
Abstract
Objective
Online parenting interventions for enhancing child development, specifically mental health is relatively new in Malaysia. This pilot study tests the feasibility, acceptability, and initial effects of a universal digital-assisted parenting intervention (DaPI) in promoting mental health in adolescents by improving parental behaviors and self-efficacy.
Methods
A two-arm pilot randomized controlled trial was conducted. Twenty-four mothers of adolescent aged 10 to 14 years from a non-clinical sample were recruited online and randomly allocated into two groups (intervention [DaPI] and waitlist-control [WLC]). Eight weekly sessions were delivered online via technological devices. Feasibility outcomes were based on the participants’ engagement in DaPI and study retention. Primary (parental behaviors and self-efficacy) and secondary (adolescent mental health) outcomes were assessed using an online survey at baseline (T0), post-intervention (T1), and 1-month follow-up (T2). Data were analyzed using descriptive and inferential statistics and an intention-to-treat approach.
Results
The DaPI was well received by the mothers. Retention was high (81.8%) in both groups and intervention adherence was excellent (91.6%). Within-group analyses showed a significant decrease in physical control at T2 and an increase in parental self-efficacy at T1 and T2 among the DaPI mothers. No significant differences were observed in adolescents’ mental health at any time point. As for the WLC group, there were no significant differences in all the outcome variables across the three assessment moments. Between groups analyses revealed DaPI mothers had significant differences in proactive parenting at T1, and in positive reinforcement and lax control at T2. There were no significant differences in adolescents’ mental health between the groups at any time point.
Discussion
The DaPI is feasible and acceptable in the Malaysian context. Findings show promise regarding the initial effects of the DaPI. However, a larger RCT is needed to determine its effectiveness in promoting mental health of adolescents.
Trial registration
https://www.irct.ir/; identifier: IRCT20211129053207N1.
Introduction
In Malaysia, mental illness in adolescents has been increasing, particularly during the COVID-19 pandemic. Behavioral (antisocial and conduct problems) and emotional disorders (depression, anxiety, and stress) are common mental health problems in adolescence. 1 The onset of mental illness can occur during the early stages 2 of adolescence, that is, between the ages of 10 and 14. 3 In 2019, the population of adolescents in Malaysia was 4,797,200, of which nearly 53% were categorized as early adolescents. 3 Before the pandemic, 424,000 (4.5%) Malaysian children were reported to have mental health problems. 4 Of these, 9.5% were aged between 10 and 15 years, 8.4% were girls, and 8.8% lived in rural areas. 4 In 2017, a survey 5 showed that anxiety (39.7%) had the highest prevalence compared to depression (18.3%) and stress (9.6%) in adolescent aged between 13 and 17 years. These numbers are expected to increase due to continuous stressors resulting from the COVID-19 pandemic. Unfortunately, published data on Malaysian adolescent's mental health during the pandemic stages are still lacking, as most studies have focused on groups such as older adults, university students, and healthcare workers. 6 A study involving 348 children and adolescents aged between 8 and 17 years reported experiencing clinical trauma resulting from the COVID-19 pandemic. Furthermore, some of them experienced anxiety (28.5%), depression (31.4%), and stress (13.3%) due to family hardship, social isolation, stressors from online learning, and loss of a family member during the pandemic. 6
Numerous public health efforts have been made to tackle the rise of mental health problems in adolescents. One of the most common approaches is conducting universal parenting programs at the community level. A universal parenting program aids parents seeking support or extra parenting advice 7 for reducing the risk of mental health issues in adolescents. Prior research indicates that improving key parenting factors such as parenting behavior, self-efficacy, and mental health can mitigate childhood adversity and improve overall adolescent outcomes.8–10 A universal parenting program that targets to improve these parenting factors would then help in building a secure parent–child relationship thus becoming protective factors for adolescent's mental health problems and externalizing behaviors. 11 The effects of a universal parenting program have been well documented across the globe (i.e. UK, 7 Thailand, 12 Spain, 13 Great Beirut, 14 Brazil 15 ) as robust and often long-lasting across various developmental outcomes in children and adolescents.8,16 For example, the CANparent Trial 7 was effective in improving parents’ sense of parenting efficacy and mental health which subsequently improved parents’ relationship with their child. Similarly, The Positive Parent Program 13 was found to increase parenting competencies that in turn promotes positive parenting among medium-high educated parents. Meanwhile, the ACT Raising Safe Kids Parenting Program 15 found that by improving parenting practices, child behavior problems were reduced. Even though well established, studies on universal parenting programs are still lacking, 17 especially in Malaysia.
As Malaysia progresses toward becoming a developed country, one aspect of its development can be seen in the crucial role played by digital technology in increasing the productivity, innovation, and livelihood of Malaysians. The Malaysian Communication and Multimedia Commission have conducted an Internet User Survey (IUS) since 2012 to monitor the digitalization trend in Malaysia. A recent IUS indicated increasing Internet usage among Malaysians over the past decade. 18 In 2012, 64.1% of Malaysians were Internet users. In 2020, the percentage of Internet users increased significantly to nearly 89%. Of them, 21% were considered heavy users as they spent more than 12 hours daily on the Internet, and 50% were regular users as they spent 5 to 12 hours daily. The increase in Internet use mostly resulted from the COVID-19 lockdowns, as Malaysians relied on the Internet to work from home; attend online classes; and access information, communication, and entertainment. 18 Therefore, unsurprisingly, the percentage of Malaysian Internet users increased to 95.5% by 2021. 19 Malaysians were found to favor mobile phones (99.6%) and computers (88.3%) for accessing the Internet for social networking (99%); downloading pictures, videos, and music; playing games (91.8%); and finding information about goods and services (89.4%). This increase in Internet usage indicates that Malaysians have now embraced digitalization and may be willing to utilize health apps to better manage their health. 20 A recent study within Selangor, the most developed and populous state in Malaysia, 21 reported that 33.5% Malaysians utilized mobile health apps daily, while 36.7% of them reported using their mobile health apps at least once weekly and 25.2% monthly. 22 It was further reported that the most utilized mobile health apps were multi-purpose health apps (53.6%) and fitness apps (38.1%). The main benefits of mobile health apps were reported to be tracking of health status (47%), motivation (41%), and gaining knowledge about health and fitness (9%). In view of the increasing mobile health apps pattern of usage, utilizing digital technology for therapy is the way forward for mental health practices.
Digital-assisted interventions are relatively new in Malaysia. The few studies available noted several challenges particularly in relations to the utilization of various platforms such as video conferencing, apps or social media. Intervention using video conferencing, especially those targeting behaviors takes time to get used to despite online assistance from therapist. 23 Apps downloadable on smartphones were convenient and effective yet was found to lack interactive features. 24 Interventions using a mix of traditional face-to-face and social media were well received by parents 25 and adoelscents. 26 Engagement, however, was noted to be higher using social media due to its convenience 25 affordability and privacy. 26 Despite the challenges, these studies have generally indicated positive outcomes from their interventions. Therefore, suggesting that digital-assisted interventions are feasible and acceptable in the Malaysian context. To date, to the best of our knowledge, no technology-assisted parenting intervention has been conducted to promote the mental health of Malaysian adolescents.
The primary aim of this pilot randomized control trial was to test the feasibility and acceptability of a universal digital-assisted parenting intervention (DaPI). Second, the study examined preliminary data on the efficacy of the DaPI in promoting mental health of adolescents by improving parenting behaviors and parental self-efficacy.
Materials and methods
Design
An 8-week two-arm pilot RCT was conducted in February 2022, consisting of pre- (baseline) and post-intervention (April 2022) and 1-month follow-up (May 2022) periods. The trial was registered at the Iranian Registry of Clinical Trials (registration number: IRCT20211129053207N1).
Participants
Participants were parents of early adolescents aged between 10 and 14 years recruited from across Malaysia. This age group was chosen because early adolescence is among the most crucial yet frequently neglected stage of development. 27 Inclusion criteria were parents who have a child aged between 10 and 14, digitally literate, have access to the Internet, fluent in Malay, and willing to participate in weekly online sessions. Parents were excluded if they reported receiving professional help for their adolescent's mental health.
Procedure
Parents from the community were recruited through social media platforms, word of mouth, and the study website. Once parents were screened for the inclusion and exclusion criteria, they were given a consent form and information sheet regarding the study. Parents were made aware of the nature of the study and that they can withdraw from the study at any point of time. Thereafter, eligible parents who consented to participate in the study completed the baseline (T0) assessment and were randomized into two groups based on a 1:1 ratio—DaPI and WLC groups. As contamination was deemed unlikely among the parents, individual randomization by a research coordinator was utilized because the intervention was delivered online through the study's website. Due to the nature of the pilot study, the participants and facilitator (a doctoral student with over 10 years of experience as a clinical psychologist) handling the DaPI could not be blinded to the condition. However, the coders and data analysts were blinded to the group allocation status.
A week prior to the program's commencement, parents in the DaPI group were given a personalized login ID and password to the intervention website. Those in the WLC group received their login details after completing the 1-month follow-up assessment.
Intervention
The DaPI is a universal parenting intervention program developed by a team of clinical psychologists, psychiatrist, and researchers specifically for Malaysian parents by referring to several successful evidence-based programs developed in the West, such as Parenting Wisely, 28 the Triple-P Positive Parenting Program, 29 and Incredible Years. 30 Dozens of RCTs have been conducted to determine the efficacy of these programs across continents. For example, the Parenting Wisely program has been conducted in the United States31,32 and Australia, 33 the Triple-P Positive Parenting Program has been conducted in Singapore, 34 Indonesia, 35 Turkey, 36 and Iran 37 ; and Incredible Years has been tested among families from the Netherlands,38,39 Ireland, 40 Turkey, 41 and Malaysia. 42
Despite the efficacy of Western parenting programs, adjustments are needed when adapting them to Asian cultures. 43 Moreover, parenting styles from Western cultures may not be appropriate for implementation in the Malaysian context as the parenting styles of Malaysian parents may be more localized and culturally specific. 44 Therefore, the DaPI program is unique as it includes culturally specific parenting beliefs and examples that represent the diverse ethnicities and religions of Malaysian parents. The DaPI program includes videos, infographics, comic strips, and interactive exercises, which were designed using day-to-day parent–child scenarios commonly found in the Malaysian context. The program's scenarios are also more inclusive of the religion and culture of Malaysia, which is characterized by filial piety. For example, the program emphasized the development of independence in adolescents within the framework of values such as respecting elders and accepting the responsibility of caring for them. Additionally, activities suggested in the program to promote family involvement and parent–child attachment included spending time together performing religious activities such as going to the mosque, praying, and reading the Holy Quran together.
The DaPI provides parents with training on effective parenting skills that promote the mental health of adolescents. Specifically, this program aims to increase parents’ positive parenting behaviors and self-efficacy across eight weekly sessions. Additionally, the program includes effective strategies for building secure parent–child attachment, handling parent–child conflict, and managing parents’ and adolescents’ mental health. As emphasized by past literature, effective parenting behaviors that strengthen the parent–child relationship promote positive adolescent outcomes such as reducing emotional problems (peer problems) and behavioral problems (conduct disorder).45–47 Furthermore, effective parenting behaviors enable parents to demonstrate to their adolescents how to communicate effectively, listen empathetically, regulate emotions, and resolve conflicts. Table 1 provides an overview of the DaPI program and its intended objectives.
Session content of the DaPI.

The DaPI could be accessed online from February to May 2022 at any time using computers, tablets, or smartphones, making it convenient for parents. It consists of various parent-training materials in written, visual, and audio formats along with interactive quizzes, case scenarios, and parent–child activities. The DaPI is fully conducted in Malay, the official language of Malaysia.
Parents in the DaPI group gained immediate access to the program upon receiving login details. New sessions were made available to the parents after the completion of the previous session. For example, a parent who completed Session 2 could advance to Session 3 in the third week of enrolment. Parents were encouraged to complete one session per week throughout the eight-week program. After the completion of a session, parents received a text message via WhatsApp to reinforce the parenting techniques and activities learned. Parents were also notified of the availability of a new session which prompts them to use the program.
As the DaPI is self-monitored, it allows parents to complete the sessions at their own pace. Each session takes approximately 30 minutes to complete. Parents can choose to save their progress and return to a particular session on a later date and time. Parents could monitor their progress and receive written feedback on their performance from the facilitator on the intervention website. For example, in case scenario activities, parents would describe the parenting techniques they plan to use in the scenario. The facilitator would then provide positive or constructive feedback based on the techniques described. If a parent becomes inactive for more than 3 weeks, a reminder via WhatsApp and email will be sent to encourage parents’ continuation with the program as well as check on any arising issues.
At the end of the pilot study, parents were asked to fill in a feedback form to help the researchers improve the DaPI program. Parents were requested to complete the program by May 29, 2022, to provide the researchers with sufficient time to analyze the feedback and make modifications to the program in preparation for the larger RCT.
Control
Parents randomized into the WLC group received no treatment during the 8-week program and continued their usual parenting practices. These parents were given access to the program 12 weeks after enrolment.
Measures
Data were collected at the following three time points: when parents enrolled in the program (T0), post-intervention (T1), and at 1-month follow-up (T2). In addition to reminders, parents received an e-voucher worth MYR10 at each time point as an incentive to complete the questionnaire.48,49 Parents provided information on their personal and adolescent characteristics, family social context, and parenting and adolescent mental health. All measures went through a forward-backward translation procedure from English to the Malay language by two bilingual translators. Content validity on all measures was carried out by six experts to review the content for consistency, clarity, difficulty, and suitability for inclusion. Face validity was then carried out on 10 randomly selected parents.
Feasibility
Feasibility was measured in terms of recruitment, retention, and completion of the intervention. Recruitment was determined based on the number of potential participants who showed interest in the study, fulfilled the inclusion criteria, and completed baseline assessment. An acceptable recruitment rate would be at least 80% of the target sample size. 8 Retention was based on the number of enrolled participants who completed all measures at three time point. Retention rate was considered acceptable if more than 50% of participants completed all measures at each time point, similar to past studies.50,51 Completion was based on the percentage of participants who participated in all the eight sessions of the DaPI program, which was considered acceptable if at least 75% of participants completed the program. 52
Acceptability
At post-intervention (T1), participants rated whether the intervention was deemed appropriate, acceptable, and effective in promoting mental health of early adolescents. Answers were on a 4-point Likert scale ranging from “Strongly disagree” (1) to “Strongly agree” (4). The program is considered acceptable if at least 75% of participants agreed or strongly agreed with the questions provided, aligning with acceptability rates in past studies.53,54 In addition, parents were invited to answer an open-ended question about their overall satisfaction with the program.
Primary outcomes: parenting measures
The Multidimensional Assessment of Parenting Scale (MAPS) 55 is a 34-item self-reporting measure comprising two broad domains—positive and negative parenting—covering seven narrowband domains of parenting behavior. The positive parenting domain includes four narrowband domains (proactive parenting, positive reinforcements, warmth, and supportiveness), while the negative parenting domain comprises three narrowband domains (hostility, physical control, and lax control). Furthermore, MAPS items are scored on a 5-point scale ranging from 1 = never to 5 = always. The total scores are obtained by summing all item scores in the respective domains. High scores in the positive parenting domain indicate greater levels of warmth, supportiveness, and positive control. High scores in the negative parenting domain indicate high levels of hostility and over- and under-controlled parenting behaviors. Both the broad (αPositive = .90 and αNegative = .90) and narrowband (ranging from .76 to .96) domains were reported to have good internal consistency and concurrent and convergent validity. 56
The Child Adjustment and Parent Efficacy Scale (CAPES) 57 is a 20-item measure of parental self-efficacy in managing adolescent's emotional and behavioral health. Scale items are rated on a 4-point scale (0 = Not true of my child at all to 3 = True of my child very much, or most of the time), through which parents indicate how true each statement is for them over the last four weeks. Total scores range from 0 to 60, with higher scores indicating greater self-efficacy in dealing with adolescent's emotions and behaviors. The CAPES self-efficacy scale was reported to have good construct and discriminant validity, 52 as well as good internal consistency (α = .97).
Secondary outcome: adolescent's mental health measure
The CAPES 57 was used to measure parents’ perceptions of their adolescent's mental health. This scale has 30 items under two subscales—behavioral and emotional maladjustment. Parents rated their adolescent's behavioral concerns, competencies, and emotional adjustment over the past four weeks on a scale ranging from 0 (not true for my child at all) to 3 (very true for my child or most of the time). Total scores ranged from 0 to 90, with higher scores indicating a greater intensity of problems. The internal consistency of the total scale (α = .94) and subscales (αBehavioral Problem = .93 and αEmotional maladjustment = .71) were reported to be good, as well as adequate convergent and discriminant validity. 57
Statistical methods and preliminary analyses
Descriptive analyses were conducted to examine baseline participant characteristics, attendance, acceptability, and intervention outcomes in the DaPI. In terms of feasibility, the proportion of participants who completed the online sessions was assessed. Chi-squared and t-tests analyses were conducted to examine between-group and within-group differences in the participants’ characteristics and intervention variables. Analyses were conducted using SPSS 25, and all outcome variables were tested for normality prior to the analyses. Paired sample t-tests were conducted on measures that followed a normal distribution, whereas Wilcoxon signed-rank tests were performed on measures that were not normally distributed.
Preliminary intervention effects were examined using intention-to-treat analysis. Missing data due to dropouts at post-intervention and follow-up were imputed using the last observation carried forward (LOCF) method. This method was chosen as it maximizes the number of observations by assigning a singly imputed score for each missing observation. 58 Furthermore, LOCF allows examination of trends over time, rather than focusing on the final value. 59 To enable a comparison of post-treatment effect sizes between the variables, all effect sizes of parametric and nonparametric tests were computed using Cohen's d via Psychometrica, a free online computing software. 60 Cohen's 61 suggestion on the magnitude of effect sizes was used to interpret the effect sizes. Values of less than 0 indicate an adverse effect, 0.0–0.1 indicate no effect, 0.2–0.4 indicate a small effect, 0.5–0.7 indicate a medium effect, and more than 0.8 indicate a large effect.
Results
Demographic data of participants
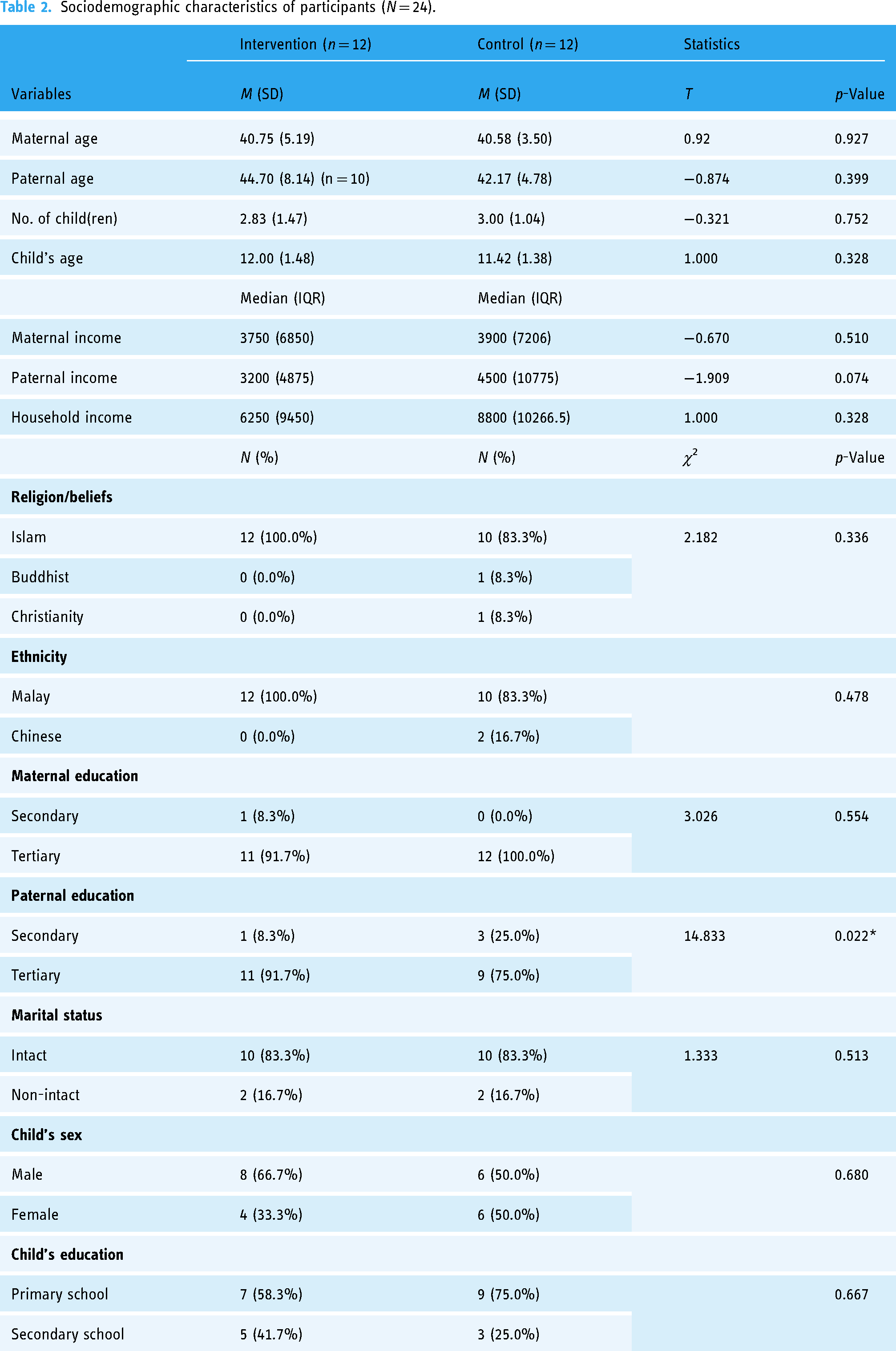
Although this pilot study invited eligible parents from across Malaysia to participate, only 30 mothers responded to the invitation. Of these, only 24 mothers were eligible based on the inclusion and exclusion criteria. The mothers were comparable across all demographic characteristics (Table 2). Most of the mothers were middle-aged (M = 41, SD = 5.19), Malay (91.7%), and Muslim (91.7%). Nearly all mothers reported being married (83.8%), completed tertiary education (95.8%), and had a median monthly family income of MYR7900 (IQR = 8500). Mothers in the DaPI group were found to significantly have partners with higher education level than the control group. Of the adolescents in this study, nearly 58.3% were boys, with an average age of 12 (SD = 1.4) years. Most of the adolescents were in primary school (66.7%), while a smaller portion was in secondary school (33.3%).
Sociodemographic characteristics of participants (N = 24).
Feasibility of study methodology
Recruitment, retention, and completion
The recruitment advertisement for the pilot study was run for a month in January 2022, within the time frame specified by the grant. As shown in Figure 1, parents who responded to advertisements on social media platforms were screened for eligibility. Out of the 30 parents who responded, only 24 fulfilled the pilot study criteria. In line with past studies62,63 this sample size (n = 24) was deemed acceptable for a two-arm pilot RCT based on the flat rule of thumb recommendation of Julious, 64 Kieser and Wassmer, 65 and Whitehead et al. 66 of having a minimum of 10 people per arm for a pilot trial. Participants in the pilot study were asked to complete the baseline assessment (T0; 100%). They were then randomly assigned to either the DaPI or the WLC group. In terms of study retention, 20 of the 24 participants (83.3%) completed the follow-up assessments; however, retention rates varied between the DaPI and WLC groups from baseline to other time points. For the intervention group, the retention rate was 83.8% at both T1 and T2. In contrast, the retention rate for the WLC group was 100% at post-intervention and 83.8% at 1-month follow-up. The reasons for dropout at T1 were hospital admission due to post-COVID-19 illness (n = 1) and losing contact (n = 1), while those for dropout at T2 were busy work schedules (n = 1) and losing contact (n = 1). Nevertheless, the retention rates were deemed acceptable for an online universal parenting intervention.50,51 Similar to past studies,45,46 intervention completion was excellent, with 11 out of 12 intervention participants (91.6%) completing all online sessions. Feedback from the facilitator suggested that all contents were covered, and personalized written feedback was provided for all session activities.

Flowchart of the participants.
Acceptability
Of the 11 parents in the DaPI group, 10 completed the satisfaction survey. As presented in Table 3, most participants reported being highly satisfied with the DaPI. Moreover, all parents considered the program beneficial and informative as well as interesting and practical. Additionally, parents indicated their satisfaction with the amount of help they received from the program and the facilitator: “The DaPI program is practical and gives significant impact in building a healthy relationship not only with my child, but with my partner and other family members. The content of the DaPI program is very well organized, easy to understand, and does not take a long time to complete. The videos included are interesting and informative. I strongly encourage other parents to participate in the DaPI program.” (Mrs. A)
Results of DaPI participant feedback questionnaire.

Further, parents reported that the DaPI helped with their adolescent's emotional maladjustment and behavioral problems. Parents rated that they felt satisfied with the skills taught on managing their adolescent's emotion and behavior. Overall, parents felt satisfied with their adolescent's changes in emotion and behavior by the end of the intervention: “Since I practiced the techniques taught in the DaPI program, I noticed that my child talks to me more. I feel so much closer to her now.” (Mrs. N)
Parents reported that in addition to improving their relationship with their focus child, the DaPI program also helped improve the relationship with other family members such as partners and other children. Only one parent was found to report that DaPI was not beneficial in improving her relationship with her partner. Upon further inspection, this parent was found to be divorced.
Serious adverse event and contamination
No serious adverse events were reported during the study, indicating that the program was safe. Participants adhered to the request to not share the DaPI learning materials and activities with their family and/or friends. No contamination issues were reported.
Descriptive on outcome measures
Within-group analyses
Table 4 presents the results of the within-group analyses at pre- and post-intervention and at 1-month follow-up for the DaPI and WLC groups. Only one of the measures of parenting behavior, physical control, was found to have a significant change at the 1-month follow-up in the DaPI group (Z = −1.98, p = 0.047, Cohen's d = 1.396). Cohen's d score suggested that the improvement in the DaPI group had a large effect size. In terms of parental self-efficacy, the DaPI group showed significant improvements at post-intervention (t = −2.83, p = 0.015, Cohen's d = 0.816) and 1-month follow-up (t = −2.20, p = 0.050, Cohen's d = 0.636). Cohen's d calculation indicated that these improvements had medium-to-large effect sizes. As to the WLC group, no significant differences were found in all primary and secondary outcomes across the three assessment points.
Within-group differences pre- and post-intervention and at 1-month follow-up for the DaPI and WLC groups.


Note:
Two-tailed accepted at p < 0.05.
To compare the non-parametric measures with parametric measures, the means and standard deviations were presented.
M, mean; SD, standard deviation; t, t-statistics; Z, z-score.
Cohen's d: Adverse effect =< 0; no effect = 0.0–0.1; small effect = 0.2–0.4; medium effect = 0.5–0.7; large effect => 0.8.
The adolescent outcomes reported by the parents were also tested within groups. Adolescents whose parents were in the DaPI group showed a non-significant change in behavioral problems and emotional maladjustment. No significant changes were also observed in the WLC group.
Between-group analyses
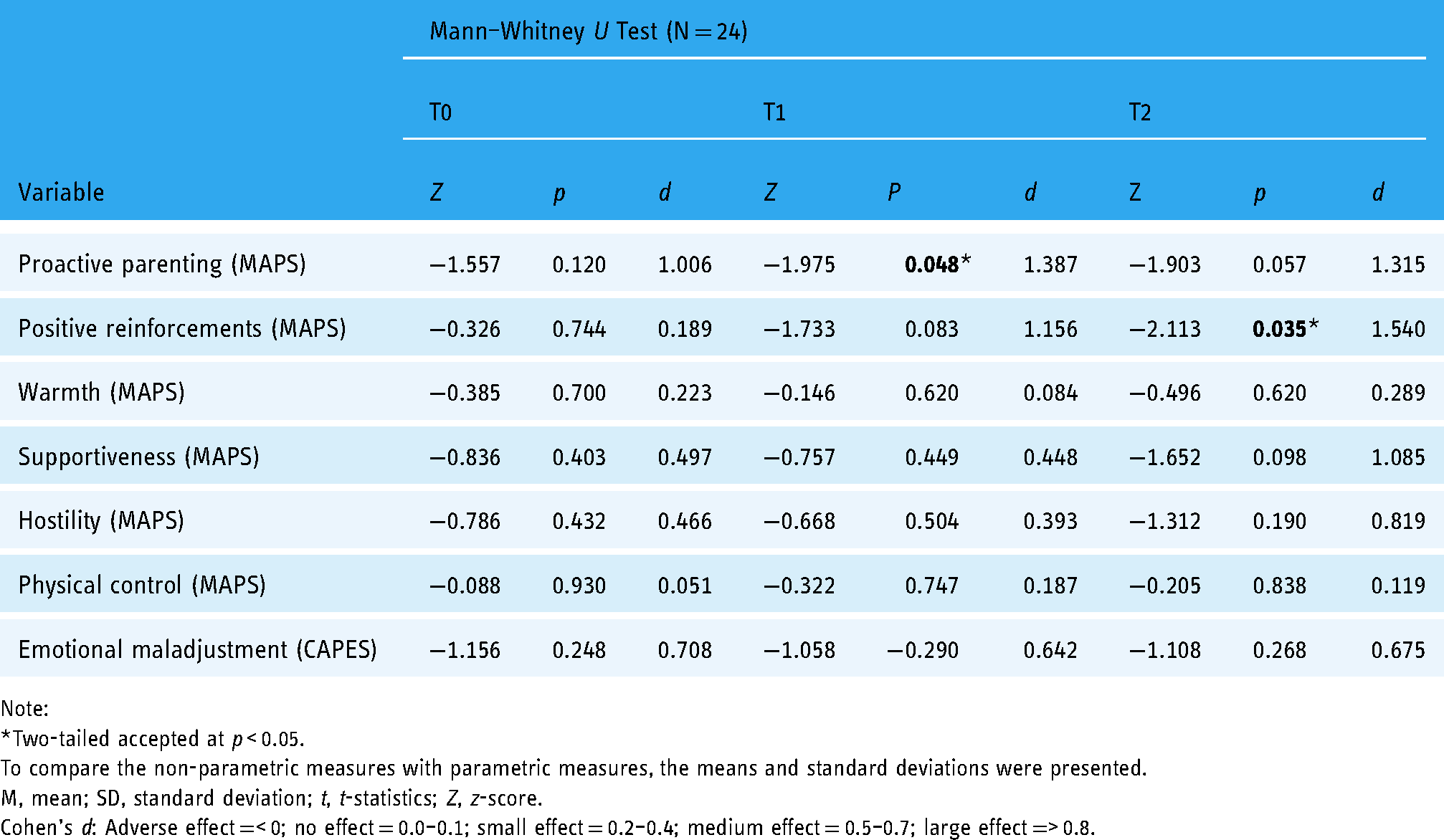
Between-group analyses were conducted at pre- and post-intervention and 1-month follow-up. The results from the pre-intervention analysis presented in Table 5 indicate no significant differences between the DaPI and WLC groups. Post-intervention analysis was then conducted to determine the effectiveness of the intervention. The results indicate a significant difference in the level of proactive parenting (Z = −1.98, p = 0.048, Cohen's d = 1.387), but not in other parental behaviors, parenting self-efficacy, and adolescent mental health measures. Cohen's d indicated that the improvement in proactive parenting in the DaPI group had a large effect size.
Between-group analysis between DaPI and WLC groups at pre-, post-, and 1-month follow-up.

Note:
Two-tailed accepted at p < 0.05.
To compare the non-parametric measures with parametric measures, the means and standard deviations were presented.
M, mean; SD, standard deviation; t, t-statistics; Z, z-score.
Cohen's d: Adverse effect =< 0; no effect = 0.0–0.1; small effect = 0.2–0.4; medium effect = 0.5–0.7; large effect => 0.8.
At the 1-month follow-up, the results demonstrated significant differences in the DaPI group for two parenting behaviors, that is positive reinforcement (Z = −2.11, p = 0.035, Cohen's d = 1.540) and lax control (t = −2.15, p = 0.043, Cohen's d = 0.878) with both indicating improvements. Cohen's d scores indicated a large effect size. There were no significant differences in adolescent behavioral problems and emotional maladjustment between the two groups at post-intervention and 1-month follow-up.
Discussion
This pilot study investigated the feasibility, acceptability, and initial effects of the newly developed DaPI in promoting mental health of adolescents aged from 10 to 14 years by changing their parents’ dysfunctional parenting and improving parental self-efficacy. Results highlighted specific aspects of the trial design and intervention that were feasible and that were not feasible. It is therefore important to modify the trial methods and intervention components before a fully powered RCT in a larger sample can be considered.
Compared to past local studies that recruited participants either from school, targeted neighborhood, and specific non-government organization, the present study recruited parents through online (social media platforms such as Facebook, Instagram and X) and offline (word of mouth) medium. Despite the recruitment efforts done and the monetary reward given at the end of intervention as well as at each assessment point, the number of participants interested in the pilot study were lower than anticipated. Low participation may be due to the lifting of the COVID-19 lockdown during the start of the pilot study, where parents were expected to go into the office in comparison to working online from home and children were back in school. Therefore, parents became unable to commit to an 8-week online program due to their busy daily schedule of balancing between work and home. As the program would require parents to participate in interactive activities, the cognitive workload may be taxing on parents. Furthermore, as online intervention is relatively new in Malaysia, these parents may not know how such program works. Moving forward, researchers may want to educate parents in general about how an interactive online intervention works in detail such as the total time needed to complete a session in a week, and the ability to save personal progress throughout the week. Information brochures and testimonial booklets containing photos and parent–child activities can be distributed to interested parents. Additionally, using recruitment strategies beyond those used herein may increase the number of participants and ensure greater diversity among parents. For example, researchers could consider mailing or emailing brochures about the intervention to various parent association groups and schools, placing flyers at local community venues such as libraries, family activity and leisure centers, attending public health and community events especially those relating to mental health, approaching general health practitioners for targeted referrals, and partnering with organizations that advocate for mental health.
Overall, the intervention components seemed to work well together. The high rates of session completion as well as at post-intervention and 1-month follow-up are promising in indicating the feasibility of the DaPI program. This could also be attributed to the weekly WhatsApp messages or email and monetary incentives given at each time point. Program acceptability was high. Parents reported satisfaction with the DaPI content on how it was simple, clear, and interactive, the amount of time needed to complete a session, and personalized feedback provided by the facilitator. Parents also felt that there were positive changes in their relationship with their children as they perceived that the content of the DaPI helped improve their parenting practices. As most of the digital parenting interventions have been developed, tested, and implemented in high-income and Western context, 67 results from this pilot study are a promising sign that an emerging middle-income, multi-cultural, Asian country finds digital parenting intervention to be feasible and acceptable.
Although this was a small pilot trial, we observed the initial effects of the DaPI program on parenting behaviors and parental self-efficacy in changing adolescent emotional and behavioral problems. As hypothesized, parents who received the DaPI reported significant improvements in parenting behaviors and parental self-efficacy. Specifically, parents reported a decrease in physical control at the 1-month follow-up. Furthermore, parents in the DaPI group reported a significant improvement in their parental self-efficacy at post-intervention and 1-month follow-up. Compared to parents in the control group, parents in the DaPI group reported an increase in proactive parenting at post-intervention, and an increase of positive reinforcement and a decrease of lax parenting at 1-month follow-up. These findings are consistent with those of previous studies that demonstrated the efficacy of universal parenting interventions in improving modifiable parenting behaviors68–70 and parental efficacy. 66 Furthermore, the current findings add to the local research investigating universal interventions for parents of adolescents. To the best of our knowledge, this is the first such study in Malaysia to be conducted entirely online with minimal support from therapists. Traditional parenting interventions are delivered by professionals in a face-to-face setting and are expensive to disseminate. The improvements in self-reported parenting behaviors and parental self-efficacy in this study hold promise for a more acceptable, accessible, and less-expansive universal parenting intervention.
Contrary to the expectation that universal parenting interventions will have a significant effect on adolescents’ mental health (i.e. emotional and behavioral issues),69,70 this study found no significant changes at post-intervention and at 1-month follow-up in the DaPI and WLC groups. Although the DaPI intervention helped improve parenting behaviors and parental self-efficacy, it did not have a significant impact on reducing emotional and behavioral problems of adolescents. There are several plausible explanations for these findings. First, data were collected only for the 1-month follow-up period. Although past studies have shown significant changes in adolescent outcomes at 1-month post-intervention,71–73 it is possible that the parents in this study required a longer timeframe to implement changes in their parenting behaviors that stimulate better outcomes for their adolescent children, especially in improving mental health. 74 As adolescent changes have been observed over time, these changes may be due to a decrease in harsh parenting and increase in positive parenting, which in turn foster healthy parent–adolescent relationships. 71 It is noteworthy that the adolescents in this pilot RCT were from a non-clinical sample and did not have high levels of emotional and behavioral problems at baseline (pre-intervention). A previous study hypothesized that adolescents with higher levels of emotional and behavioral problems would be more influenced by changes in parenting. 75
Limitations
The findings of this study have some limitations. First, all the outcome measures were based on parent reports. Future trials would benefit from incorporating different informants according to the research question, such as adolescent's self-reports on their emotional and behavioral outcomes. Second, the follow-up conducted 1-month post-intervention may not have been sufficient to observe any positive changes in adolescent outcomes, particularly in the non-clinical sample. 72 Future studies should examine the long-term effects of the intervention on parental behaviors and adolescent outcomes. Third, although this study invited parents of both sexes, only mothers responded to the study invitation. This restricts the generalizability of the results to other populations. Future studies should encourage fathers’ participation or allow both parents to participate in the intervention. Fourth, the LOCF method was chosen to impute missing outcome data despite its shortcomings of overestimating efficacy of treatment on a disorder hence leading to biased results. In view of the nature of the present study, that is universal parenting intervention conducted in a non-clinical sample, the application of LOCF is probably not harmful for generating reliable results. Nevertheless, future studies should imply other imputation methods to reduce treatment biasness. Lastly, although the current study's participants found the program satisfactory, retaining their participation was challenging, with consistent reminders sent to them for completing the program and online survey. Despite these efforts, a couple of mothers dropped out of the intervention for personal reasons.
Conclusions
The findings indicate that the DaPI, a universal technological-assisted parenting intervention, is feasible, acceptable, and beneficial for parents of early adolescents. Positive changes in dysfunctional parenting behaviors were observed in the parents receiving the intervention, and it is believed that these changes will affect their adolescent's emotional and behavioral outcomes over time. Overall, the trend from the study findings implies that DaPI is suitable for large-scale trials and can be implemented as a measure to promote good parenting behavior and practices subsequently curbing mental health problems in adolescents.
Footnotes
Acknowledgements
The authors would like to express our sincerest appreciation to all the participants of this pilot study who generously gave their time and effort to this project.
Contributorship
NSZ contributed to drafting, reviewing, and editing the manuscript. ARDS contributed to the recruitment of participants, literature review, statistical analyses, and drafting the manuscript. NAZ contributed to the recruitment of participants and aided the program implementation. FM was consulted regarding the operation of the RCT. RD contributed to the recruitment of participants. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from the Ethics Committee for Research Involving Human Subjects (JKEUPM-2021-161) of Universiti Putra Malaysia. The trial was registered in the Iranian Registry of Clinical Trials (IRCT20211129053207N1). The study findings will be disseminated at relevant national and international conferences and peer-reviewed scientific journals, and a final report will be provided to the Malaysian Ministry of Higher Education, the funding body. A brief report of the results will be emailed to the parents involved in the RCT upon request.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Higher Education, Malaysia (grant number FRGS/1/2020/SS0/UPM/02/8).
Guarantor
NSZ.