
Abstract
The effects of perioperative dialogue have been studied using qualitative methods, describing patient satisfaction with their care. However, they have not been studied in patients with peritoneal carcinomatosis who undergo major surgery, nor with quantitative variables. The aim was to study the use of pain medication and length of hospital stay following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in patients who received, versus those who did not receive, perioperative dialogue. The study had a quantitative, retrospective and comparative design including 89 audits. Of these, 37 patients received perioperative dialogues, and 52 patients did not (the control group). The result showed that by postoperative day six, patients who received a perioperative dialogue experienced pain less frequently than patients in the control group. However, no differences between the groups were noted with regard to pain medication consumption and length of hospital stay. To ease their worries, all patients in both groups used benzodiazepines. The perioperative dialogue may be studied quantitatively, but it must involve the patient, who is an equal partner in the dialogue. Structured validated self-reporting measures may be used systematically before and after surgery in order to evaluate the perioperative dialogue using quantitative measures.
Introduction
The overall goal for perioperative care is individualized and professional attention for each patient when they must undergo a surgical examination, treatment or surgery. The perioperative dialogue (PD) is a part of perioperative care and is a caring model influenced by Eriksson’s theory of humanity, health, suffering and caring towards a more humanistic way of thinking.1,2 The PD is defined as a conversation between the perioperative nurse (operating room or nurse anaesthetist) and the patient, which takes place preoperatively, during the surgical procedure (intraoperatively) in the operating room, and postoperatively after the surgical procedure.3–6 Without this perioperative approach, patients meet a perioperative nurse for the first time on the day of surgery in the operating room shortly before anaesthesia. Through the PD, the perioperative nurse is given the opportunity to implement person-centred care (PCC)7–10 during the surgical procedure, which in the perioperative context is defined as recognizing the patient as a unique entity, who is allowed to be the person he or she is. It also acknowledges the patient as important by taking his or her personal wishes into consideration before, during and after the surgical procedure. 11 Furthermore, PCC means having full access to one’s own nurse, who offers closeness by touching the patient, and promising the patient to be present at all times during the surgery and the perioperative process.11,12 In view of this, the PD provides an opportunity for a joint meeting and sharing of experiences and feelings between the patient and the perioperative nurse, based on an overall perspective of patients’ needs and a more humanistic view of the patient. The PD offers a chance to inform and to better prepare the patient before the surgical procedure, and to let the patient ask questions 12 in order to calm the patient and reduce experience of anxiety or worries which could influence their postoperative pain. The purpose is for the patient to meet the same operating room or nurse anaesthetist throughout anaesthesia and surgery, to create a relationship, and establish trust. 13 This is extremely important before anaesthesia and the surgical procedure – a time when the patient places control of his or her body into the hands of the operating room or nurse anaesthetist, 13 the anaesthesiologist and the surgeon.
Preoperative anxiety or worries have been found to influence the experience of immediate postoperative pain. Patients with higher levels of preoperative anxiety or worries can be expected to experience higher levels of postoperative pain, both in hospital and at home. 14 The greater the concern that a patient feels before the surgery, the more pain they experience after surgery. 15 Postoperative pain can be seen as a stress factor that stimulates increased acknowledgment contributing to continuation of ‘the cycle of pain-anxiety’.14(p.421) Fearon et al. have studied a multidisciplinary team approach that focused on stress reduction and promotion of a return to everyday function. 16 In their study, it appeared that good preparation before the surgery, where patients were involved and received detailed information, could speed recovery and thereby shorten the hospital stay. Many patients felt that they received sufficient information about pain and pain management. However, lack of opportunities to discuss concerns and fears led to postoperative pain in many patients despite their being well informed. 17
Patients with peritoneal carcinomatosis (PC) suffer from cancer tumours in the abdomen that have their origin in different organs, e.g. the colon, small intestines, rectum, ovaries, and peritoneum. Untreated, PC is considered a lethal disease. 18 During the past 30 years, patients have been successfully treated using a method called cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC). This means that during the extensive surgical procedure, tumour burden is counted with a PCI score (Peritoneal Cancer Index); all visible tumour cells are removed from the abdomen during cytoreductive surgery (CRS), and heated chemotherapeutic agents are administered into the abdomen (HIPEC). 19 Treatment with CRS and HIPEC, which is considered a curative option, is challenging for patients both during and after surgery, and it has an impact on postoperative recovery mentally and physically.20,21 Therefore, patients undergo a thorough selection process before surgery. 19 The waiting time for surgery is long and postoperative recovery also takes a long time.20–22 During the postoperative period, both in the early (before discharge) and late (after discharge) recovery phases, 23 patients need psychosocial support and other, practical forms of support. 24 Patients with PC describe having anxiety or worries before surgery and for a long time afterwards.20,21
Kruzik indicated that the PD may have a positive effect on worry before surgery and on postoperative progress. 25 It may therefore be beneficial for patients who go through extensive surgery such as CRS and HIPEC to be offered PD. The hypothesis is that if patients feel safe and comfortable after discussing their needs with the perioperative nurse, this could result in their feeling calmer and more comfortable. Thus they would need fewer pain medications and psychopharmaceutical agents, and hospitalization would be shorter. Patient satisfaction when their care includes PD has been studied using qualitative methods. 26 However, no studies have investigated whether PD can influence pain and anxiety or worry in patients with PC, as measured using quantitative variables such as the use of pain medication and psychopharmaceutical agents as outcome variables.
Aim
To study the use of pain medication and length of hospital stay following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in patients who received perioperative dialogue versus those who did not.
Method
Design
The study had a quantitative and retrospective design, comparing patients with PC who received perioperative dialogue with those who did not, and undertaking a review of patients’ electronic medical and nursing records.
Study sample
The group receiving PD contained 37 patients who received perioperative dialogue as part of their clinical procedures between 2007 and 2009. The control group included 52 patients between 2010 and 2012 who received no perioperative dialogue. At that time, PD was not a standard part of clinical procedure because there was a different organizational structure in the surgical department. A consecutive sample of 89 electronic medical and nursing records of patients who underwent CRS and HIPEC in a university hospital in Sweden were selected for review. Of these, 37 patients received a perioperative dialogue with an operating room or nurse anaesthetist from the surgical team and 52 patients did not. The inclusion criteria were patients with PC who underwent CRS and HIPEC. Exclusion criteria for both groups included electronic medical and nursing records of patients who had had an acute or elective re-operation, as well as patients who were under the age of 18 and patients who received only a pre- or postoperative dialogue. Procedures were otherwise similar. Most patients included in this study were from Swedish counties at some distance from the university hospital, and hence had been referred from their local hospital. This meant that some patients had to return to their local hospital for further postoperative rehabilitation after the first postoperative period in the university hospital.
Setting and the perioperative dialogue
During the data collection period, patients with PC were diagnosed and treated at a university hospital in central Sweden. Two patients were scheduled for surgery per week and patients were usually admitted to the hospital one or two days before the surgical intervention.
The perioperative dialogue was offered by an operating room or a nurse anaesthetist working in the team that was caring for the patients with PC, which made it possible for the patients to have PD with the same nurse before, during, and after surgery. The perioperative dialogue the day before surgery took 30–60 minutes. The PD was performed following a protocol of information about anaesthesia and explained different procedures and variables that would be monitored during the surgical procedure. Information was provided about surgical wound care and patients’ questions were answered. During the PD the nurse also asked questions about the patients’ preferences and needs in order to involve the patients in their own care. The PD aimed to create a trusting relationship between the patient and the nurse.3,13,26 Data concerning pain were assessed and documented using the Numeric Rating Scale (NRS). Each patient’s self-reported anxiety or worries were documented as descriptive data. Length of hospital stay was recorded as the number of days stated in the patient’s electronic medical and nursing records by the nurses on the surgical ward.
A thoracic epidural catheter was inserted and activated, usually with bupivacaine and sufentanil (and in some cases with narop) before general anaesthesia. General anaesthesia was induced with fentanyl and sodium thiopental. Patients had continuous support from epidural analgaesia for eight days postoperatively 27 and this was supplemented with paracetamol and other pain medications if necessary. Thereafter, patients were offered patient-controlled analgesia (PCA) with an opiate, which meant that patients could control the intake of their pain medication themselves to a certain extent.
Data collection
The review protocol, which was designed specifically for this study, included demographic variables such as the patient’s age, gender and family status, and whether or not the patient had received PD. Variables that were associated with the disease such as diagnosis, number of days between diagnosis and surgery, 28 tumour burden (PCI score range 1–39), 28 and length of hospital stay 16 were included in the protocol. The protocol also included variables concerning the patient’s pain medication and psychopharmaceutical drug consumption, and pain estimation levels, NRS > 3 seven days postoperatively. The NRS scale consisted of a horizontal 10 cm line between the phrases ‘no pain at all’ at point zero and ‘the worst pain’ at point 10. 29 Pain was a self-reported variable which was documented by patients themselves in a structured protocol. This information was then transferred into the patients’ electronic nursing records by the postoperative ward nurses. According to the quality guidelines and indicators for pain management at the hospital, patients with an NRS pain rating > 3 should be treated pharmacologically. 30 Variables associated with pharmaceutical consumption, such as the name of the pharmaceutical drug, the dose given, as well as the method of administration, number of days the drug was administered and the number of doses, were all recorded. Variables about patients’ self-reported worry about surgery, the use of tranquilizers and whether the patient had contact with a counsellor or a hospital chaplain were also recorded in the review protocol. This study was based on the nurses’ documentation of patients’ comments, descriptions and feelings. The documentation was carried out by the nurses and placed in the patients’ electronic nursing and medical records.
Data analysis
Descriptive statistics were used for demographic data. Chi-squared was used to test the effect of PD on the usage of psychosocial support. Mann–Whitney U tests were used to answer questions about the amount of psychopharmaceutical and pain medications, or whether the PD had an impact on length of hospital stay. Data were analysed using IBM SPSS statistics version 20.0. Statistical significance was inferred at p < 0.05.
Ethical considerations
The study was approved by the Ethics Committee of Uppsala University’s Faculty of Medicine (Dnr 2012/542) and followed both the Declaration of Helsinki and Swedish national ethical guidelines.31,32 Although there are advantages to patients having the PD with the same operating room or nurse anaesthetist before, during and after surgery, the PD was not offered to all patients at all times due to organizational changes in the surgical department. However, this was a description of everyday/real life in the department during the study and it was valuable to study whether the PD had had any impact on consumption of pain medication or hospital stay.
Results
Background data and comparison between patients who received a perioperative dialogue and patients who did not receive a perioperative dialogue (control group), n = 89.
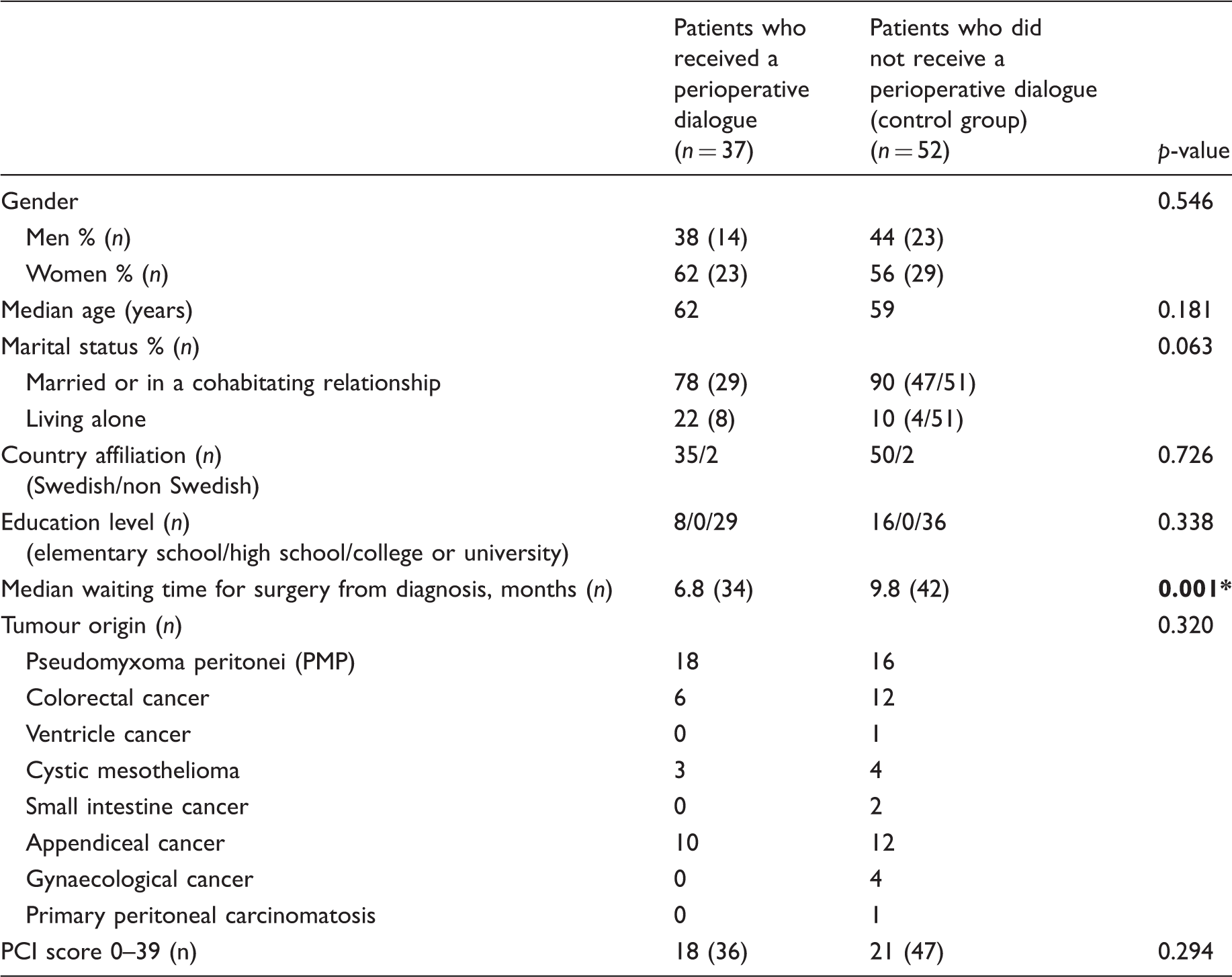
PCI: Peritoneal Cancer Index. Values in bold font: significance of difference between patients who did and did not receive a perioperative dialogue: * p<0.05.
Postoperative pain management
Number of times pain assessment NRS > 3 was recorded for patients who received a perioperative dialogue and patients who did not receive a perioperative dialogue (control group), n = 89.
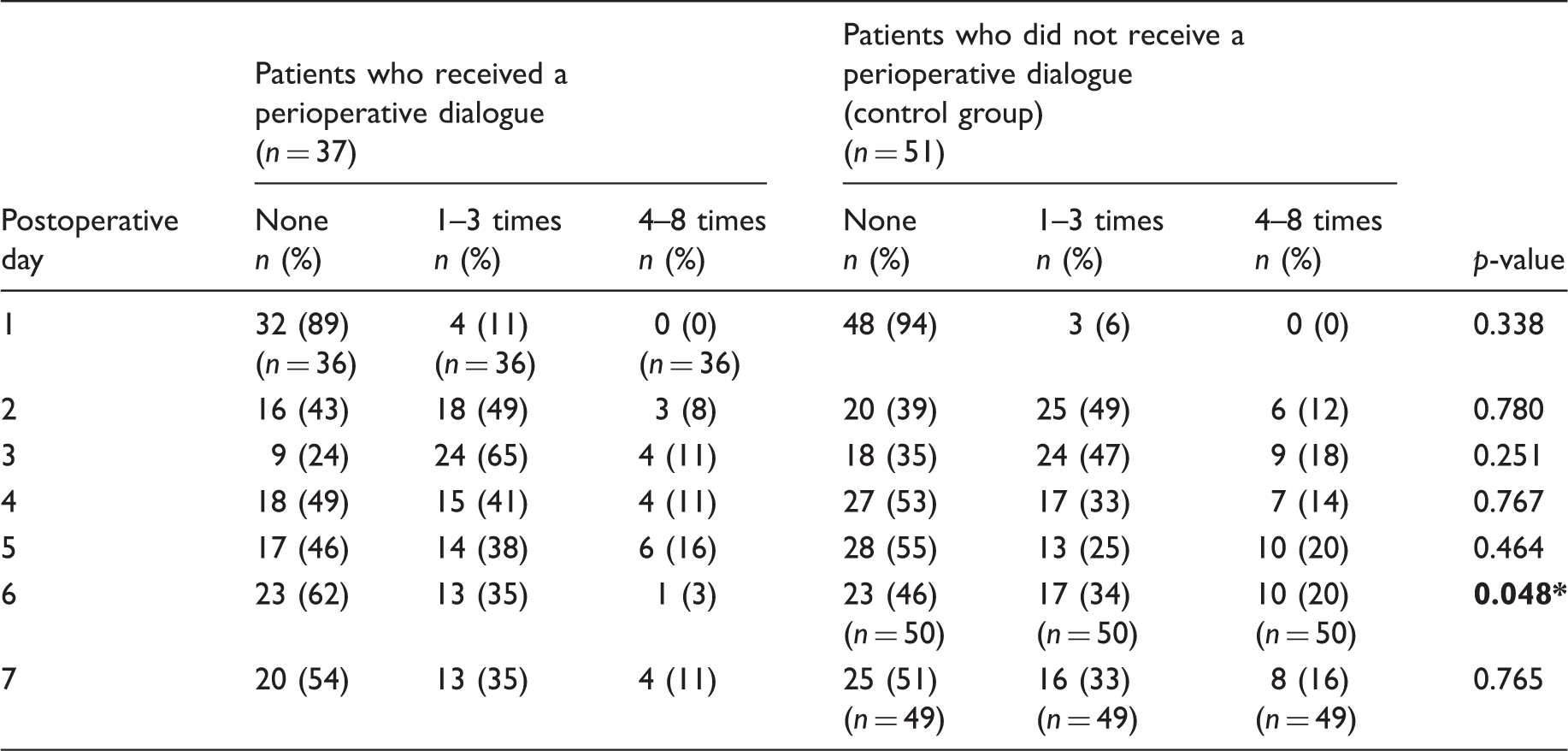
Note: The statistical analysis was performed using the Chi-squared test. Values in bold font: significance of difference between patients who did and did not receive a perioperative dialogue: * p<0.05.
One patient in the control group did not assess pain according to the NRS scale during the first seven postoperative days. A comparison between the group who received a perioperative dialogue (n = 37) and the control group (n = 51) during postoperative day six indicated a difference between the groups in the number of times pain assessment NRS > 3 was recorded. Those who had received a PD were assessed less often for pain (Chi-squared test, p = 0.048).
Analgesia consumption, dosage given (mg) as well as method of administration, number of days the drug was administered and the number of doses in patients who received a perioperative dialogue and patients who did not receive a perioperative dialogue (control group), n = 89.
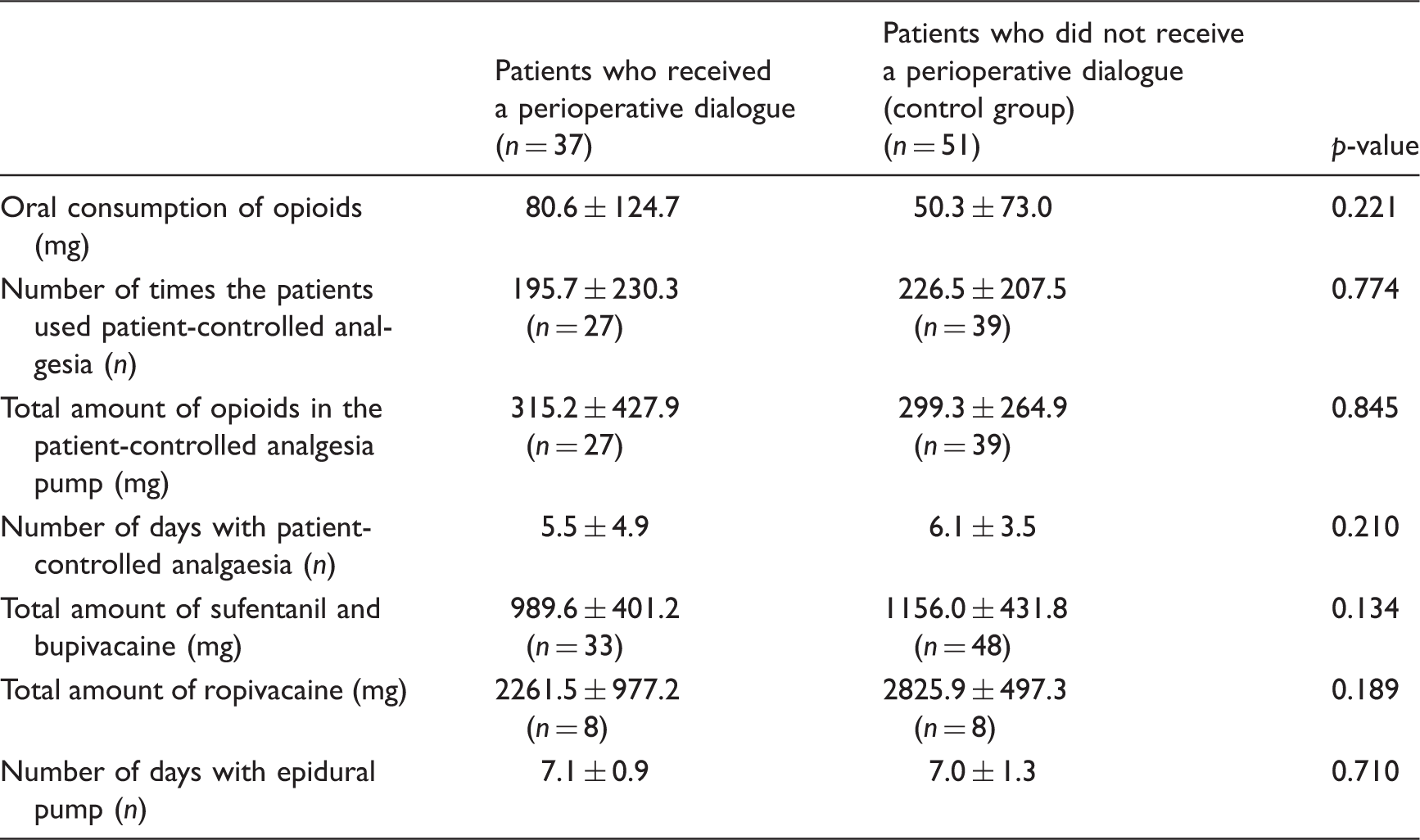
Note: The statistical test used to compare the intervention and control groups was the Mann–Whitney U test.
Psychosocial support and usage of psychopharmaceutical agents
According to self-reported anxiety or worries in the patients’ records, 24 (27%) of the patients had anxiety or worries during their hospital stay. Fourteen patients (16%) had no anxieties or worries and 51 (57%) could not decide whether they had any anxieties or worries or not. There were no differences between the group who received perioperative dialogue and the control group regarding psychosocial support. Eight per cent (n = 3) of the patients in the group who received a perioperative dialogue and 13% (n = 7) in the control group contacted a social worker or hospital chaplain after their surgical procedures. However, all of the patients, i.e. 37 patients in the group who received a perioperative dialogue, used benzodiazepines 11 ± 37 mg and 52 patients in the control group used benzodiazepines 12 ± 54 mg to help cope with their anxiety or worries during their hospital stay.
Length of hospital stay
There was no difference between the group who received a perioperative dialogue and the control group in terms of the length of hospital stay. In the group who received a perioperative dialogue, patients stayed in the hospital an average of 11 days versus the patients in the control group, who stayed an average of 12 days.
Discussion
On postoperative day six, there was a difference in the number of pain assessments at NRS > 3 recorded in patients’ electronic medical and nursing records, which showed that patients in the group who received a perioperative dialogue had pain less frequently than the patients in the control group. However, no differences were noticed between the group who received a perioperative dialogue and the control group with regard to pain medication consumption, i.e. how many mg were given, as well as the method of administration, number of days the drug was administered, the number of doses, and the length of hospital stay.
In their self-reported documentation, the majority of the patients could not decide whether they had any postoperative anxiety or worries or not. Postoperative anxiety or worries were only documented in 27% of the patients’ electronic medical and nursing records. Despite that, only 8% in the group who received a perioperative dialogue and 13% of the patients in the control group had taken the initiative to talk with a social worker or hospital chaplain after surgery. Earlier studies20,21 have illustrated that patients actually had thoughts and worries but did not want to burden their families by sharing these with them. This could possibly be understood by the fact that, in this study, both groups used benzodiazepines to ease their postoperative anxiety or worries. However, the result revealed no difference between those who received a perioperative dialogue or the control group with regard to having worries or the consumption of benzodiazepines.
Psychological wellbeing was not a variable that was recorded systematically in the patients’ files. Despite the serious diagnosis and demanding surgical procedure, neither depression nor anxiety or worries were measured by a validated instrument, either at baseline upon admission to the hospital or continuously during postoperative recovery. This is remarkable since these patients were seriously ill and scheduled to undergo major surgery. According to a study by Ayuso-Mateos et al. 33 the prevalence of depressive disorders among the general population in five European countries was 8.56% and a meta-analysis by Stenman et al. 34 showed that 4.47% of patients who underwent coronary artery bypass surgery had had preoperative depression. One can assume that the proportion of patients with depressive symptoms might be high in patients with PC. Therefore, when scheduling the surgery, it is important to map and to identify those individuals who already have or may be at risk of developing anxiety, worries or depressive symptoms. For that purpose, the self-reported Montgomery–Åsberg Depression Rating Scale (MADRAS) or the State-Trait Anxiety Inventory (STAI) can be used. 35 Furthermore, it is important to offer good patient-centred care in perioperative settings 11 in order to see each individual as a unique person and to increase patients’ involvement in their care. This in its turn may reduce the patient’s suffering by giving some sense of control back to the patient during the perioperative period.1,2 One way to provide patient-centred care is to have PD with patients who are to undergo CRS and HIPEC.
In terms of pain and pain medication usage, there were no differences in this current study between the group who received PD and the group who did not. Both Kain et al. 14 and Lin and Wang 15 emphasized that preoperative anxiety or worries may influence the experience of pain, meaning that the greater the level of anxiety or worry the patient has, the more likely it is for him or her to experience postoperative pain. On the other hand, earlier studies7–9 demonstrate that working with a person-centred focus with PD10,13 and providing information 17 may have a positive impact on patients and their recovery. In our study there was a difference in the number of times pain was rated as NRS > 3 in the group who received a perioperative dialogue compared to the control group. We believe that pain levels after this kind of major abdominal surgery are not solely affected by PD, but information and correct levels of pain medication are also required, as Kain et al. 14 and Lin and Wang 15 hinted in their studies.
The length of hospital stay and the overall outcome including pain are influenced by several factors such as age, gender, comorbidities, the diagnosis and the surgery itself, and whether the patient has poor mental health or anxiety or worries before surgery. 36 Again, this means that PD alone could not have an impact on the length of hospital stay. Our study illustrated this, as there was no difference between the group who received a perioperative dialogue and control groups as regards to how long patients were hospitalized.
Methodological considerations
This study is unique, as it describes and compares two groups of patients with PC: one group who received perioperative dialogue with an operating room or a nurse anaesthetist, and one who did not, with regard to pain medication, psychopharmaceutical agents and length of hospital stay. Even if the value of PD cannot solely be studied by parameters such as pain medication consumption, consumption of psychopharmaceutical agents or length of hospital stay, this study was a first attempt to describe ‘reality’, with a retrospective audit. Such studies are lacking in the literature. The PD and its correlation with postoperative pain 14 and patient satisfaction12,13 have been studied before. This study engages the possibility of studying the PD with quantitative variables as mentioned above. However, the fact that the variables mentioned above cannot solely be affected by the PD should be taken into consideration.
Correct and complete documentation is required when a study is based on an audit. In this study, few variables were missing from the documentation, which indicates that it was performed according to clinical standards. However, to increase the study’s reliability, a prospective study with greater control over documentation is needed. The documentation in patients’ electronic medical and nursing records was created by nurses and physicians and not by the patients themselves. In pain assessment, patients are usually asked about the intensity of their pain measured by a validated instrument. These data are self-reported by patients and therefore considered as the patients’ own grading. To increase validity in future studies and to be able to give a more complete picture, prospective data including measures of pain and anxiety before and after surgery should be assessed, and questionnaires or in-depth interviews should be performed in order to measure anxiety or worries which influence postoperative pain.
The current study had a descriptive character indicating that the perioperative dialogue can be studied quantitatively. As this was the first study of patients with PC treated with HIPEC, several groups of patients with different tumour burdens, different diagnoses or operations, and different waiting times for surgery were included. This might explain why there were no differences between the group who received PD and the control group. However, in order to study the impact of perioperative dialogue on patients’ postoperative recovery, patients with different tumour burdens, operations and diagnoses, or waiting times for surgery may be included in other study designs such as randomized controlled trials (RCT) that may better serve that purpose. Using the RCT design would also enable the analysis of both study and control groups during the same time period. Patients with different tumour burdens, operations and diagnoses, or waiting times for surgery, may be affected differently psychologically and experience different levels of pain postoperatively. In this study tumour burden was the same for the two groups. Furthermore, future studies must involve the patient, who is an equal partner in the perioperative dialogue, and anxiety or worries should be measured using validated instruments.
Further studies should also be conducted by following the patients in each phase of the perioperative period, i.e. pre-, intra- and postoperatively.
Conclusion
The perioperative dialogue may be studied quantitatively, but it must involve the patient, who is an equal partner in the dialogue. The perioperative dialogue did not affect the usage of pain or psychopharmaceutical medications or the length of hospital stay. Structured, validated self-reporting measures such as the Montgomery–Åsberg Depression Rating Scale or the State-Trait Anxiety Inventory may be used systematically before and after surgery in order to build a more comprehensive picture and to evaluate the perioperative dialogue quantitatively.
Footnotes
Author contributions
Christine Leo Swenne was responsible for the study design. Christine Leo Swenne and Erebouni Arakelian were responsible for the analysis as well as drafting of the manuscript. Louise Hjelte, Emma Härdne and Carin Friberg were responsible for the data collection.
Acknowledgements
We would like to thank all participating patients for their permission to review their medical and nursing records, and we have ensured that all patient identifiers have been removed so the patients cannot be identified.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.