented the project were interviewed, and the data were analysed using content analysis. The COREQ guidelines were followed in the reporting of this study. The findings show that some municipalities did not have a training or preparation course in place, and guided the HHNs to refer to self-education material. The HHNs emphasised the importance of continuously updating their knowledge and skills through regular training. Further, feedback and reflection were considered important as reinforcement of learning.
Introduction
In out-of-hospital cardiac arrest cases, the response time can be shortened and lives can be saved by early cardiopulmonary resuscitation (CPR) and defibrillation with an automated external defibrillator. 1 A shortened response time can also be achieved by dual dispatch of emergency medical services and other professionals as first responders.2,3 The first responder on the scene arrives before emergency medical services and shortens the time between collapse and defibrillation; this improves the chances of the patient surviving, and increases the survival rate in the 30-day period after out-of-hospital cardiac arrest.1,4 First responders from various professions can often be on the scene rapidly if they are in the area, but they have to be prepared for and educated in, for example, CPR and defibrillation with an automated external defibrillator, along with other acute treatments, so that they are confident enough to provide on-scene emergency treatment.2,3 Potential first responders include home health nurses (HHNs) home care providers, and firefighters.2,3,5 However, such assignments are rather different from the first responders’ usual work and require preparedness and clear information before their implementation.3,6 The process of understanding acute situations in a pre-hospital setting can be divided into four stages: orientation, identification, exploitation and resolution.7
Home health nursing is defined as the provision of skilled nursing care to patients in their homes by registered nurses and is typically ongoing, where interventions have preceded the care with social and medical care planning. 8 In this article, the term ‘nurse’ is used interchangeably with ‘home health nurse’. HHNs are involved in long-term care, and their daily work does not involve acute situations. During long-term care, a professional relationship is formed between the nurses and patients, their next of kin, and significant others, and this relationship evolves further during future visits. 9 , 10 This relationship is positive and valuable, as it provides the nurses with a holistic view of different perspectives of the patient’s situation and allows them to provide care that is tailored to the specific needs of the patient. 11 HHNs perceive their work as complex. In fact, they believe that it is even more complex than working in acute care, because it sometimes goes beyond the use of solely technical skills. 11 To be prepared for the challenges in home health nursing, the nurses need to have good leaders, to co-operate with others, and to undergo further education in developing and improving their clinical competence. They need continuous on-the-job training in the course of their daily work; however, lack of time is a common barrier in developing competence. Co-operation and exchange of information with colleagues and other care providers is one of the ways in which nurses can develop their skills on a regular basis. 12
The project: Health Care Interaction
Health Care Interaction is a project that was introduced in a county in western Sweden during 2009–2010. 5 The aim of the project was to provide patients the appropriate level of care in the appropriate setting, by initiating emergency treatment as quickly as possible, and by increasing interaction between caregivers. As part of this project, a team comprising various caregivers, such as HHNs, emergency medical services and other caregivers, was set up, and these personnel were required to co-operate with, support and assist each other. 5 According to the protocol set out by the project, when a critically ill patient called for an ambulance, a nurse was sent out as the first responder. The nurse was assigned to assess the patient and start emergency treatment while waiting for the ambulance, so that the patient had a good chance of surviving. 5 Nurses who wanted to join the interprofessional team were required to undergo training in CPR and defibrillation, guiding principles and diagnostic skills, before they were given such assignments. The expected outcome was to decrease the waiting time at the emergency unit and, hence, potentially save the life of the patient and also reduce healthcare costs to society. The HHNs who took part in these ‘while waiting for the ambulance’ assignments reported feelings of ambivalence when managing different contexts, lack of resources and difficulty in combining these assignments with their daily work. However, the nurses emphasised the importance of acting on such calls in accordance with their code of ethics. 6 Earlier studies show that interprofessional teamwork increases the sphere of competence of nurses and enhances co-operation between professionals.6,13 However, emotional issues can arise when nurses feel inadequate or anxious about their lack of understanding of what is expected in such assignments. In a previous study on HHNs’ experiences of being on standby as first responders, the nurses reported that in order to feel safe in their professional role and in the unfamiliar situation, they needed support from other professionals in providing high-quality and safe patient care. 6 However, little is known about the preparations that HHNs underwent before they were enrolled in the project, and which competencies, according to the nurses, should be developed. Therefore, the aim of this study was to evaluate the Health Care Interaction project in terms of the training and preparation of HHNs and the competencies that the nurses felt they needed to develop to feel confident in these assignments.
Methods and design
This study was conducted using a qualitative descriptive method 14 with an inductive approach, as such methodologies are suitable for studying individuals’ experiences. The data were collected through semi-structured interviews 15 that were transcribed and analysed using manifest content analysis. 16 The guidelines of the Consolidated Criteria for Reporting Qualitative Studies (COREQ) were used when reporting this study. 17
Study setting
The setting for this study was six municipalities in a county in western Sweden. The participants were recruited from among HHNs working in municipalities where the Health Care Interaction project was implemented in 2009–2010.
Participants and recruitment
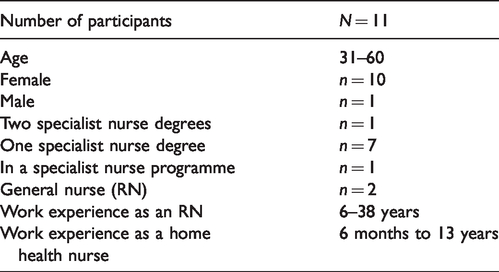
This study employed purposive and convenience sampling. 15 An invitation to participate was sent to the management of seven municipalities, with a request to the leaders to nominate two nurses for the project. After several reminders, six municipalities responded, and 11 of the nurses consented to participate in the study. Of the 11 nurses who participated, ten were female and one was male. They were between 31 and 60 years of age, and had 6–38 years of work experience as registered nurses, and six months to 13 years of experience as HHNs. One informant had two specialist nurse degrees, seven had one specialist nurse degree, one was studying in a specialist programme, and two were general nurses (Table 1).
The participants.
Data collection
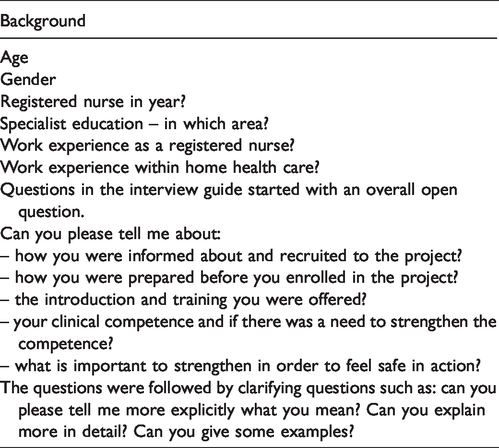
A semi-structured interview is considered as an appropriate method to gain insight into a complex problem area, such as the one being studied here. 15 To ensure uniformity, an interview guide was created and used for all the interviews. The interview guide (Table 2) contained questions about how the nurses were prepared before they were enrolled in the project and what clinical competences the nurses felt they needed to develop to feel confident about their abilities in acute scenarios. 18 A pilot interview was carried out with a resident nurse, and based on it, a clarifying question was added at the end. Individual interviews were conducted by the first author during working hours at the workplace in a quiet space that was chosen by the participants. The interviews were carried out from April to May 2017. They were audio-recorded and transcribed verbatim, and lasted between 21 and 38 minutes, with an average duration of 30 minutes.
The interview guide.
Data analysis
Data were analysed using qualitative content analys. 16 The first author was responsible for the preliminary analysis. All transcripts were first read to gain an understanding of the entire dataset. The next step was to identify the meaning units that addressed the aim of the study. In order to give the derived data better structure, meaning units with similarities were sorted into condensed meaning units. In this way, the units were condensed but their meaning was preserved. The condensed meaning units were labelled and sorted into codes. After the material was coded, all three authors participated in the analysis process. Eventually, consensus was reached, and two main categories, which encompassed sub-categories, were identified: Lack of a common structure for preparation and Developing clinical competence.
Ethical considerations
Permission to interview HHNs was granted by the management in the organisations in seven different municipalities. The leaders were asked to recruit two nurses from each municipality. Despite several reminders six municipalities answered and named 11 participants. The ethical considerations for this study were based on Swedish law 19 and the guidelines of the Swedish Research Council. 20 The ethical matters concerned the integrity of the data, self-determination of the participants and confidentiality of their data. Participants were informed about the details of the study, the method to be used, the risks involved, who was responsible of the study and their right to withdraw from the interview at any point without any explanation. The participants provided their informed consent in writing before the interviews were conducted. They were informed that the interviews were only to be used for the purpose of this study, and that the data would be stored in a safe place that was monitored by the university. The transcribed interviews were coded according to the codes assigned to the participants (P1 to P11) to guarantee anonymity. However, the interviewer had the key to the codes, so that they could connect with the participants and access the transcribed data in case some clarification was required. The transcripts were deleted after the thesis was approved. Furthermore, the participants were informed that the findings of the study would be published as a scientific paper.
Findings
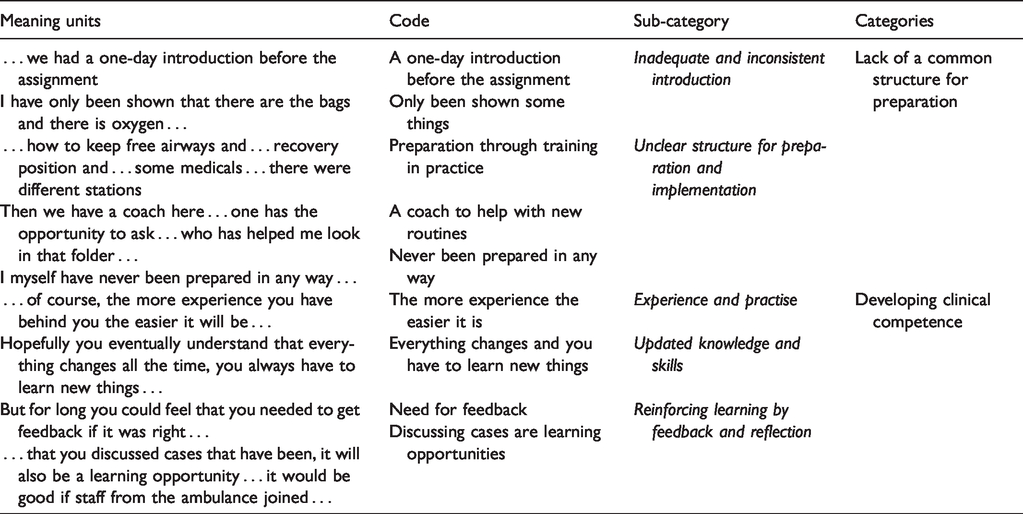
The findings from the interviews were summarised into two main categories: Lack of a common structure for preparation and Developing clinical competence, with their belonging sub-categories (Table 3).
Nurses’ views on taking part in the project Health Care Interaction.
Lack of a common structure for preparation
The category Lack of a common structure for preparation mirrored the participants’ views about how the introduction to the project differed between workplaces in different municipalities and about the lack of a common structure and routine. In some municipalities, the preparation was well organised, while it was non-existent in others. Importantly, the participants mentioned that they were not included in the decision-making process for participation in the project.
Inadequate and inconsistent introduction
The sub-category ‘Inadequate and inconsistent introduction’ reflected the participants’ view that some municipalities had a good introduction as well as organised preparations before the project was started. The length of training differed between the workplaces, and lasted from one day to three days. This was managed by a supervisor or by personnel working in interactional care. The participants were verbally informed about the project, which assignments would be included, and guidance and routines. Apart from the verbal information, written and online information was also provided. … on the training days we got the more detailed information … eh what the different types of assignment meant … (P1) … you need … to go through the guidelines … or the treatment guidelines with someone who has more experience in using them … (P6) … I got oral information from our leader, and I got to read the existing documents, I was shown the homepage where one could read about the assignments. (P3) … I myself have never been prepared in any way, I have only been shown that there are the bags and there is oxygen … (P5) … there was never anyone who asked the nursing team what they thought about it. (P1) … and we [HHNs at the workplaces] felt very strongly that we were forced, because we did not want this from the first beginning … (P9)
Unclear structure for preparation and implementation
The sub-category ‘Unclear structure for preparation and implementation’ reflected that the project required the institution of new routines at the workplace, but there was no clear structure in their implementation. In some workplaces, coaches were given the responsibility to educate personnel, to act as supervisors, to care for and control the equipment to make sure it worked, and to be the point of contact for the project. The presence of the coaches promoted confidence among the HHNs. We have two coaches here and they are responsible for the medicines and ensure that there is enough material and order more material and do such things. (P8) … and we had to work out a schedule, who have the ‘while waiting for the ambulance’ assignments and that rotates in the group … (P3) … it’s not the case here that we’ve got a new employee to facilitate [due to the project], absolutely not. (P8) Training in how to keep free airways and … recovery position and how to administer some medicines … there were different stations. (P7) I had to read through covers and documents and take a quick look at the equipment what there was to be found. (P3)
Developing clinical competence
The participants described the importance of ‘regularly updating their clinical competence’ in order to provide high-quality and safe patient care when taking on their new roles. They also described the need to continuously maintain and develop their clinical skills. They emphasised on the need to have accurate knowledge and skills, both in theory and practice, in order to be able to act efficiently and with confidence.
Experience and practise
This sub-category highlighted the need for ‘experience and continuous practise’ in order to develop and update technical skills and have up-to-date knowledge, as this would help them feel confident. The participants noted that there were long intervals between the assignments that might cause feelings of uncertainty. Therefore, regular training for the skills needed to develop routines for the assignments should ideally be arranged. … education means a lot [to develop routines], but you have to have assignments otherwise … you forget (P1) … of course, it will be so, the more experience you have behind you the easier it will be … (P10) … that you are a group from different home care units training together with the ambulance and … possibly others who should attend … (P7) … its obviously your own responsibility to read the guidelines, but sometimes, you need someone who knows more … (P6)
Updated knowledge and skills
The participants emphasised the need for ‘updated knowledge and skills’. The participants articulated the need for deeper knowledge about emergency treatment, that is, more expert knowledge than what they used in their daily work. This meant that they constantly tried to broaden and deepen their knowledge and skills, in order to better perform the procedures. Yes, but it would be good to have [regularly] a kind of a ‘refreshment day’ obligatory for everyone … or some kind of regular [training] … in which you went through everything again. So that you all the time feel that you’re updated. (P2) … yes, a couple of months ago we did a written exam … I think that was very good because many things were brought up then … I think that was evolving … (P7) Hopefully you eventually understand that everything changes all the time, you always have to learn new things … (P5)
Reinforcing learning by feedback and reflection
This sub-category describes the need for ‘reinforcing learning by feedback and reflection’, which highlights the need for feedback on one’s performance and achievements in order to develop professional skills. The participants asked for professional opinions on their performance, and they were also curious about the effects of the given treatment. … but only some kind of feedback that you thought in the right paths so that if you are wrong, you do not the same mistake again next time … (P11) … there is a need to reflect on exactly what has happened in the situation and if there are just one or two persons at my workplace, as it usually is, well then the reflection will be somewhat thin … (P5) … that you discussed cases that have been, it will also be a learning opportunity … it would be good if staff from the ambulance joined … (P6)
Discussion
The aim of this study was to evaluate the Health Care Interaction project in terms of the training and preparation of HHNs and the competencies that the nurses felt they needed to develop to feel confident in these assignments. The everyday work of these nurses is rather different from the responsibilities they have as part of the project, Health Care Interaction. Home health nursing is characterised by long-term care and long-lasting relationships built by the nurses with the patients and their informal caregivers. It is, therefore, important that they are well prepared for the new assignments and that they develop the clinical competencies which will help them feel confident in acute situations, which are new for them. The data collected from the semi-structured interviews conducted in this study implies that the training and preparation courses for the nurses before they were enrolled in the project varied across municipalities, and some municipalities did not provide any preparation or training before recruiting nurses for the project. This raises some questions about the quality of care and, above all, about patient safety, as an early, comprehensive introduction is crucial for the implementation of new routines and strategies. Another important finding that emerged was that the nurses were frustrated about not being included in the decision-making about their participation in the project. The decision to enrol in the project was not made by them; instead, they were ordered to take on the ‘while waiting for the ambulance’ assignments. This raises some ethical questions about the actions of the management and the work environment.
The nurses who were interviewed as part of this study also stressed the need to receive regular feedback and to engage as a team in reflecting on their experiences, as this would help them to learn more and develop their professional competence. The nurses emphasised the importance of feeling confident in their work in order to be able to provide high-quality and safe patient care. They felt that in order to feel confident, one also needs to have both accurate knowledge and good technical skills. Thus, the nurses considered regular feedback, evidence-based practice, access to updated information, and reflection to be important. However, according to the present findings, these elements are overlooked by the organisations. Thus, this is an aspect that needs to be in focus in the future.
In order to combine new assignments with everyday work, nurses need to widen and deepen their clinical competence and work efficiently in co-operation with other professionals.6,13 For developing clinical competence, it is essential to have both theoretical knowledge and an opportunity to apply it in practice. 21 Unfortunately, the findings of this study showed that the nurses experienced few ‘while waiting for the ambulance’ assignments, and this made them feel unsafe. 22 In order to provide efficient and safe patient care, nurses put a lot of effort into training, as shown in earlier studies.23,24 In the context of the current project, regular and structured simulation-based training would complement other training for skills development. In agreement with this, earlier studies have also concluded that simulations provide a safe and sound way of testing and developing professional competence in interprofessional teams.24–26 The nurses in this study expressed the need for training and simulation to develop their professional competence and to reflect on both real-life situations and training situations. 27 Reflection is necessary to gain an understanding of what happens in an acute situation and possible ways to enhance the outcome. 28
This study showed that feedback and reflection are two essential elements in promoting the development of professional competence. However, these elements are often missing and are not given enough attention, and the support provided for the HHNs seems to be unorganised. This means that learning opportunities are often lost. Accordingly, earlier research suggests that developing professional competence and feeling qualified and confident when on duty require repeated training, education, reflection and feedback.6,29,30 In fact, there is evidence that structured feedback, reflection and learning are all associated with competence in integrating theory and practice, building confidence at work, and positive changes for professional competence.22,31–33 The nurses in this study have a reflective attitude, which is connected to their strong will to develop professional competence as in earlier studies.27–29 They wish for more space for reflection in the workgroup and as part of the emergency medical service. This is supported by earlier research which explains that the participation of experts can deepen the level of reflection and knowledge.28,29 Apart from co-operation and reflection with interprofessional teams, feedback on the nurses’ achievements is another important aspect in the development of professional skills.12,30 However, organising feedback and reflection sessions is the responsibility of the management, which must allow and enable more space for these as structured and planned activities. 27 Structures to inspire the development of professional competence are important, as these can get the staff more involved in further development and sharing of knowledge. 27 Sharing experiences and knowledge with each other is a way to develop not only one’s own competence, but the whole team’s competence as well. 27
Methodological strengths and limitations
This study was conducted using a qualitative descriptive design with an inductive approach. 15 , 16 This approach was suitable because we wanted to capture the experiences of the participants, and descriptive design tends to stay true to the data and events. The methodology is therefore one of the strengths of this study. A semi-structured interview guide with open-ended questions was used, 18 and the participants were encouraged to narrate their experiences. The interviews were carried out in a quiet space at the workplace during working hours, and the participants willingly talked about their experiences and provided rich material. Individual interviews and qualitative content analysis were also suitable methods in this study, as the focus was to identify meaning units from the participants’ narratives. Several quotations are included to ensure the transparency and trustworthiness of the study. The categories and sub-categories and description of the process and how the overall categories and sub-categories were developed were discussed and agreed upon by all the researchers which promoted objectivity. 15 , 16
Further, the relevant ethical guidelines were carefully followed during the whole process. 19 , 20 Thus, the stringent protocol followed is also a strength of this study. However, one of the limitations might lie in the fact that the leaders of the seven municipalities were asked to nominate participants. This might have caused a bias, as the leaders may have chosen participants who had a positive view of the project. Despite this, the findings reveal both positive and negative experiences. Although the majority of informants were specialist nurses, their competence was not sufficient to provide acute assessment and emergency treatment. Another limitation is that only one male nurse participated. On the other hand, this reflects the gender distribution in the field. Despite these limitations, the findings can be transferred, with some caution, to other contexts at the national and international level. This is because clinical competence needs to be developed in all contexts, and feedback and reflection seem to be powerful tools. 15
Conclusions and implications
The findings of this study show that to be able to perform well as part of the Health Care Interaction project, nurses need to improve their clinical competence through regular training in acute assessment and emergency treatment. To this end, it is highly important that municipalities and workplaces develop a common and well-structured programme for introduction and preparation before the new routines are implemented. The nurses show great responsibility with regard to keeping up with technical skills and deepening their level of competence so as to be able to provide high-quality and safe patient care. Furthermore, the nurses emphasised the importance of receiving feedback so that they could evaluate the outcome of their actions. Another point they emphasised was reflection together with a coach and an interprofessional team. Thus, a coach or supervisor should be appointed at all workplaces to support the nurses. Simulations are regarded as a good way of staying updated and practicing the required skills. The management is responsible for safe patient care and, thus, also responsible for ensuring that the nurses are well prepared before taking on these emergency treatment assignments. The goals for the future should be to develop a regulated and structured introduction programme for the nurses and to create space for reflection and feedback in everyday work. Further research is needed to understand how reflection and feedback can be part of the daily work of nurses.
Footnotes
Author contributions
This article is based on a master’s thesis by CF who is the first author. CF has been supervised through the whole process by YH and L-LJ. CF has been responsible for collecting and analysing data and for the draft of the manuscript. Both supervisors, who are senior researchers, have participated in the analysis process. The supervisors have taken an active part in commenting on the draft and made substantial revision of the article. All authors are in agreement of the content of this article.
Acknowledgements
Carina Fjällman wishes to thank Fyrbodal Association of Local Authorities for financial support and her employer Mellerud municipality for the possibility to perform this study. All authors thank the home health nurses who participated in this study and thus made it possible.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
Fyrbodal Association of Local Authorities gave financial support for this study.