
Abstract
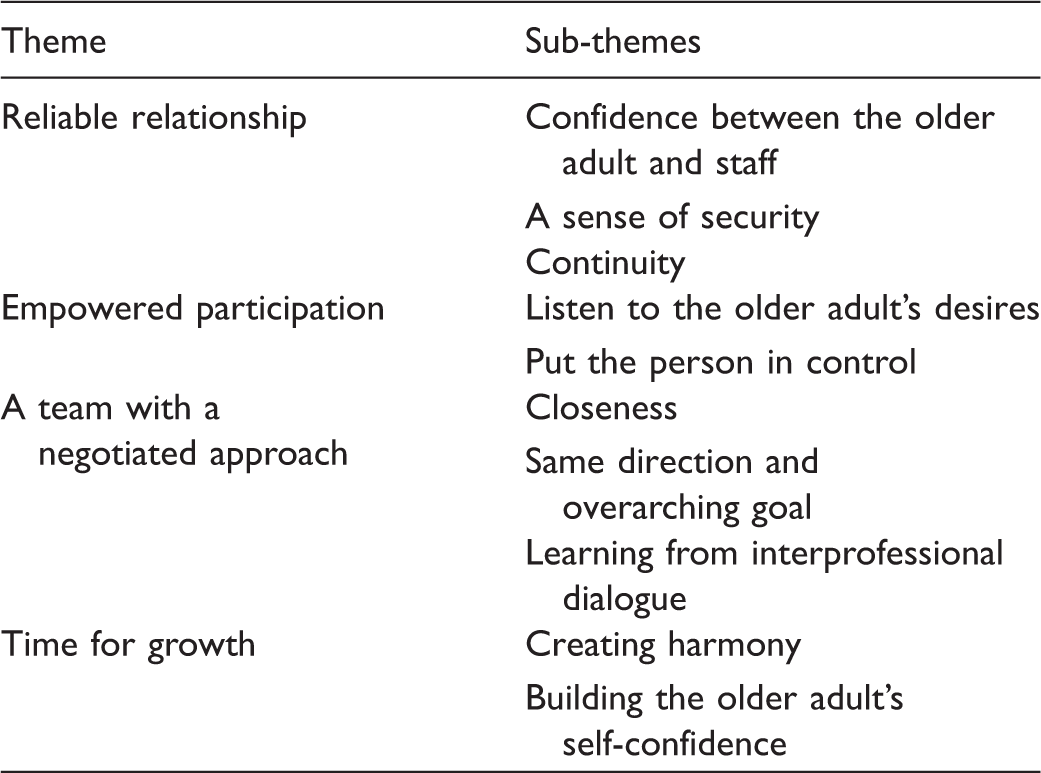
The increased number of older adults who experience longevity requires increased investment in healthcare services. Short-term goal-directed reablement is expected to strengthen the functional capacity and quality of life of older adults, while homecare hours, and thus municipal expenditures, decrease. Facilitation of successful interprofessional collaboration includes not only enhancing coordination structurally, but also establishing a commitment regarding culture that overcomes professionally differentiated attitudes. Nurses have an obvious role in these multi-professional teams and the study explores some aspects' of working in this type of collaboration. The aim was to illuminate the meaning of working with short-term goal-directed reablement of older adults as experienced by an interprofessional team. Data were collected after an intervention with goal-directed time-limited reablement of older people. Written narratives from an interprofessional team were analyzed using a phenomenological-hermeneutic approach. Findings identified four major thematic structures that characterized the meaning: 1) Reliable relationship; including the aspects ‘Confidence between the older adult and staff’, ‘A sense of security’ and ‘Continuity’, 2) Empowered participation, including the following aspects: ‘Listen to the older adult’s desires’ and ‘Put the person in control’, 3) Team with a negotiated approach, including the aspects: ‘Closeness’, ‘Same direction and overarching goal’, ‘Learning from interprofessional dialogue’, 4) Time for growth with the aspects ‘Creating harmony’ and ‘Building the older adult’s self-confidence’. The process of reablement seemed strengthened by the collaborative approach of different professions and their combined efforts. The present study argues that teamwork gives confidence both in terms of general knowledge of reablement but also specific confidence in one’s profession.
Keywords
Introduction
The increased number of older adults who experience longevity is a positive development, but it also means higher requirements on homecare and reablement initiatives. General policy goals state that older adults should live independently and have an active and meaningful existence in a community with others. Previous reports show that reablement has a good effect on municipal economies in the form of reduced hours of homecare.1,2 However, there is not enough research focusing on the professional’s perspective regarding the meanings of short-term goal-directed reablement from a multi-disciplinary view on health, described by the care staff working with these new interventions. Municipal home healthcare is a growing field of interest for nurses. More and more patients are staying at home or being sent home from hospital in an earlier stage in recovery than before, which requires more and more multi-professional cooperation in order to manage this growing challenge. Nurses have an obvious role in these multi-professional teams. This article explores some aspects' of working in this type of collaborative team that could be used to widen the picture of how this is experienced and to know how nurses’ confidence of their profession within this collaborative approach could be strengthened. An illumination of the phenomenon can deepen understanding about working with reablement within municipal care developments and research at a national as well as international level.
Background
The National Board of Health and Welfare in Sweden 3 highlights in its report the importance of working with everyday rehabilitation, which has the goal of strengthening and maintaining the health and functional capacity of older adults. International research2,4,5 uses the term reablement to describe targeted home-based rehabilitation. Reablement interventions are sometimes used synonymously with the Danish term ‘hverdagsrehabilitering’ 1 or the Swedish concept of everyday rehabilitation and describes the purpose of supporting and assisting older people to learn or relearn the necessary skills to cope with their daily lives. Reablement refers to an intense form of rehabilitation that is limited in time and carried out in people’s homes or in assisted living. It is often inter-disciplinary and focuses on supporting people to regain the ability to perform and participate in daily activities which are decided by the older adult. 5 It must be noted, however, that the evidence regarding reablement is limited.
Older adults often have a multiplicity of age-related needs which implies that a key element is to empower and enable professional care-givers to work with person-centered care. 6 Person-centered care can be seen as an approach to practice and establish therapeutic relations between care-givers, patients and other important people in the older adult’s life. Caring is built on values such as respect for the person, the person’s right to self-determination and equal understandings. 7 Janssen, Snoeren and Van Regenmortel 8 point out the importance of interdisciplinary cooperation between professionals working with older people in community care. They describe professional cooperation as a prerequisite for providing strong and integrated care since older people living at home often face complex, multi-faceted problems that cannot be solved by one profession alone. The foundation of interprofessional teamwork can, according to Berlin 9 be seen as a) to be able to offer help to others b) to be able to receive help from other professions. Robben et al 10 emphasize that the care for older frail adults is often fragmentized, involving many professionals from various disciplines. Their study suggested a specific program with interprofessional education (IPE) and collaboration, and concluded there is a need to get to know each profession’s viewpoint, though it is known that interprofessional communication is not without problems. Norman and Peck 11 found four key reasons for interprofessional team problems in community care: loss of faith in systems within which they work; strong adherence to uni-professional cultures; absence of a strong shared philosophy; and a mistrust of managerial solutions to problems. These problems can lead to disputes about the area of practice and to mistrust of the interprofessional idea, according to the WHO’s Framework for Action on Interprofessional Education and Collaborative Practice. 12 Robinson and Cotell 13 found that successful interprofessional collaboration includes both enhanced structural coordination, and the establishment of a cultural commitment that overcomes different professional attitudes. Studies14–16 also show that different professionals who experience involved in reablement are also encouraged to interact interprofessionally.
The confidence of healthcare staff, both in their own capacity and their professional role, is crucial for the quality of care and should receive more attention. 17 Leadership plays an important role in ethical qualitative care, supplying tools, confirmation and recognition such as common space and structures for the staff to be able to act in an evidence-based way. 18 Previous research with municipal healthcare staff shows a lack of confidence in their own capacity to apply such things as evidence to their own daily work.18,19 Empowerment of healthcare staff and their influence are significant factors for such things as keeping cultures in healthcare that create high quality of care. 20 Severinsson and Hummelvoll 21 claim that factors such as time to spend with the elderly contribute to job satisfaction or dissatisfaction and are related to each nurse’s ethical system. Trojan and Yonge 22 also showed in their research that spending more time with the patient may be more cost-effective, as the patients experienced that their needs were cared for and experienced a sense of confidence. This also might lead to a situation where the patient may not enter the healthcare system as frequently.
Aim
The specific aim of this study was to illuminate the meaning of working with short-term goal-directed reablement of older adults as experienced by an interprofessional team.
Methods
The overall short-term goal-directed reablement project has a multi-method design, where a randomized intervention project was combined with qualitative studies with both older adults and staff as research persons to follow up the intervention. The intervention was a goal-directed, home-based, time-limited (three months) reablement, organized by an interprofessional team in which the controls received traditional homecare. The overall research design included measurements of the older adult’s multi-dimensional health, and the ability to perform daily activities as well as their physical ability. Measurement was performed at inclusion when the older adult applied for homecare as well as after three and six months to study the effects of the intervention. Qualitative data were collected after the intervention via interviews with the older adults about their experiences, and from personal letters from the staff. In this particular study an analysis of the interprofessional rehabilitation team’s narrated experience of the meaning of working with this type of short-term goal-directed reablement is presented.
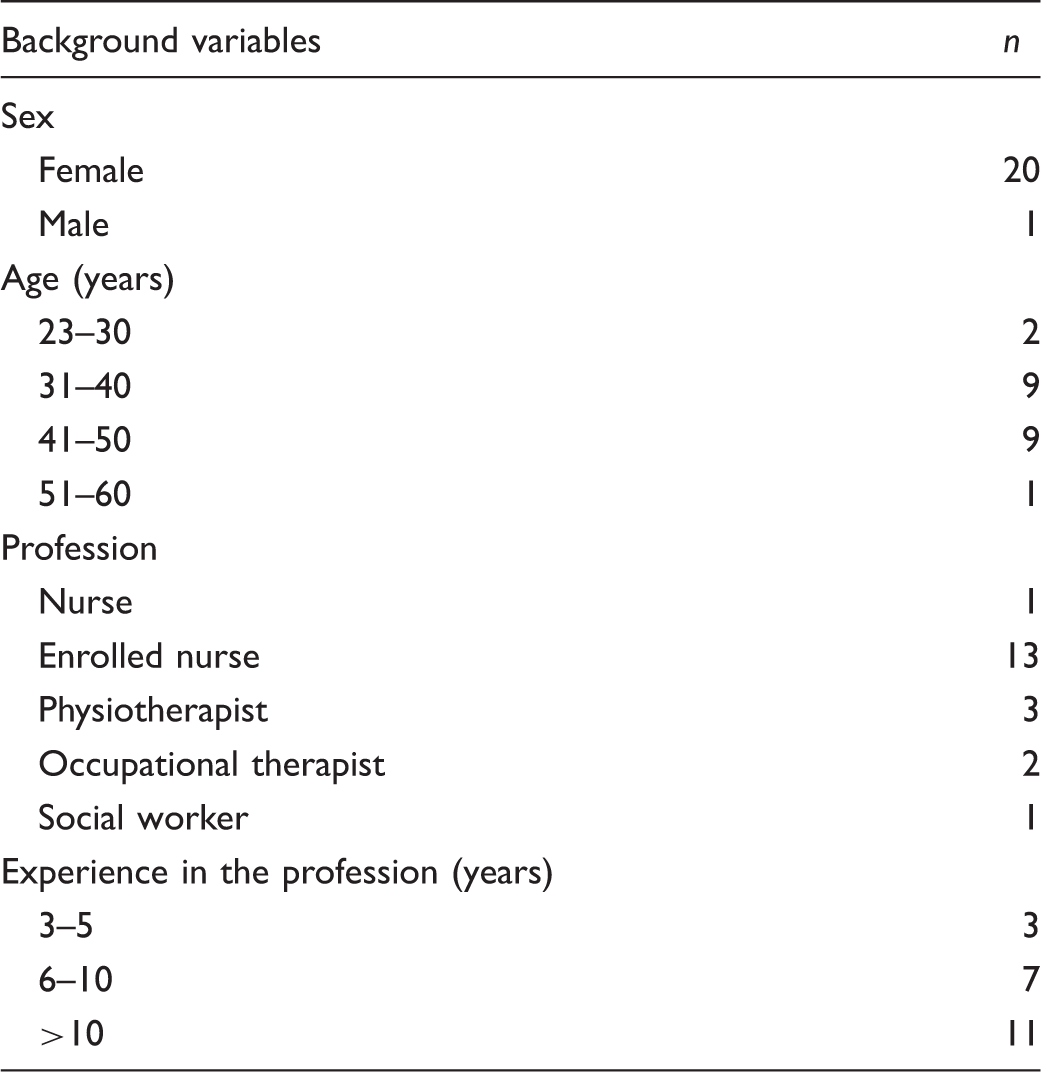
Data collection
Demographics.
Analysis
A phenomenological hermeneutical approach, inspired by the philosophy of Ricoeur23,24 was used to grasp the understandings of the meaning of working with short-term goal-directed reablement with older adults. The phenomenological-hermeneutic analysis was conducted according to Linseth and Norberg 25 as follows: a) Naïve reading of the text as a whole and initial definition of a first spontaneous guess of the common meaning – naïve interpretation, which in the next step was validated by structure analysis. Structure analysis is a way of identifying themes in the text and naming them in a way that illuminates the meaning. b) The text was split up into meaning units that contained one or more text pieces with a common meaning. The meaning units were then condensed, also termed decontextualized,23,24 and divided into sub-themes that illuminated different aspects of the main themes that were formulated as a broader understanding of the meaning connected to the aim found in the text. c) Then a comprehensive understanding was described after widening and deepening the understanding by new reading of the text including the naïve interpretation and structure analysis, together with literature and earlier research. This re-contextualization of the text offered a confrontation of different understandings and dialectic interpretation in order to promote a deeper understanding of the meaning of working with short-term goal-directed reablement with older adults as experienced by an interprofessional team.
Ethical considerations
Approval for the study was obtained through the Regional Ethics Committee in Uppsala, Sweden (Dnr, 2015/350). The staff invited were informed that participation was voluntary and that any data collected would be handled without anyone unauthorized taking part. Further ethical aspects were considered based on the World Medical Association Declaration of Helsinki. 26
Results
The staff in the interdisciplinary team working with short-term goal-directed reablement described their experiences, ambitions, and motives for performing their mutual work. The findings are presented in the order of the described methodological phases of phenomenological hermeneutics to make the process of interpretation as visible as possible.
Naïve understanding
Through naïve understanding, the meaning of working with short-term goal-directed reablement with older adults as it is experienced by an interprofessional team means the creation of a Reliable relationship with the older adult that incorporates the person’s Empowered participation. The reablement is given by a Team with a negotiated approach, it has clear goals and includes time for growth.
Structural analysis
The meaning of working with short-term goal-oriented reablement with older persons.
Reliable relationship
The relationship with the older adult, according to the team members, was characterized by confidence, security and continuity. The staff emphasized that the creation of a trustworthy, dependable, and continuous relationship facilitated reablement work.
Confidence between the older adult and staff
The team members compared short-term goal-directed reablement with traditional homecare and described the importance of developing reliable relationships with both the older adults and their next of kin. The team created quite close connections with both the person receiving care and their spouse or engaged relatives, depending on the number of daily visits. The degree of trust the older adult had in the team members gave them sufficient power to look after the interests of the older adult. Few nursing staff with high continuity make us quickly build up a mutual trust and a reliable relationship to both older adult and their next of kin. We then build up a trust that makes the older adult rely on us quicker than ordinary homecare staff. A reliable relationship with trust is then created.
A sense of security
The team experienced that the older adults were able to get a sense of security because the team had the ability to really listen in a way that seldom takes place in traditional homecare. The team could be there for the older adult in a calm way and take their time training them on specific skills, not frightening or pushing the person too much. However, there could still be a risk that the person would experience stress if movements were pushed for that they were not ready for. I think we are experienced as more calm and more secure, we listen and have the time to sit down. I create a feeling of safety related to the older adult. He or she knows they can turn to me if they wonder about anything.
Continuity
Since the team worked with fewer older adults they were granted more hours of care. Implementation of the intervention resulted in personnel continuity being much higher than for ordinary homecare. Repeat visits to the same older adult were described as helpful in creating a caring relationship, and being able to attach and involved in different levels. Working with a smaller group of older adults gives the possibility to create a caring relationship and the possibility to work on different levels of the person’s life. By performing continuous visits one has the preconditions to create a good relationship and as a result the possibility to follow up in time, adjust and change if necessary.
Empowered participation
In relation to the reablement process, the team underlined the need for the older adult to be engaged and empowered in her or his own participation. Empowered participation was supported by listening to the older adult’s wishes, and giving the person control over goals and activities in the reablement process.
Listen to the older adult’s desires
The staff described the necessity of listening to the older adult’s own desires to find out their personal needs and wants. In traditional homecare, it is the group leader or planners who make decisions on the older adult’s behalf and guide the staff activities. According to their descriptions, the staff often felt that they had no control over their care work under such conditions. The staff expressed a changing situation, which promoted concentrating on meeting the older adult’s needs and goals rather than keeping the schedule as decided by others. I listen to the older adult and allow it to be their personal wishes we are working from. To be able to work at a calm working pace with all these good conditions make us staff feel that we have the time to meet the older adult and all their needs and should be able to always positively meet their requests. My experience is that I work in a different way and this is better for the older adult. Earlier I was thinking how I could compensate for care and now I think more about activities and rehabilitation. I ask the older adult in a more detailed way what is important for this person and what goals they want to achieve.
Put the person in control
In order to contribute to progress and reablement, the staff emphasized the importance of the older adult being in control of decisions and actions in their everyday lives. The relationship with the person was more on the older adult’s terms putting them at the center of decisions and their wishes as the main driver behind the team’s ambitions. The older adults participate more in their daily living, in everything from time-schedules to decisions about ending granted actions. For the person the team [presence] means safety, being able to be seen as an adult and to direct their own future towards independence.
A team with a negotiated approach
This thematic structure is about interprofessional relationships and their outcomes. Working full time in a team with a negotiated approach was not something any of the team members had done before. Their descriptions about team cooperation focused on team closeness, working with the same overall directions and the opportunity of learning from an interprofessional dialogue.
Closeness
When the team members described team work they focused on closeness within the team and among different professions; so-called interprofessional team work. The team needed to find closeness in their way of handling work tasks and to create easy ways of communicating and finding weekly or daily contact among members. At first they worked a lot to facilitate cooperation and to ensure close communication on a daily basis. They also worked to find ways of giving faster decisions, from those who govern within the municipal organization to the older adults with less time in between. It is easy to get in contact with all the different professions, frequent meetings and as good as daily contact makes it easy to work and it results in us making quick decisions in favor of the older adults. Closeness to the whole team, the same base from the university course, forms of meetings, everyone in the team is engaged and has a high working moral. I have my time to reflect over myself and my way of working together with colleagues both within the same profession and together with the whole team.
Same direction and overarching goal
According to the staff, team work was understood as working in the same direction towards similar overarching goals, although this was not always easily achieved. The members in the team also referred to having experienced caring staff working in opposite directions. Working in the same direction, supporting each other’s decisions and judgments can be hard if some of the other team members do not have the same ambitions and perspective on care and rehabilitation. However, the staff described it as being a relief to work together with rehabilitation-oriented colleagues who had chosen this project, since they were driven by similar ambitions and had a similar view of caring. The whole staff now work towards the same goals. Everybody supports each other, towards the same goals and in turn is supported by the mangers of the team.
Learning from interprofessional dialogue
Interdisciplinary teamwork helped the staff to develop and reflect on the values and foundations for practice. According to the staff descriptions, ongoing discussions on rehabilitation activities and intentions were repeatedly debated in plenary, which gave the team members more reflected knowledge. I reflect on a daily basis together with the team which makes the reflections deeper and maybe I question myself more. When you have team of co-workers of different professions you examine your own work more critically which I think is very good. This is how I develop to be better at my job  .
.
Time for growth
According to the interprofessional team, the older adult’s development and progress were supported by reliable relationships and trust, and creating harmony instead of contributing to stress and time pressure.
Creating harmony
Finding ways of making the older adult experience a sense of calmness, a feeling of not being abandoned and being left alone was another important aspect brought up by the team members in their descriptions. The importance of being able to create a more relaxed situation, including having the time to get to know each other and be safe and cared for by the team was underlined as an important part of the reablement work. Taking part in the reablement process together created a harmonious approach to rehabilitation and the staff also found it easier to monitor progress and provide positive feedback when time was not limited. I think they experience that there is more calmness and harmony, no stress for them. The older adult can be calm, we are in this together.
Building the older adult’s self-confidence
The staff also described how the older adult’s self-confidence was developed through reablement, because the person was able to manage daily activities on their own. This growing confidence in managing life as before made most of the older adults keep on practicing skills even if the team was absent and this created a positive chain reaction which led to more positive results. The older adult develops self-confidence and has the [courage] to trust themselves in managing [difficult] moments of everyday life. We are there to support until they feel they manage by themselves. I have the possibility to bring in aspects of mental health which also might strengthen their trust in themselves.
Discussion and comprehensive understanding
The present study is based on narratives written by the members of an interprofessional team working with short-term goal-directed reablement with older adults. According to these staff, the basic foundations of the team’s reablement work are: creating reliable relationships, finding ways to empower older adult’s participation, giving enough time for growth, and developing a team with a negotiated approach in the work situation. The interprofessional team further underlined that basic elements of person-centeredness included respect for the person’s values and rights to self-determination in deciding on goals and staying in control over the reablement process. Offering reliable relationships supporting confidence and trust where there is time for the older adult’s growth of self-esteem and self-efficacy in regaining autonomy was important. The concept ‘being in a relationship’ as part of patient-centeredness can be compared with the present study where the staff in the interprofessional team put forward the staff as offering reliable relationships. Exploring the person’s own values and desires is described as a starting position of person-centered care 7 and another central concept is ‘being with oneself’, which show a similar understanding of how staff can contribute to patients’ empowerment. The present study illuminates how the older adult’s engagement influences the reablement process from two different angles. The first angle concerns when the person becomes empowered through gaining control of own goals of reablement. The other angle relates to the development of trust and confidence gained through the relationships with staff and their capacity to deliver supportive homecare promoting reablement.
The members of the interprofessional team in the present study describe trusting their own competencies and working methods and believe that through their way of working they manage to make major contributions to older adults’ reablement processes. Previous research has shown that staff confidence in working methods is a factor that contributes to job satisfaction and is likely to affect the care of the patients. 18 The staff in the present study believed in working within a negotiating team that facilitated finding mutual goals and directions that improved both work quality and older adults’ multi-dimensional health. The staff in the present study also underlined how their interprofessional teamwork included being able to offer help to others and being able to receive help from other professions as has previously been described, 9 but they also recognized the contribution concerning a broader development of reflected knowledge that the team delivered. The interprofessional team members in the present study described the importance of learning from interprofessional dialogue in a two-way communication where no hierarchy ruled the outcome of discussions or decisions made. Negotiating and communicating within the team was described as contributing to a culture commitment that overcame personal or uni-professional differentiated attitudes. 13 The team in the present study also argued that teamwork gave them confidence both in their general knowledge of homecare but also as a specific confidence of one’s profession. According to Norman and Peck, 27 four key components are needed to succeed with cooperation in interprofessional teams in community care: faith in systems within which they work; rejection of uni-professional cultures; strong shared philosophy; and trust in managerial solutions to problems. When comparing our team’s descriptions they seem to have created a working culture with a shared theoretical framework, rehabilitative approach and trust in managerial solutions of problems through communication and negotiation of professionals’ values. However, the staff did not reflect on trust related to their organization, and we as researchers did not ask about this. A possible interpretation is that the staff in the present study have faith in the organization, since they volunteered to take part in this two-year project to develop and test a new method in elderly care.
Time also held a high level of importance in working with short-term goal-directed reablement of older adults as experienced by an interprofessional team. Time for the older adult to grow was discussed, which is comparable with Trojan and Yonge’s 22 descriptions that spending more time became more effective as the older adults experienced that their needs were cared for and that seemed to create a sense of confidence in care. Earlier research often brings up leadership as having an important role in structures for the staff to be able to act in an evidence-based way. 8 Surprisingly little was mentioned about leadership’s role in work with short-term goal-directed reablement. This could be understood as a result of the non-hierarchical team spirit the team had already developed in the introduction phase of the intervention.
Methodological issues
A strength of the study including the team composition is that the participants were predominantly enrolled nurses. This might have empowered this profession, given they experienced more equal colleague relationships within the team, and strengthened the team spirit (e.g. work satisfaction and trust in ability to mediate reablement). However, it might be that even with this composition in the team, occupational therapists or physiotherapists might have more influence in reablement work, since they are the professions which usually are responsible for the rehabilitation strategies. In addition, this team was built up from an idea that even if rehabilitation is explicitly the responsibility of the aforementioned professionals, enrolled nurses are the ones who meet older adults the most in municipal homecare and, as a result, who have the greatest opportunity to make change.
It may seem strange that everyone in the team answered positively to being asked to participate in this study, but the fact is that members of this team have voluntarily applied to work within a development project linked to research from the beginning. These research participants were also particularly interested in developing their work, which is likely to have affected the results in a positive way. In addition, the short-term goal-directed reablement was a voluntary intervention for the older adults to participate in. Anyone could easily choose traditional homecare if they wanted to. Therefore the older adults joining the intervention were very engaged in their reablement, which perhaps not would be the case if short-term goal-directed reablement became a more common approach. Thus the team work with a motivated group of older adults, and that might have influenced their positive views of how the reablement intervention turned out.
Moreover, the staff were asked to contribute with written narratives by the research group that also had been involved in educating them at the university in preparing them for the new method. The email correspondence did not allow the narratives to be anonymous since they attached their narratives to an email to one of the researchers. However, we found it important to label the narratives as soon as we received them and not connect them to a specific person in the team. It might perhaps be interesting to see whether the different professions included in the team experienced participation differently, but we chose not to perform any analysis of differences as we were, according to Ricoeur, 23 searching for the common meanings of the phenomenon. In further research it could also be interesting to see whether such positive results would result from an in-depth interview study with the interprofessional team where some members have been replaced by new colleagues.
Conclusions and relevance to clinical practice
The findings highlight the process of short-term goal-directed reablement that can be understood as being strengthened by a collaborative approach and the efforts of different professions. Having an increased amount of time over a shorter period created, according to the team, harmonic confidence between the older adult and staff. Goal-directed reablement has the potential to build the older adult’s self-esteem and empowerment and thereby independency if listening to the person’s wishes, and giving the older adult control over goals and activities in the reablement process. An implication to praxis is that short-term goal-directed reablement has the potential to be experienced with a sense of calmness, a feeling of not being abandoned and therefore not claiming more homecare hours. These results can function as a way of widening understanding, and form the basis for decisions regarding planning for reablement processes that enable interprofessional teams to plan for home-based rehabilitation of older people as well as to widen the picture of how nurses’ confidence in their profession within this collaborative approach could be strengthened.
Footnotes
Acknowledgements
The authors would like to thank the older persons who participated in the study and the professional reablement team who made this study possible. We also want to thank Simon Dyar for professional revision of the English language.
Author contributions
Study design: L-KG, E-MA, MLE, VS, GÖ. Data collection: L-KG. Data analysis: L-KG, GÖ. Manuscript preparation: L-KG, E-MA, MLE, VS, GÖ.
Funding
The foundation of the Swedish social contract of Mälardalen MKHV provided financial support.
Declaration of conflicting interests
The authors declare that there is no conflict of interest