
Abstract
The adolescent population is facing mental-health challenges such as depression and anxiety. The aim of this study was to describe and investigate the mental health of adolescents, their relation to their parents, who they contact for help and their healthcare service use. A further objective was to describe and investigate family functioning in parents. A cross-sectional design was employed using register data from a survey of adolescents (n = 46,961), and surveys were conducted of two groups of parents – one group of parents with children with attention deficit hyperactivity disorder (n = 264) and one group of parents with school children (n = 157). Descriptive and comparative statistics were used. Of the adolescents, 5.65% were quite distressed. This group of adolescents would be less likely to seek help from friends and parents than the other adolescents. They were also more likely to use all types of healthcare services, and parents reported that they avoided discussing fears and concerns. School nurses are low-threshold professionals who can contribute in early support and interventions, providing service to all school pupils with an open-door policy. The use of family conversations focusing on strengths and resources may help the families to talk about difficult matters and highlight the resources in the family.
Background
The period of adolescence is considered as a difficult stage in the transition process to adulthood and is characterized by significant change mentally and physically. In addition, individual, social and contextual transitions also occur.1,2 Mental-health problems among adolescents have increased worldwide. 3 In Norway approximately 10–20% of the adolescent population experience mental distress, meaning having symptoms such as depression, anxiety and fatigue. 4 About half of these have more serious symptoms that generate a psychiatric diagnosis or behaviour disorders. 5 One of these disorders is attention deficit hyperactivity disorder (ADHD), with a prevalence of approximately 3–4% in school-age children in Norway 6 and 5% worldwide. 7 The Youth Studies in Norway show that the prevalence of self-reported mental distress had increased since 2010 to about 20% in the child and adolescent population. 8 Studies describe girls as more vulnerable to stress, having lower self-esteem, a higher state of depression and greater anxiety than boys.9–11 Early adolescent depression was found to persist into early adulthood and had negative consequences for health and associated health costs and resulted in increased work impairment. 12 Strategies such as prevention, health promotion and early identification may lead to better health outcomes later in life. 5 The 2017 World Health Day focused on depression with the campaign ‘Depression: let's talk’. 3
Adolescents describe the importance of having a good friend and having parents to talk to and feel secure with. 2 This highlights the parental role and family functioning. Family functioning is important in managing everyday life, and can be described as a dimension that influences the family in relation to problem solving, communication, roles, behavioural control as well as affective responsiveness and involvement. 13 Family functioning in families with children with ADHD has been described as weaker than in families of secondary school children. 14 Furthermore, perceived social support from the network and from the community health services influences family functioning positively in families with a child with ADHD. 15
Adolescents' use of healthcare services and whom they turn to for help if they have a problem or are not feeling well are little described. Discussing personal matters with their GP was reported as difficult for adolescents, and the adolescents with greatest need reported poorer experience of care. 16 Frequent primary healthcare use by girls has been associated with psychosocial difficulties. 17 The primary healthcare system in Norway for adolescents consists of school nurses and GPs – services all municipalities are required to have by law. 18 Some municipalities also offer psychological help, while others have to refer to the specialist health service. School nurses in Norway are authorized nurses with a one-year postgraduate education in public health nursing. 19 The school nurse is a low-threshold service providing advice to all school pupils from the age of six to 19 years old, with an open-door policy, located at the school where pupils can receive early healthcare at the lowest possible level. 19 The new national professional guidelines for the school health service in Norway 20 set out school nurses' responsibility for early recognition and referral of adolescents with mental-health problems.
The adolescent population facing mental-health challenges such as depression and anxiety has increased in recent years. Since the healthcare services are partly responsible for the health of adolescents, it is important to study adolescents' use of these services. Previous studies have stated that important factors of quality of life for adolescents are having a good friend and parents to turn to if they have problems or are not feeling well, and a family that functions well. With this in mind, it would be of interest to investigate if there are differences between the parents of adolescents with mental distress such as ADHD and other parents with regard to family functioning.
The aim of the study was therefore to describe and investigate the mental health of a population of adolescents, their relation to their parents, who they contact for help and their healthcare service use. Furthermore, the aim was to describe and investigate family functioning in two groups of parents.
Methods
Design and sample
The study had a cross-sectional design with use of register data from a survey of adolescents and surveys of two groups of parents.
The sample consisted of a total number of 46,961 adolescents, boys and girls, aged from 13 to 19 years old, from 97 municipalities across Norway. They responded to ‘Ungdata’, an annual survey of young people in lower and upper secondary schools. ‘Ungdata’ is an important and comprehensive source of information about adolescents’ health and wellbeing in Norway. (For more information on Ungdata, see ungdata.no.) The present study included data from the 2014 survey with an overall participation rate of 80%.
Two groups of parents were included. The first group consisted of 264 (out of 548 randomly sampled) parents of children with ADHD across Norway (Group A), giving a response rate of 48.2% (mothers 82.2% and fathers 17.8%). The second group included 157 (out of 584 randomly sampled) parents of children in three secondary schools in three municipalities (Group B), with a response rate of 26.9% (mothers 67.5% and fathers 32.5%).
Data collection
The participating adolescents filled in an online questionnaire anonymously during school hours.
The parents in Group A, who were members of the ADHD Association, received a questionnaire with an information letter by postal mail. An employee at the association had the coding key for the randomized sample and two reminders were sent. The parents in Group B were sent an information letter and the questionnaire by postal mail. The researcher (ØLM) contacted secondary school headteachers, and received lists of parents from which a sample was drawn.
Questionnaires
The adolescents
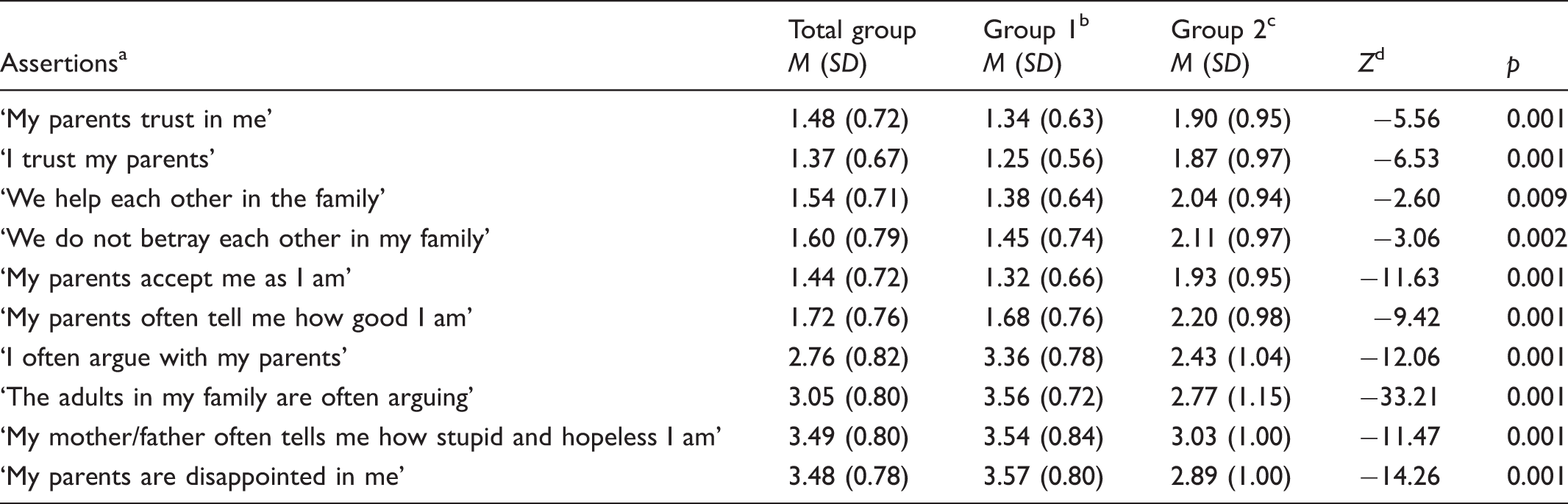
Background questions – with regard to gender and school level. Relationships with their parents – ten items (see Table 1). The items are answered on a four-point scale from 1 = suits very well, 2 = suits fairly well, 3 = suits fairly badly, 4 = suits not at all. A total mean score was calculated by adding item scores and dividing the sum of the number of items. Advice and help when they experience a personal problem or feel unhappy and sad – the question, ‘Imagine you have a personal problem. You feel unhappy and sad and need someone to talk to. Who would you talk to or turn to for help?’ offered five alternative responses: parents, other family members, friends, other adults and nobody. The response options were 1 = certainly, 2 = maybe, 3 = no. Use of the healthcare services during the previous 12 months – the question ‘How many times have you used the following healthcare services during the last 12 months?’ had five alternatives: school nurse or school doctor, health centre for youth, general practitioner (GP), psychologist or psychiatrist, and acute and emergency unit (A&E). The response options were 1 = never, 2 = one to two times, 3 = three to five times and 4 = six times or more. The adolescent−parent relationship. Assertions answered on a four-point scale with the smaller mean the better, except for the negative assertions. Group 1: not distressed. Group 2: fairly distressed. Mann–Whitney U test.
The parents
Background questions – included the parents' age and gender and the age of their child. The Family Assessment Device (FAD) was developed by Epstein, Baldwin and Bishop.
24
In this study, the subscale ‘General Functioning’ with 12 items measuring family climate and functioning was used. The items were answered on a four-point scale from 1 = totally agree to 4 = do not agree at all. A total FAD mean score was calculated by adding item scores and dividing the sum of the number of items. The lower mean score, the better family functioning.
Ethical considerations
The study was approved by the Regional Ethical Committee for Medical and Health Research in Norway in respect of the parents of children with ADHD, and approved by the Norwegian Social Science Data Services (NSD) for the other group of parents. The ‘Ungdata’ survey contained only anonymous data and no approval was therefore needed. The entire research process was guided by ethical research principles on confidentiality, non-maleficence and justice. 25
Statistics
Statistical analysis was performed using IBM statistics version 22. Descriptive and comparative analyses were used. An independent-sample t-test compared for differences between boys and girls in terms of measures of depression and anxiety, and the total mean score measured the relationship with parents. An independent-sample t-test analysed the two groups of adolescents (one group of adolescents who were not distressed − Group 1 – and one group who were quite distressed − Group 2) with regard to the items measuring the relationship with their parents. The two groups of parents were compared for differences with regard to the total FAD mean score. The Mann–Whitney U test was run in order to compare the two groups of adolescents in terms of the items concerning their relationship with their parents, and the items measuring advice and help when experiencing a personal problem or feeling unhappy and sad. Furthermore, the Mann–Whitney U test was used to compare the two groups of parents on the FAD items. 26 All tests were two-tailed with a p-value of <0.05.
Results
Adolescents
The adolescents' measurements for symptoms of depression and anxiety gave a mean score of 1.82 (SD = 0.70), a mean score of 1.89 (SD = 0.73) for depression and a mean score of 1.52 (SD = 0.65) for anxiety. Girls reported significantly more depression (M = 2.10, SD = 0.74) than boys (M = 1.68, SD = 0.63) (t = 116.425, p = 0.001). They also reported significantly higher anxiety (M = 1.77, SD = 0.72) than boys (M = 1.28, SD = 0.47) (t = 103.33, p = 0.001).
The adolescents' responses to the items relating to their relationship with their parents are reported in Table 1. Overall, the total mean score (M = 2.43, SD = 0.38) revealed that most of the adolescents, 82.5%, were pleased or very pleased with their parents. No significant differences between boys and girls were found.
The adolescents were divided into two groups – one of adolescents who were not distressed (Group 1) and one of those who were quite distressed (Group 2). The group of quite distressed adolescents represented 5.65% of the adolescents. Comparisons between the two groups in relation to their responses to the items regarding their relationship with their parents are shown in Table 1. There were significant differences between the two groups in all the ten items. The group of quite distressed adolescents (Group 2) argued more with their parents, than the group who were not distressed (Group 1). The parents of the distressed adolescents (Group 2) also argued more with each other compared with the adolescents who were not distressed (Group 1).
Comparing groups of youths with psychological distress and less psychological distress: Who would you turn to and seek help from when you have a personal problem or are feeling sad and need someone to speak to?
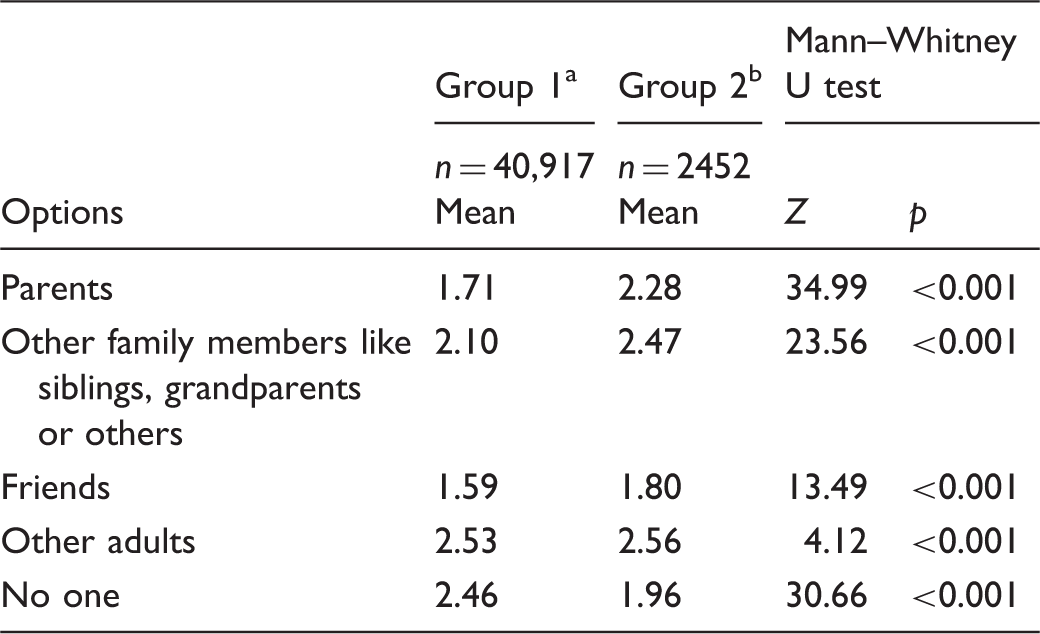
Options were responded to on a three-point scale 1 = certainly, 2 = maybe, 3 = no.
Group 1: not distressed.
Group 2: fairly distressed.
The quite distressed adolescents (Group 2) would be more likely to use all types of health services (Figure 1). In general, most of the adolescents did not use the health centre for youths, 64.1% did not see the school nurse or school doctor, and 37.5% did not see a GP. However, 24% had seen the school nurse or school doctor one to two times over the previous 12 months and 37.3% had seen a GP one to two times. Some 14.3% saw a GP three to five times and 6% saw a GP more than six times. Altogether 92.7% of the adolescents who were not distressed (Group 1) had not used the services of a psychologist or psychiatrist, while 2.3% of this group had used this service six times or more during the previous 12 months. The quite distressed group (Group 2) 58.9% did not use this service at all, but 23.4% had seen a psychologist or psychiatrist more than six times in the last year. Furthermore, the girls used all health services significantly more often than the boys (p > 0.001).
Adolescents' healthcare use divided in two groups: quite distressed and not distressed.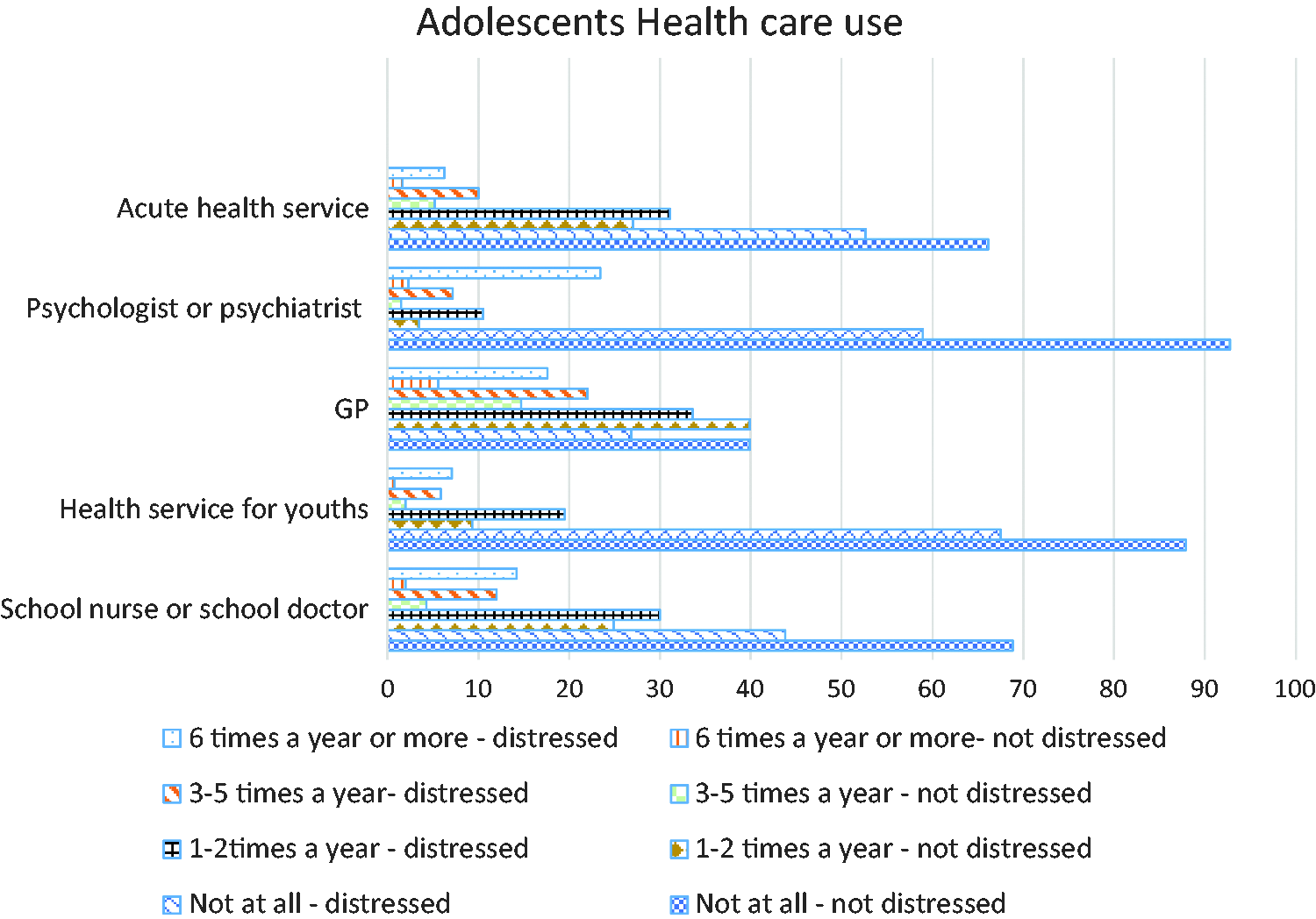
Parents
Comparing the groups of parents in questions on family functioning.
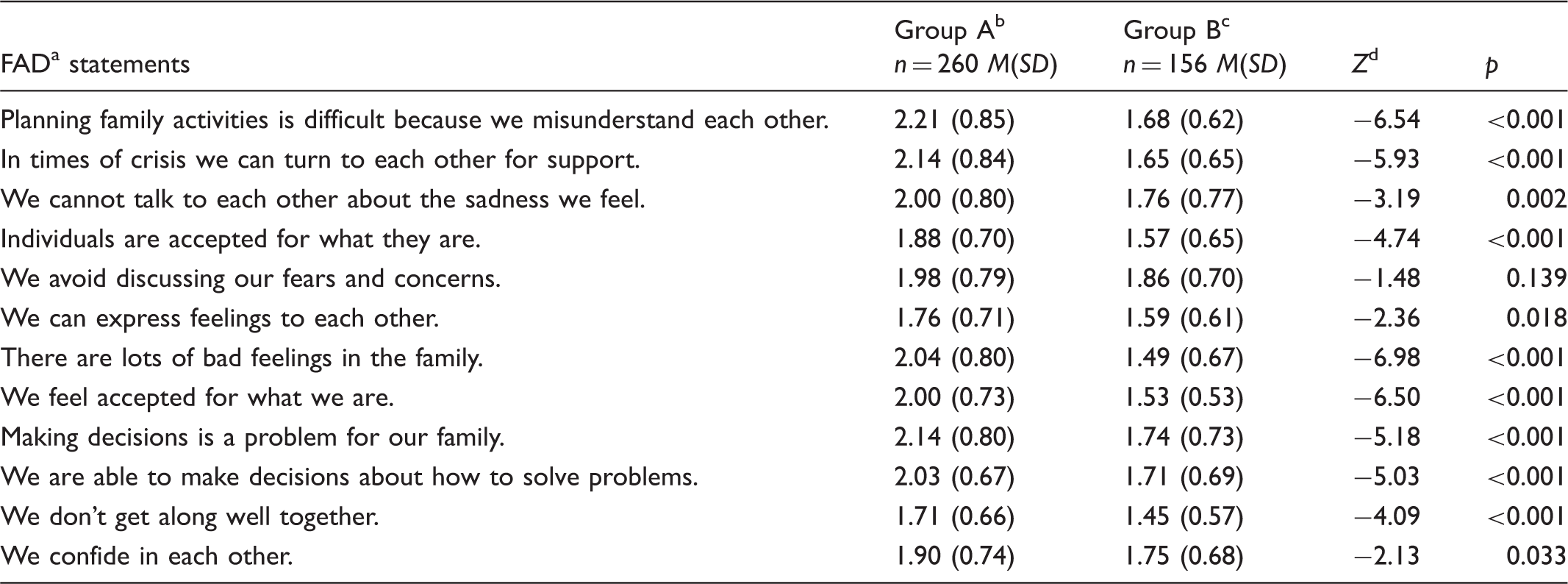
Family Assessment Device, scores could range from 1 (most favourable) to 4 (least
favourable).
Group A parents with a child with ADHD.
Group B parents of children in secondary school.
Mann–Whitney U test.
Discussion
The main findings in this study's reveal that girls reported more anxiety and depression than boys, as is also reported in other studies.10,11 The group of adolescents who feel quite distressed also quarrel more with their parents, and they are less likely seek help from their parents, friends or other adults than the other group of adolescents who were not distressed (Group 1). Furthermore, Group 2 had used more of all types of healthcare services during the previous 12 months than Group 1. The parents of children with ADHD reported weaker family functioning than the other parents.
Adolescents in general use healthcare services to a lesser extent than adults. 27 The adolescents in this study also used healthcare services to a small extent. Hence, the adolescents who felt quite distressed (Group 2) used all kinds of health services more than the other adolescents did, and they turned to their parents and friends for help to a lesser extent than the other group of adolescents (Group 1). This survey focused on all parts of the health service. This reflects the school nurse's legal responsibility to have routines for cooperation with GPs, other personnel in schools, pedagogic psychological services (PPS) and the psychiatric specialist health services. 19 The school nurse is a low-threshold service and may be the first professional adolescents turn to. However, school nurses have described uncertainty as to who their collaborating partners are, who they can turn to for collaboration on mental-health matters in the case of adolescents, and difficulties in collaborating with GPs. 28 The collaboration with the psychiatric specialist service has been described as varying in quality and as being person-dependent. 29 Therefore, school nurses often have to depend on their own clinical judgement as to whether they can handle such problems themselves before consulting with and referring to a mental-health specialist. 30 The school nurses' confidence when addressing adolescents' mental-health issues is highlighted in another study 31 in which school nurses asked for more supervision and decision-making tools with regard to mental-health issues.
Adolescents describe their relationship with peers and having a good friend as vital to their quality of life as well as having parents they can talk to. 2 The relationship with parents has proved to be a determinant of adolescents’ psychosomatic problems. 32 Parents can create an essentially secure base in life, as a ‘life coach’, and the family is essential if it functions well.33,34 Parents may also play a role in in assessing treatment and support for their adolescent child. 33
Parents of children with ADHD reported significantly lower family functioning than the other parents in this study. Family functioning was shown to be influenced by the child's behaviour, social support, sense of coherence and support from the community health service in a study of parents with children with ADHD. 15 It is questionable whether the parents of children with ADHD perceive family functioning differently from parents of adolescents with mental distress. However, other studies report weaker family functioning in families with adolescents having a psychiatric diagnosis.35,36 Hence, in this study, there was no significant difference between the groups of parents regarding the item ‘We avoid discussing fears or concerns’. The quite distressed adolescents reported that they were less likely to seek help when having a personal problem. If the parents do not discuss fears and concerns the problems they see in their adolescent may not be raised as a focus. Parents may try to reduce conflicts and thereby avoid talking about their concerns. 37
Having an adolescent with mental distress may be difficult for the parents to handle, and support from the network and community health service may strengthen them. The school nurses must be available for the adolescents, and sometimes they might be the first person the adolescents have dared to speak to about difficult topics in life. 38 School pupils may have depressive thoughts related to the experience of being an ordinary young person who is not unhealthy, but who nevertheless needs to speak to a professional. 38 Not all mental-health interventions are complex and only able to be delivered by specialized personnel. 39 The school nurse can be a supportive adult with a professional relationship to adolescents with depression or other mental distress. On the other hand, adolescents suffering from mental distress stated that they did not necessarily find the school health services easily accessible. The school nurse's office was often hidden in a back entrance and walking through the corridors made pupils feel that they were being observed by others. 40 A study in Norway revealed that the school nurse was present at the school two days a week. 41 The adolescents live in the present and may not be able to wait several days before seeing the school nurse. The recommendation for improvement is to expand the service so that the national intentions of early intervention, including prevention and promotion, can be met. It is also important to have clear guidelines for cooperation with other professions when there is a need.
School nurses use different approaches. Clausson and Berg 42 used ‘family support conversation intervention sessions’ to improve schoolchildren's mental health, in order to strengthen the parents in their role and reveal the family's resources. This may lead to stronger family functioning, promoting a family climate with internal support, expressed emotions, acceptance, decision-making and the courage to talk about fears and concerns. 13 The school nurse supported the families and encouraged them to talk about difficult matters using ‘family support conversation intervention sessions’. 43 The conversations focused on both the adolescents’ and the parents’ view of the situation and how the family can support the adolescent.
Other interventions focus on strengthening adolescents as a group. Garmy et al. 44 evaluated a universal school-based programme employing cognitive-behavioural strategies. This intervention was used for strengthening adolescents on a group level. This might then inspire the adolescents to be supportive friends.
The present study had strengths as well as limitations. The strengths of the study were the use of nationwide recruitment, both in the adolescent group and in one of the groups of parents (Group A). This study contributes knowledge from a national survey and generates knowledge from this population. The cross-sectional design limits the causality of the study results. The response rates from parents were low especially from fathers. How to get fathers to respond is a question raised by other researchers. 45
Conclusions and further research
This study highlights the quite distressed group of adolescents’ avoidance of seeking help from friends, parents and other adults and their healthcare service use in Norway. It may, however, have transferability to other parts of the world where school nurses provide health services for adolescents. Mental distress in adolescents is a high priority topic in the rest of the world, and the World Health Organization has put depression on the agenda. The use of family intervention sessions with family strength and resource conversations may help families to talk about difficult matters, to reveal a common understanding of the problems and highlight the resources in the family. Further research with the use of ‘family support conversation intervention sessions’ in families with adolescents and young adults with mental distress is needed.
Footnotes
Author contributions
Study design: ØLM and MLH-L; data collection; ØLM; data analysis: ØLM and MLH-L, manuscript preparation: ØLM and MLH-L. All the authors have seen this last version and agreed upon it.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.