
Abstract
The aim of the study was to describe and explore public health nurses’ perceptions of involvement and their attitudes concerning the mental health aspects of their work in schools. Furthermore, we wished to explore their need for useful approaches and training topics. The teenage years in particular are associated with an incidence of mental health problems such as depression. Public health nurses in schools have an extensive role in relation to health promotion and the prevention of both physical and mental health. A cross-sectional study with 284 public health nurses from 163 municipalities in Norway was carried out, using the Depression Attitude Questionnaire. The public health nurses reported various degrees of confidence and time spent working with mental health issues. Confidence was found to be related to further education and courses.
Keywords
Background
The last decade has seen an increasing focus on child and adolescent mental health worldwide. 1 The teenage years in particular are associated with a high incidence of mental health problems such as depression.2,3 According to the Youth Study in Norway, which addresses mental health problems, this prevalence has increased since 2010 with 20% of the child and adolescent population reporting more depression and anxiety. 4 A depression is often persistent and relapses may occur – a debut in adolescence may be linked to risk of further episodes in adulthood. 5 Mental health problems, such as depression and anxiety, are strongly related to behavioural problems as well as problems related to social relations and school achievements.3,6,7 Several studies describe girls as being more vulnerable to stress, having lower self-esteem, a higher state of depression and anxiety and a lower sense of coherence than boys.8–10 Stress related to school performance is reported as strongly associated with depressive symptoms. 2 Studies show that pupils with emotional and mental health problems seek advice from friends and family and from professionals, such as teachers and public health nurses (PHNs).7,11
In Norway, every municipality is obliged to have a school health service to take care of the health of school-aged children and young people, as stated in the Act of Public Health from 2012. Public health nurses are professionals working in the school health service located in schools, and are among the first community health professionals who help to reduce health inequalities in the youth population. 12 Public health nurses in Norway are authorized nurses with a one-year postgraduate education in public health nursing 13 who have a particular responsibility for children of all ages, as well as adolescents and families, 14 in contrast to many other countries where PHNs provide services for the entire population. 15 They have an extensive role in relation to health promotion and prevention, and in detecting early signals of both physical and mental health problems. 13 A PHN is employed by the municipal community health service, and may have responsibility for one or several schools, which varies between different municipalities. A PHN meets most of the pupils through the school health service, with delivery of immunization programmes and screenings, followed by individual and group activities with pupils. Many PHNs have an open-door policy for pupils. 16 The PHN will, later in this article, be described as school nurse to make the context clearer. The recommended norm per full-time school nurse position is 300 students in primary schools, 550 in lower secondary schools and 800 in upper secondary schools. 17 The norm is not fulfilled in all municipalities. 17 The community health service for young people includes school nurses, general practitioners (GPs), mental health personnel and psychologists in some municipalities. The specialist health service has responsibility for the process of diagnostic assessment, treatment and follow up. Regulations require a school nurse to have routines for cooperation with GPs, personnel in schools, pedagogic psychological services (PPS) and the psychiatric specialist health services. 13
The changing healthcare system and new health challenges in the youth population may have changed the school nurse’s role and professional identity. 18 Mental health problems are not a key subject in the school nurse’s education. 13 In the curriculum, the main focus is on the children’s physical and mental development and health. The focus is clear with regard to paediatrics but less focused in mental health disorders. This may possibly influence the quality of the school nurse’s delivery of services to the child and youth population.
The aim of the study was to describe and explore school nurses’ perceptions of involvement and their attitudes concerning the mental health aspects of their work in schools. Furthermore, we wished to explore their need for useful approaches and training topics. Our research objectives were:
To describe school nurses’ perceptions of and involvement in emotional and psychological problems in children and young people. To explore and compare the attitudes of school nurses who, in addition, have completed a degree in mental health nursing with those who have not.
Methods
Design and sample
A cross-sectional study was conducted using a questionnaire sent by email. The internet survey software package Questback was used. A random sample of 703 PHNs in schools from all regions in Norway was included, with the inclusion criteria being working as a school nurse in schools with children and adolescents in the age range 11 to 18 years. The response rate was 40.39%, including 284 school nurses from 163 municipalities in Norway.
Data collection
Information about the study and a request for participants were sent to school nurse managers in municipalities in Norway by email. The managers supplied the email addresses of possible participants matching the inclusion criteria. An information letter was sent with the Questback questionnaire to the sample of school nurses. Those who wished to participate responded to the questionnaire, and three reminders were sent over a period of three weeks. The data collection took place from January to February 2016.
Measures and instruments
The questionnaire included questions regarding the background of the school nurses: age, gender, work experience as a school nurse, education as school nurse or not, a further degree in mental health nursing or not, courses in mental health issues, size of the municipality, job extent, number of pupils at the school and time spent on pupils with emotional or psychological problems. Ten items regarding views of useful approaches and training topics to assist mental health work were previously used and developed by Haddad et al. 7 The items were answered on a five-point response scale from 1 (not useful at all) to 5 (very useful). In addition, four questions were open-ended (to be reported elsewhere).
The Depression Attitude Questionnaire (DAQ) was developed by Botega et al. 19 and further developed to apply to school nurses and their work with adolescents by Haddad et al. 7 The questionnaire is a 20-item self-report questionnaire to measure the PHNs’ attitudes to working with pupils with depression. The items were on a 10-point response scale with the anchors defined as 1 (strongly disagree) and 10 (strongly agree). Previous examinations 7 with an exploratory factor analysis of the DAQ indicated three factors: ‘Professional ease and confidence’ (items 9, 12, 15), ‘Pessimistic attitude toward depression’ (items 7, 8, 10, 11, 16) and ‘Tendency to refer to psychiatric experts’ (items 17, 19, 20). In this study, the Cronbach’s alpha for the entire scale was 0.698, and for the three factors they were: ‘Professional Ease and Confidence’ 0.576, ‘Pessimistic attitude toward depression’ 0.498 and ‘Tendency to refer to psychiatric experts’ 0.548.
The questionnaire has not previously been used in Norway, and the translation process was inspired by Yu and Lee’s description of back-translation. 20 The instrument was translated from English to Norwegian by a bilingual expert in the topic and back-translated by another bilingual expert. A team of experts in mental health and public health nursing commented on the clarity of the instrument and further clarifications were made. The instrument was pilot tested with 10 nurses, and some formulations were clarified, thereby making them more understandable.
Data analysis
Statistical analyses were performed using IBM Statistics SPSS, version 22.0, and descriptive statistics with frequencies, percentages, means and standard deviations were used. Comparisons between groups were analysed using independent sample t-tests, a one-way analysis of variance (ANOVA) and a Kruskal–Wallis test. Post hoc tests, such as a Tukey’s HSD and Mann–Whitney U-test, were used to find out where the differences between the groups occurred. The internal consistency for the whole scale and for the factors was measured using Cronbach’s alpha. 21 All tests were two-tailed with a p-value < 0.05.
Ethical approval
The study was approved by the Norwegian Social Science Data Services (NSD) (ref: 45366). Ethical research principles were followed during the entire research process. 22
Results
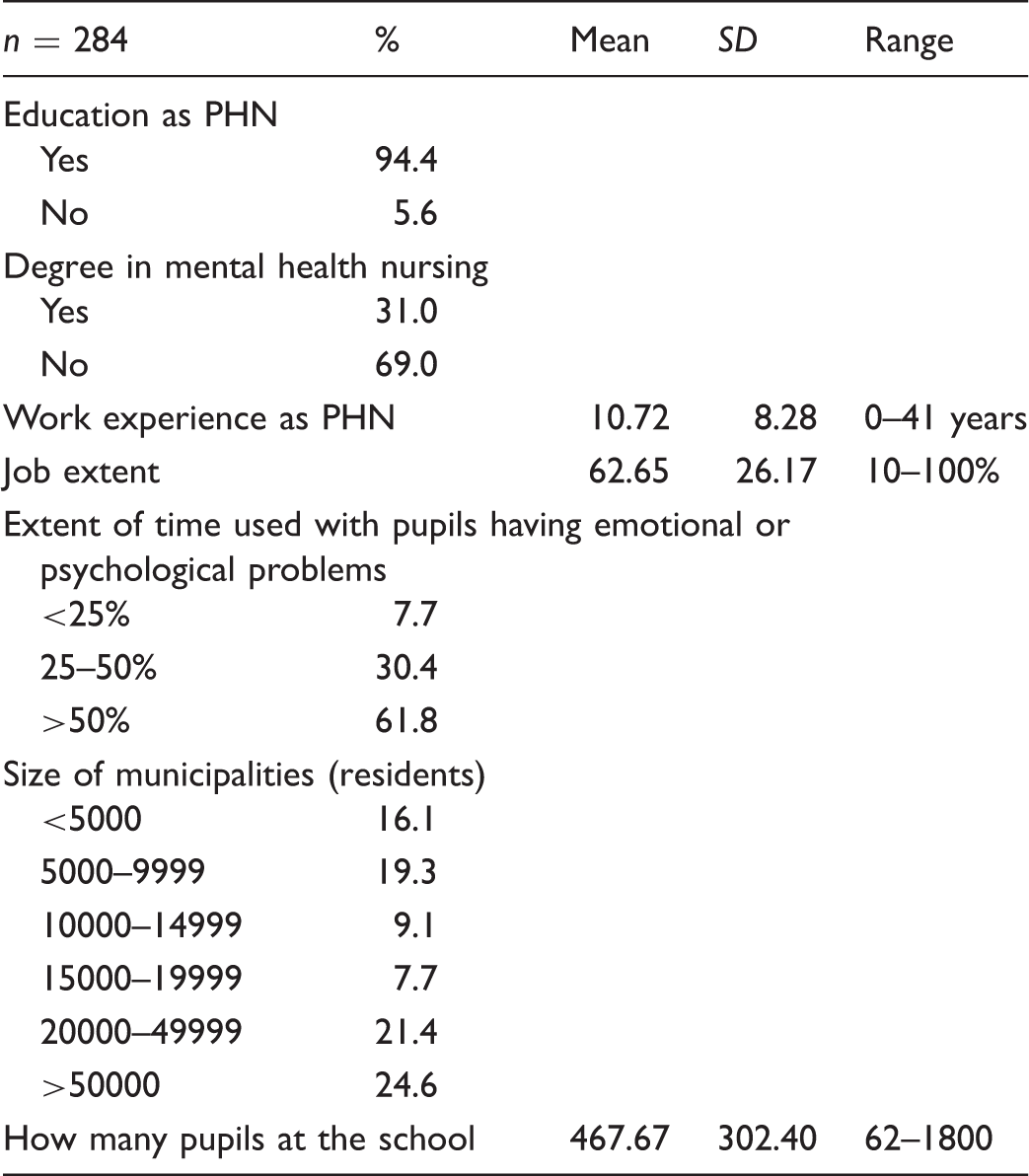
Background of the public health nurses (PHNs).
Public health nurses’ (PHNs’) priorities for approaches and training topics to assist in mental health work.
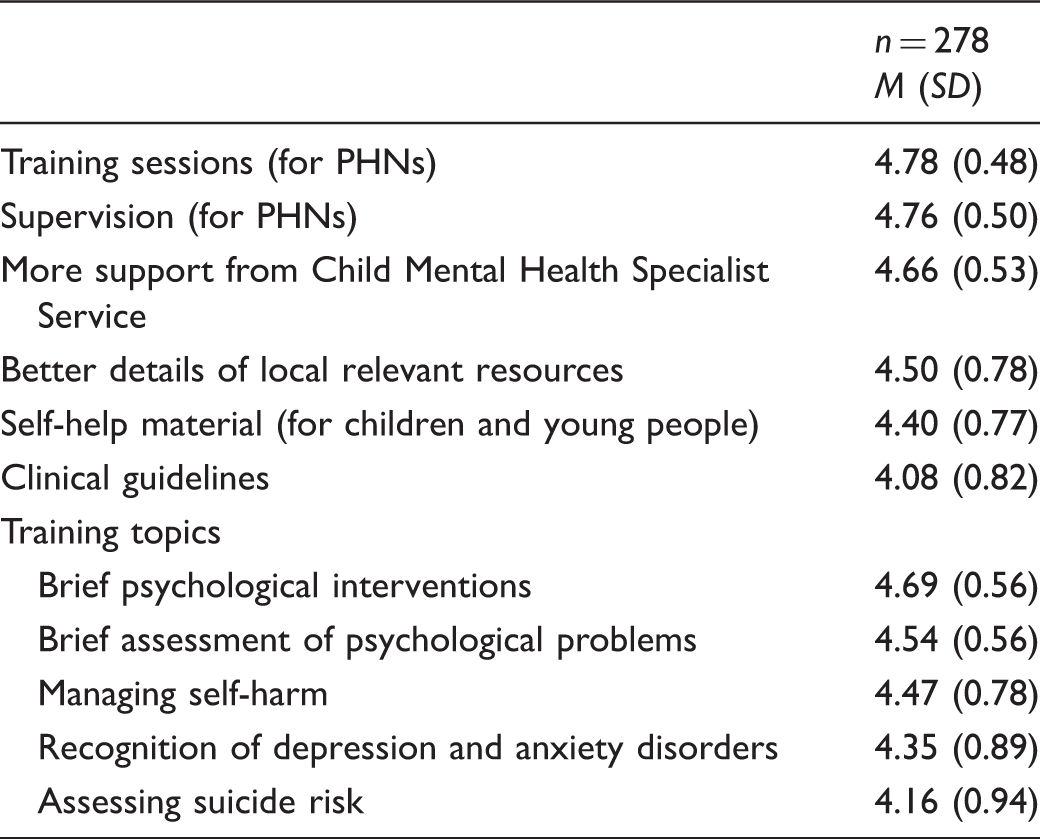
Note. Answered on a five-point response scale from 1 (not useful at all) to 5 (very useful).
To compare the group of school nurses with the group of school nurses with a degree in mental health nursing regarding their views of useful approaches, a Student’s t-test was conducted. There was a significant statistical difference between the groups of PHNs regarding ‘training sessions for school nurses’, with the group of school nurses without a degree in mental health nursing (n = 196) wanting more training sessions (M = 4.85, SD = 0.63), than the group of school nurses with a degree in mental health nursing (n = 88) (M = 4.60, SD = 0.37, t = 4.25, p = 0.001). There were also significant differences in ‘brief assessments of psychological problems’ between the group of school nurses without a degree in mental health nursing, who found assessments more useful (M = 4.60, SD = 0.67) than the group of school nurses with a degree in mental health nursing (M = 4.41, SD = 0.72, t = 2.10, p = 0.037). Furthermore, significant differences were also found when comparing those who had a degree in mental health nursing, who found it less necessary to have ‘training sessions for school nurses’ (M = 4.60, SD = 0.64) than school nurses having attended brief courses regarding mental health issues (M = 4.86, SD = 0.37, t = 3.35, p = 0.001). Between these two groups, there was also a significant difference in ‘brief assessments of psychological problems’, with those with a degree in mental health nursing finding it less necessary (M = 4.38, SD = 0.73) compared to those having attended brief courses in mental health issues (M = 4.59, SD = 0.67, t = 2.34, p = 0.02).
The one-way ANOVA test was used to explore differences in work experience and revealed significant differences between those with less work experience as a school nurse (0–2 years) (M = 4.77, SD = 0.71) compared with the group having the most work experience (21–41 years) (M = 3.35, SD = 0.70, F = 2.45, p = 0.047). Those with less work experience reported the need for more brief assessments, brief interventions and training sessions.
There were no significant differences in the school nurses’ views on useful approaches and training topics with regard to the extent of their work at schools.
Public health nurses’ attitudes towards depression.
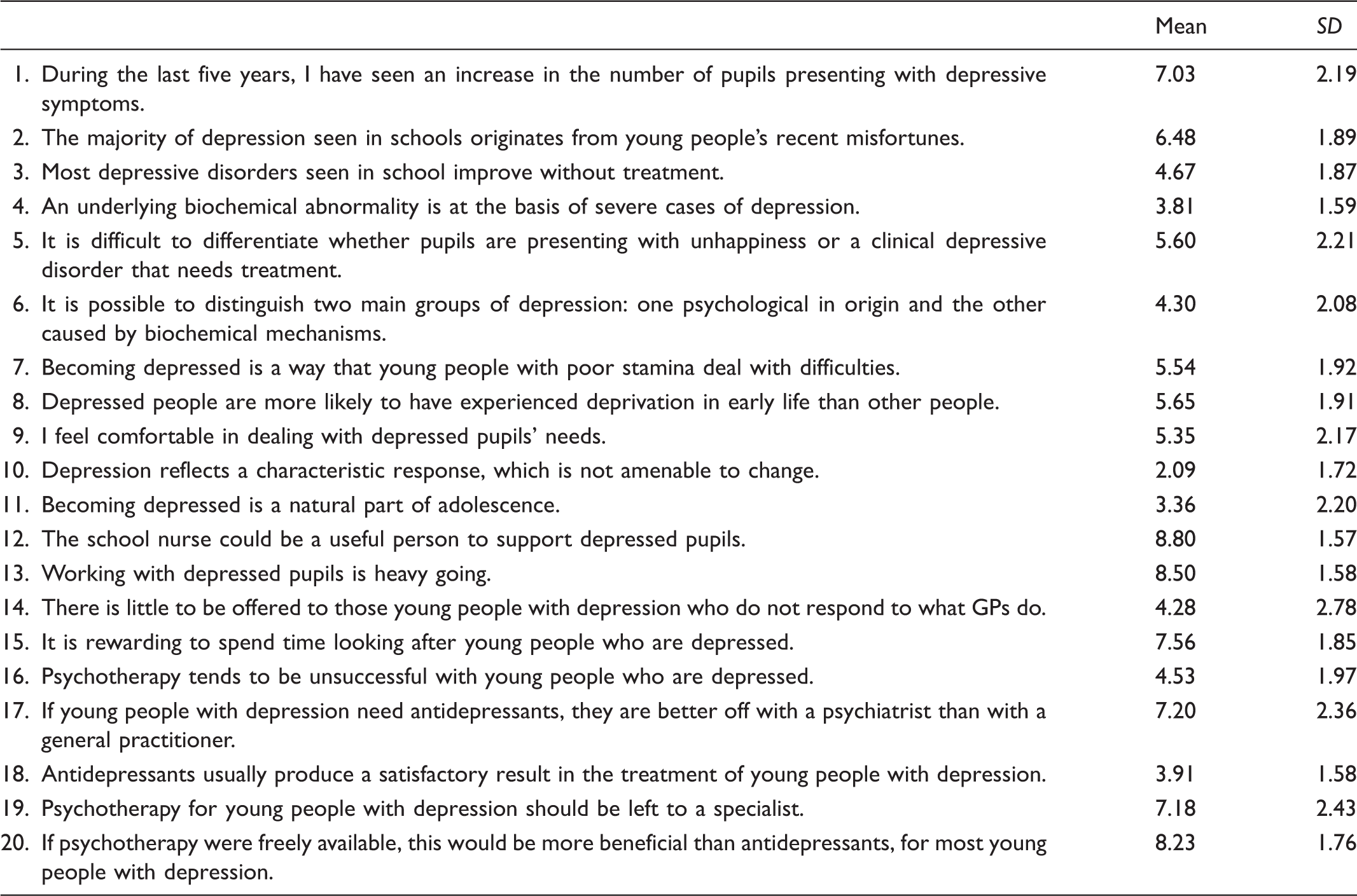
Depression attitude questionnaire answered on 10-point response scale from 1 (strongly disagree) to 10 (strongly agree).
When comparing the group of school nurses with a degree in mental health nursing with the group of school nurses without this degree, we found significant differences in the factors described as ‘Professional ease and confidence’. The group of school nurses with a degree in mental health nursing reported a higher degree of agreement with this factor (M = 7.67, SD = 1.22) than those without this degree (M = 7.06, SD = 1.42, t = 3.40, p = 0.001). The factor ‘Tendency to refer to psychiatric experts’ showed that the group of school nurses with a degree in mental health nursing demonstrated a significantly reduced tendency to refer pupils (M = 7.14, SD = 1.66) compared to others (M = 7.67, SD = 1.58, t = 2.52, p = 0.012).
Comparing the factor ‘Professional ease and confidence’ and time spent with pupils suffering from psychological and emotional problems.

Group A: Less than 25% of their time; Group B: Between 25% and 50% of their time; Group C: More than 50% of their time.
Factor 1 from the DAQ: ‘Professional ease and confidence’ (items 9, 12, 15), answered on a 10-point response scale from 1 (strongly disagree) to 10 (strongly agree).
The school nurses who spent less than 25% of their time working with pupils’ mental health issues felt less confident in helping pupils with psychological and emotional problems.
Discussion
The results of this study showed that most of the school nurses spent more than 25% of their time in dealing with pupils with mental health problems. This finding is also supported by Dahl and Clancy, who reported that school nurses had much experience related to mental health work. 18 Results in Table 2 show that the school nurses felt that they played a useful role in supporting depressed pupils. The school nurses do not diagnose mental health problems, but instead make a nursing judgement related to mental health issues. 23 To be a supportive adult with a professional relation to adolescents with depression may be an important role for the school nurse. The school nurses have to depend on their clinical judgement as to whether they can handle such problems themselves before consulting and referring to a mental health specialist or involving the parents. 23 They also perceive working with adolescents with depression as being hard work (see Table 3). Support and supervision from other school nurses may ease the burden when working with these youths. Pupils often consult the school nurses with physical or psychosomatic issues such as a headache, stomach ache or other medical complaints that give the school nurses a gateway into the pupils’ mental health issues.23,24 Most school pupils may have depressive thoughts related to the experience of being an ordinary young person who is not unhealthy but who nevertheless needs to speak to a professional. Others are in a stage of early development of mental health problems; these pupils may need referral to special mental health services. As part of their job responsibility, the school nurses must meet all young people, regardless of their mental or physical health. They do not necessarily need to have a further degree in mental health nursing, but they need to be able to cope with their work. 25 Only a small part of the curriculum for the one-year programme of further education as a school nurse is related to mental health problems. When comparing the group of school nurses with the group of school nurses with a degree in mental health nursing, those with a degree in mental health nursing as well as education as a school nurse, reported more professional ease and confidence, as well as a reduced tendency to refer to a mental health specialist. The curriculum in the school nurses’ education programme in Norway may be questioned. 25 Has this changed to reflect the increase in mental health problems in adolescents and the central role school nurses have in supporting them? In addition, school nurses who spend more than 25% of their time in helping youths with emotional and psychological problems also felt a greater sense of professional ease and confidence. In this study, we have no information as to whether those spending less than 25% of their time gave this lower priority due to a lack of time, knowledge or interest in these topics.
Furthermore, the work experience of the school nurses in this study varied, with some having worked almost a decade, while others had recently graduated. Because many of the school nurses had been educated several years ago, changing the education programme is not sufficient. Standardized training courses with a focus on brief psychological interventions and a brief assessment of psychological problems may be one solution, helping school nurses to judge which pupils need referral to collaborative partners and which pupils they can manage to help and support on their own. 26 On the other hand, if too many interventions from the community health service are implemented before referral, the adolescents’ problems become severe, as described by school nurses in a qualitative study. 27 The school nurses may need decision-making tools and standardized courses to make decisions that benefit young people with mental health problems.
Training sessions were ranked as most important for the entire group of school nurses, with brief psychological interventions and a brief assessment of psychological problems as most important for the training sessions. The focus of school nurses is to prevent sickness and promote health. 28 School nurses use a variety of different evidence-based interventions, e.g. Dahl and Clancy 18 describe one communication technique influenced by sense of coherence, 29 which motivates one to cope, understand a challenge and believe in available coping resources. Clausson and Berg used family intervention sessions to improve schoolchildren’s mental health. 24 Garmy et al. evaluated a universal school-based programme employing cognitive-behavioural strategies. 30 There is no standard intervention or school programme available, while the health authorities have no specific intervention for all PHNs to follow. This may lead to inequality in health provision depending on the municipality or on which school nurse young people consult. More standardized interventions and brief assessments are needed in the school nurse’s work.
In this study, supervision was reported as the second most important of the approaches and training topics for the school nurses, and may be a way to reflect and anonymously discuss cases in which they are involved. While under supervision, they can benefit from each other’s experience: some have a further education in mental health nursing and a large amount of work experience while others have a smaller amount of work experience but more recent education as a school nurse. Dahl and Clancy found that school nurses described themselves as being generalists, ‘knowing a little about a lot’. 18 Tacit knowledge must come to clarity when school nurses develop clinical judgement and awareness.31,32 Supervision may be one answer to the question of how to strengthen school nurses and highlight tacit knowledge. 27 Under supervision, school nurses may also support each other in difficult cases involving young people with mental health problems. Furthermore, this study shows a wide range in work experience as a school nurse, so that experience and knowledge exchange can play a major role in supervision.
Increased support from the Child Mental Health Specialist Service was ranked as the third most important topic in this study. Clancy et al. found in their study that mental health professionals in the primary health service were the professions that were most missed in school nurses’ collaboration with municipalities. 33 Some of the answers to the 20 questions regarding attitudes to depression confirm that school nurses may not be professionally confident in dealing with adolescents with depression. A decision-making tool may help school nurses to be more systematic in their work and may make it easier to describe young people’s problems in the encounter with the specialist health service. 26 Clancy et al. found that to achieve a successful collaboration, relational factors such as trust, respect and collaborative competence are important. 33 In addition, trust was ranked highly, demonstrating that relational factors are more important than political directives or organizational structures.
These findings highlight the focus on school nurses’ experiences, involvement and attitudes when working with youths with mental health problems. Norwegian policy requires school nurses to work at both the group and individual level with youths and their families. 34 School nurses’ working conditions, regarding job extent, school size and availability for the pupils, vary in Norway. Perhaps this service is under-communicated. There is a shared but false notion that all mental health interventions are complex and can only be delivered by specialized personnel. 35
Strengths and limitations
This study has both strengths and limitations. In spite of three reminders, the response rate in the study was only 40.4 %. The generalizability must therefore be interpreted with caution, although a low response rate is common in many online research studies. 36 This may reflect that those with an interest in the topic are the ones who respond to these kinds of studies. School nurse managers in municipalities recruited school nurses for the study, and there were clear inclusion criteria that strengthened the study. The school nurses who participated were from different municipalities in Norway, representing both the big cities and the more rural municipalities, thereby reflecting school nurses in a general Norwegian context.
The instrument is well known and has been used in different samples and tested for validity and reliability. 7 The Cronbach’s alpha coefficient for the DAQ was 0.698, thus showing good stability. 37 Regarding construct validity, the Norwegian version should be further tested psychometrically due to possible cultural differences. 38 The translation process was rigorous, the instrument was tested for face and content validity by a panel of researchers, and no revisions were made.
Conclusion and recommendations for further research
Overall, the school nurses reported a need for training sessions, supervision and more support from the Child Mental Health Specialist Service. Those with further education and courses in mental health nursing reported more confidence in their work. School nurses spending less than 25% of their time in dealing with mental health issues in youths reported being less confident. There are large geographical disparities concerning the school nurse’s role in a Norwegian context. In the future, the curriculum in the Norwegian education programme for school nurses may be changed to meet the increase in mental health problems among young people. Furthermore, to secure the quality of the service, a national knowledge platform among school nurses is needed and must be developed in respect of mental health issues. The extent of coverage and the utilization of the school health service could be the key to adolescents’ mental health. Further research is needed to explore and describe the school nurses’ experiences, knowledge and attitudes when working with youths and young people with mental health problems, in addition to developing evidence-based interventions school nurses can use in their daily work.
Author contributions
Study design: ØLM and HSK; data collection; ØLM and HSK; data analysis: ØLM, manuscript preparation: ØLM and HSK. Both authors have seen this last version and agreed upon it.
Footnotes
Acknowledgement
We would like to thank Nils Rui for valuable help concerning the use of Questback.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.