
Abstract
To suffer from a critical illness or injury requiring treatment in an Intensive Care Unit (ICU) is a traumatic experience that may affect patients and their relatives for a long time. This study aimed to explore intensive care survivors’ experiences of recovery after hospital discharge, from the patient perspective. A qualitative interview study with 12 interviews was conducted and analyzed using inductive content analysis. Four categories emerged from the data: Bodily changes, Emotional experiences, A prolonged struggle and Gratitude. The findings indicate that the life situation of intensive care survivors is changed, that recovery takes time and that the feeling of gratitude for having survived is strong.
Introduction
It is well known that people who have been critically ill often experience significant physical and psychological problems during the recovery phase. 1 Psychological distress such as anxiety, depression and posttraumatic stress disorder (PTSD)-related symptoms affects recovery and can persist for several months or years. Anxiety is a normal reaction and response to stress that emerges when a person feels danger, threat and fear, or if the environment does not feel safe. 2 Individuals undergoing a traumatic experience such as staying in an ICU, may develop PTSD-related symptoms. This has been seen to occur in 3–20% of former ICU patients. 3 An ICU stay may lead to memory loss due to a combination of factors such as critical illness, ICU environment, drugs and high temperature, 4 and some patients have described persisting memory loss, anxiety, sadness, loneliness, frustration and depression following ICU discharge. 5 Psychological problems and existential stress may also linger for a long time after discharge from hospital. 6 In a study where ICU survivors were interviewed it was revealed that they felt they had been brought back to life but at the same time they fought with anxiety about becoming critically ill again. 7 Some ICU patients went through an existential depression and described that some days they felt apathetic, and that hope and the meaning of life disappeared. Anxiety took over instead and they asked themselves why they existed and even if it would be better to be dead. 6
Physical symptoms such as fatigue, reduced muscle mass and muscle weakness are common after an ICU stay. 1 Physical wellbeing and physical exhaustion, such as fatigue and muscle weakness, are the core issues for ICU survivors during the initial period after discharge from the ICU. 8 Other symptoms encountered by ICU survivors are respiratory distress, difficulty climbing stairs and loss of appetite. 9 Together, this leads to an increased dependence on others. 8 Psychological problems such as anxiety, depression and PTSD-related symptoms have a major negative impact on the patient’s physical rehabilitation after discharge from hospital. Psychological problems entail that the patient not being able to be involved in their physical recovery 10 and more than 50% of ICU survivors experience a reduced quality of life. 1
Nurse-led intensive care aftercare services are important in terms of strengthening the patient’s recovery. 11 Several studies that highlight the importance of aftercare services have focused on the patient’s experience of the ICU stay.12–14 One aim with nurse-led intensive care aftercare services is to provide support for patients physically and psychologically and to identify those in an early stage of PTSD. 15 Another aim is to listen actively, allowing the patient to talk about what has happened, thereby helping the patient to recapture a new life experience. 16 Patients surviving a critical condition have a need for care and support throughout the recovery process and need a coherent explanation of what happened. 17 There are several dimensions of recovery: existential, social, physical, clinical and functional. Recovery means the restoration of health to the patient’s condition prior to the illness 18 and is an active process demanding the patient taking responsibility for his/her own process and having his/her own goal for recovery. 19 Rehabilitation is not the same as recovering. Rehabilitation focuses on the patient’s symptoms and problems, while recovery involves the development of a new meaning of life in a different perspective. Many patients describe that they do not reach the status they had before their critical illness. 19
Studies about ICU patients’ recovery after hospital discharge and how they feel are lacking. More empirical studies about the phenomenon of recovery would increase awareness of the factors that are important to consider in care in the ICU and how these would affect recovery.
Aim
The aim of this study was to explore intensive care survivors’ experiences of recovery after hospital discharge.
Method
Design
A generic qualitative, inductive approach was used in this explorative interview study.
Participants
Patients with an ICU length of stay of more than three days were invited to an ICU follow-up meeting to talk about their ICU stay and how they currently felt, two to six months after ICU discharge. The study was carried out at two different hospitals in the south of Sweden during three weeks in early spring 2016. Inclusion criteria were Swedish-speaking adults with intact communication skills, planning to attend the follow-up consultation. Twelve adults were asked to participate, of whom all accepted to take part in the study. Two of these were women and ten were men and the median age was 66 years (range 22–84). Amongst the 12 participants three had been diagnosed with sepsis, one with septic shock and ARDS (acute respiratory distress syndrome), one with pneumonia and sepsis, one with myocardial infarction, one cerebral hemorrhage, two had suffered from complications after major surgery, two had had a cardiac arrest and one had been severely injured in a traffic accident.
Data collection
Unstructured interviews with the following single open-ended question were used, allowing the informants to answer freely: ‘How have you experienced the time since you came home from the hospital?’ Follow-up questions were asked, if needed, based on the informant’s answer. The interviews lasted approximately 30 minutes, ranging from 18 minutes to 39 minutes. The interviews were digitally recorded and transcribed verbatim. One participant completed the interview with an email clarifying what had already been said by describing the experience in written text. Two of the interviews were held at a place chosen by the informant and ten of the interviews were carried out at the beginning of the follow-up session. Nine of the informants had brought a relative with them. The first two authors, MN and AS, performed the interviews separately.
Data analysis
Content analysis was used to search for similarities, differences and patterns in the described experiences and a conclusion was drawn from the collected material without a predetermined hypothesis.
20
The analysis was inspired by Burnard’s four-stage model.
21
Burnard was chosen because he offers a structured way of handling data, moreover we were familiar with this approach.
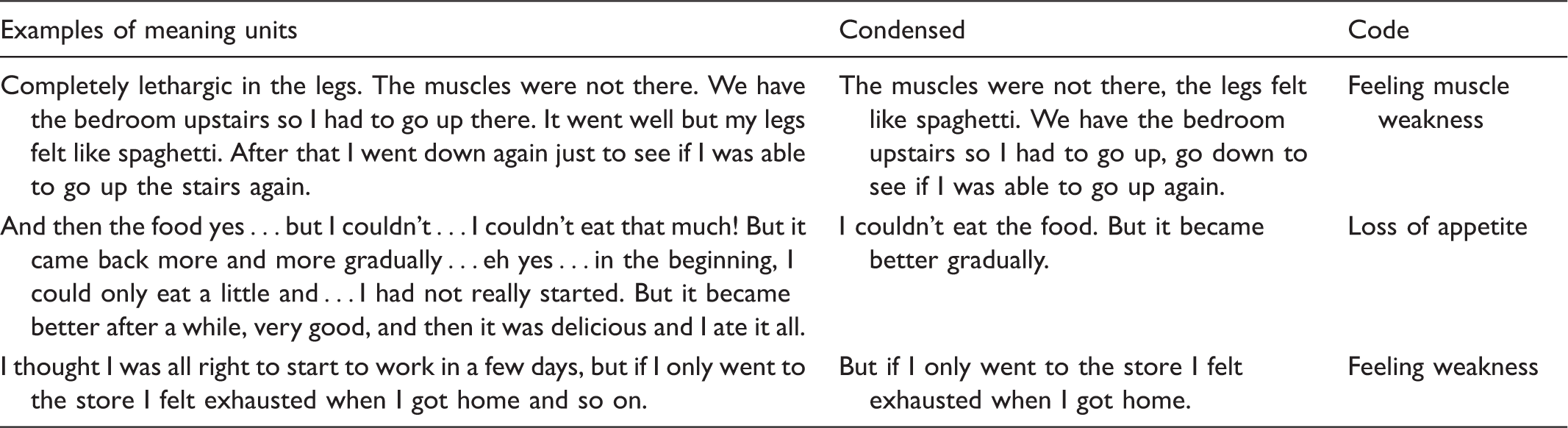
1a) In the first stage, the written text was read and meaning units were color-coded and a comment was added in the margin about the meaning units’ content. 1b) The authors identified meaning units separately for each interview and then similarities and differences were compared. The authors were, on the whole, consistent in the analysis. Differences were discussed and tested in relation to the aim of the study. If the meaning unit did not respond to the aim it was rejected. 2) The meaning units were condensed, which entailed them being shortened and redundant words being removed without losing the content of the material. 3a) The authors condensed and coded two interviews separately in order to ascertain whether they were consistent, and then compared their results. Condensing and coding of the ten remaining interviews were thereafter divided between the authors. 3b) The authors then merged the material and placed them in groups according to the codes. The authors took note of each other’s analyses and compared them. One common document was created in which the codes were pasted and similar codes were sorted together. Subcategory: the body’s limitation in daily life.
Ethical considerations
Ethical advice was obtained from the Board of Nursing Science Ethical Committee at Lund University and written approval was granted (VEN 4-16, 2016). The directors of the ICUs at the two hospitals approved the study and the participants were given verbal and written information and signed a letter of consent.
Findings
Four categories emerged from the data: Bodily changes, Emotional experiences, A prolonged struggle and Gratitude. Categories and their subcategories are presented in Figure 1.
Overview of categories and subcategories.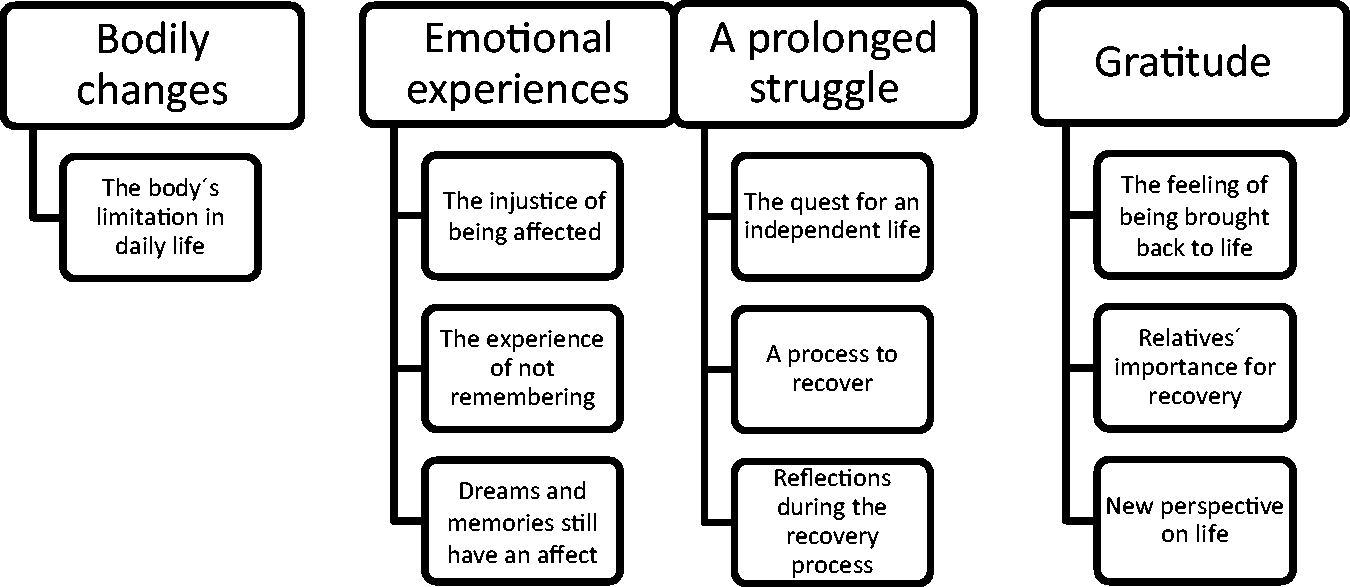
Bodily changes
Bodily changes were experienced after the ICU stay. It could feel as though the body had changed for the better or was essentially impaired, which limited daily life. Unintentional weight loss, loss of appetite and difficulties in sleeping were also described.
The body’s limitation in daily life
Bodily changes were experienced as a limitation and patients had become dependent on the help of others for managing daily life, which contributed to a feeling of helplessness. Not being able to fend for themselves and being dependent on people around them could be exemplified by not being able to pour coffee into a cup because of persistent tremors. Physical limitations led to a dependence on an aid because of impaired balance and impaired mobility and it took time before these functions were completely restored. I laughed when I was lifting up my grandchild in the swing. I could hardly lift her up! And that was no problem before … No, I said how heavy are you now? But of course, it was me who’d become weak. (5)
Emotional experiences
The ICU stay could lead to a changed frame of mind and patients felt more sensitive than previously. They spoke of being close to tears, of a fear of being locked in and an increased sensibility to loud noises. They also described an increasing fear that something unexpected would happen that would cause them to be admitted to the ICU again. Well, I’m now more afraid of something happening! I’m afraid of catching a cold. I’ve been so worried about infections and ending up there again [ICU] … But the thoughts are there in the back of my head, I hope I’m not getting ill again … And if I’m going somewhere to my family or something I check if they have stomach flu or influenza or something because if they have I won’t go to them, I don’t dare. Before I didn’t care. (6)
The injustice of being affected
Patients experienced suddenly suffering from an illness as unjust and sad. The injustice was difficult to cope with and they struggled with the question of why it should have happened to them and not somebody else. Sometimes I’m at home swearing … why should I encounter this misery … (5)
The experience of not remembering
The experience of not remembering was a very prominent feature. There were no first-hand experiences so knowledge was gained from relatives and by reading the patient’s diary and medical records. These described an acceptance and an understanding of having been brought back to life and that this process had demanded a great deal of their bodies. I’m thinking about what happened, but I can’t give myself an answer. That’s hard, I don’t know why I became ill and I want to know that. I came to the hospital … I don’t know anything! I still don’t know … the last thing I know is being in the ambulance. (6)
Dreams and memories still have an affect
The ICU stay affected some of the participants greatly. Unpleasant memories and dreams could, for example, still affect them. Unreal memories gave a strong experience of actually being real even if there was a logical explanation that they were too unreal to be true. It was described as a game in their heads. The experiences were so real that they were seeking references to confirm the theory several months later. The dreams about staying in the ICU were initially recurrent and could many times appear to be chaotic and about being close to death. … it’s my two German tanks from the second world war. My wife tells me that they’ve never existed, but I drove them down in the garage … I’ve had them. They stand in the garage. The memories are too precise to not be true. (12)
A prolonged struggle
Getting back on track after an ICU stay was described as being a long struggle. To be able to be at home at last and to continue daily life was a relief. Patients’ life situations had changed in different ways. This could entail them never being able to return to work and being dependent on daily care. At first it was nice to put my feet inside the door, take a deep breath … and you know … in some way it was important to come home to my daily habits again. But it’s been a little bit messy. A new bed, machines and so on are coming inside the house and then the home care is coming now and then and cables and stuff that need to be there. In one way you feel exposed. (12)
The quest for an independent life
Being dependent on home care and having to adjust their day depending on when home care was coming, could be experienced by participants as a feeling of being incarcerated. Home care could, on the other hand, also be experienced in a positive way, and they were relieved that the home care helped them with the daily procedure of dressing wounds as having to go to the health center every day felt impossible. Those who were positive towards home care saw the help as a relief. The desire to lead an independent life was evident when they did not want to be dependent on anybody. Yes, it’s freedom and so on that’s very important … And then my wife has to take a lot of work. The only thing I do at home is to take away the dishes from the breakfast … Sometimes when my wife has been away … she had time off from me, but she has to fight like hell you know. (8)
A process to recover
It took time to recover from the ICU stay and some participants experienced a gradual improvement, while others still struggled with slow-healing wounds and difficulties with mobility. They were motivated to exercise to restore their physical functions and progress in the exercises increased their motivation. Information provided by the physiotherapist helped them to feel more secure because they knew what to do to restore the lost functions. I took it step by step. I went to the store one day and did something else another day and then when I started working again I worked half time and so on. The food didn’t taste good in the beginning. Everything was strong. But now that’s not a problem anymore. I eat normally again. (9)
Reflections during the recovery process
Experiences of mental recovery varied among the informants. To be constantly bound to the healthcare services for regular examinations made them think about their future and whether they would be able to travel again. I love to cycle. I’d thought of cycling through the whole of Europe before, but now I can hardly dare to think about cycling. And when it comes to other diseases … that you get other diseases … it feels as if it was another life before the accident … and it’s a totally different life now … (10) What can you do for the rest of your life? What am I going to work with? Because everything I’ve done before I can’t do now. I have to work in an office … and I hate papers! It feels bad, yes it does. I can do anything else but handicraft … (3)
Gratitude
The participants were very grateful to the staff at the ICU and those in the home care services and to their relatives who had been there for them during their illness. They also expressed gratitude to life itself.
The feeling of being brought back to life
Participants said that they appreciated their life more now after nearly losing it. They considered themselves to be survivors and felt they could manage anything now. What I’ve gone through is hard. If the cat has nine lives I wonder how many lives I’ve got. I’ve had two difficult accidents as well, but I’ve always managed to come back every time. (12)
Relatives’ importance for recovery
The former ICU patients were very grateful to their relatives. They expressed that without their relatives they would not have been alive and that they still needed their help. One of them said that his wife was so important to him because they had gone through this difficult time together. It was not only the closest family members who meant a lot for recovery, but also friends, colleagues and neighbors.
New perspective on life
Having experiences of being critically ill led to participants seeing things differently and they had to make priorities about what was important in life. I worry less about everyday things such as economy and that it has to be nice in the house and garden. I don’t care. The main thing is to be alive. You get a different perspective. (10)
Discussion
Methodological considerations
Ten of the 12 participants in the study were men, which reflects the general picture of there being a majority of men admitted to ICUs in Sweden. A report from The Swedish Intensive Care Registry 2014 shows that 62% of those who met the criteria for follow-up after intensive care were male. Purposive sampling including more women could, however, have strengthened the study. The variation in age was satisfactory and the median age in current study was 66 years, which was close to the average age of 56 years at Swedish ICUs in 2014. 22
Most of the interviews were held as an initial part of the follow-up meeting, where both follow-up staff and relatives attended, which may have affected the findings. For example, the participant was sometimes interrupted by a relative who wanted to correct their stories to be more exact. Two of the interviews were held at a place chosen by the participant, where there was no time limit and no other person in the room. The informants were then able to speak more freely without anybody interrupting, which may have made it possible for them to talk about things they did not want to mention when their relative was present. If the interviews had been held in a more secluded environment they may have been longer and richer.
Content analysis was used with an inductive approach inspired by Burnard’s four-stage model. 21 The first two authors performed the analysis and read all the interviews and identified meaning units. All three authors discussed the analysis throughout the process in order to avoid losing essential parts, which can be said to increase credibility. The findings of the study are transferable because parts of the stories, for example concerning muscle weakness and the absence of memory have been shown in previous studies as symptoms that occur after an ICU stay. Despite every individual’s experience being unique, the findings of this study can, to some extent, be deemed to be transferable to similar settings and groups; i.e. to general ICU patients with an ICU length of stay of more than three days having similar conditions, treatment and care. Transferability is also strengthened by the variety of age, diagnosis and some variation of gender. 23
Discussion of the findings
The results showed that recovery after intensive care is an individual process. The individuals who recovered well, regaining their lives, saw life in a more positive way than those who were still struggling to recover. All the informants felt very grateful for having survived. They also addressed their gratitude to their relatives, the staff at the ICU and the home care services. These findings are in line with a current Nordic study which reveals that nursing staff and family members are very significant to the individual in the process of returning to everyday life. 24 The prolonged struggle back to daily life was initially difficult when the individuals did not have any energy at all and it could take a long time to regain their lost bodily functions. They experienced and went through similar processes although with some variations, and they coped with these differently. After the recovery process, they felt themselves to be more sensitive than previously and they experienced existential thoughts about why the illness had happened to them and not to somebody else. This is something that has been reported in nursing research as early as the 1970s and this type of reflection was the most common issue during recovery. 25 The feeling that somebody or something needed them made life worth living as people often need help to find meaning in different life experiences, not only to counteract resignation. 25 These emotional experiences are also described in a hermeneutic-phenomenological study on living with memories from intensive care, the result showing that the ICU stay leaves durable traces in patients’ lives for a long time, that they were dealing with who they are and that there is a quest for meaning. 26
The authors had a preconception that the ICU patients’ recovery process was long, which was confirmed in this study. The prolonged struggle back to daily life was a difficult experience manifesting itself in the complete lack of energy they experienced. Loss of muscle mass and ICU-acquired weakness is common following ICU which might explain the exhaustion experienced. 1 The physical impairments after the ICU stay were restricting their ability to live the life they had lived previously and led to a feeling of helplessness. This was due to participants being dependent on people around them, technical aids and home care services to manage their daily lives. Some thought it was difficult to be dependent, but others reasoned that life had changed and now they needed help to manage their situation. It also emerged that it took time to regain lost bodily functions, and for some of them their daily lives revolved around these and they experienced a fear of not regaining them at all. Being able to read the patient’s diary and the medical records from the ICU stay has been an important step in the recovery process as they lacked information about what had happened to them. A study that explored the meaning of patients’ lived experiences from the follow-up meetings confirms that patients seek meaning in their experiences and memories from the ICU stay and that until they come to the meeting the whole experience appears to be very unreal. 27
We thus maintain that follow-up is a significant part of the process, which is also confirmed in a study about recovery after ICU stay. 28 The aim for the Swedish nurse-led intensive care aftercare services was to facilitate the rehabilitation process by helping the individual with his/her experiences from the ICU stay, filling in memory gaps and giving information and advice. 28 Moreover, it is important that the ICU staff receive feedback, so that former patients can thank them for the lifesaving efforts they perform. Furthermore, the staff can receive knowledge about how the patients experienced being nursed at the ICU, which is significant from the perspective of improving care. A recent Swedish study shows that patients and relatives experience major differences between ICUs and ordinary hospital wards. The nurses on these latter wards need more support and knowledge to help individuals in reducing suffering related to experiences from the ICU. 29
Nurse-led intensive care aftercare services can help individuals through their illness and suffering. However, a study showed that follow-up meetings focused mostly on the experience of the critical illness and an understanding of the past rather than looking ahead. 28 An optimal follow-up requires an increased understanding of the whole recovery process and should not just consist of recalling occurrences from the ICU stay. As previously mentioned, some individuals from the current study were worried about the future and there is a risk of not identifying this if the ICU stay is the only focus of the discussion at the follow-up meetings. This means that there is a risk that the individual is not receiving the care they need. In a study about patients’ experiences from follow-up after ICU stays it emerged that former patients had positive experiences of the follow-up and that the follow-up was necessary in the recovery process. 14 They felt that the follow-up meeting helped to put pieces in place and to structure their experiences. By being able to discuss nightmares and hallucinations they gained a sense of what was real and what was unreal. The individuals who did not have a follow-up felt abandoned and disappointed. It was also shown that the former patients experienced that the hospital could not offer the aftercare that they needed. 14 Nurse-led intensive care aftercare services are thus important in terms of several aspects, for example, in a societal perspective when the aftercare can identify symptoms that need rehabilitation. If former patients receive the right support and help, the risk for long-term sick leave can be reduced. The participants experienced that the time after the ICU stay was as important as being brought back to life. Intensive care does not only entail saving someone’s life, it also entails helping someone to regain their life.
Conclusions
In conclusion, the study found that the life situation of ICU survivors changed and that the recovery process took time. The individuals described a similar recovery process, but the individual experience of it was unique. The participants experienced disparity between the ICU and the regular wards at the hospital and the lack of understanding created a feeling of frustration and abandonment. This study can contribute knowledge for ward staff that life may change following intensive care and that there is a difference between rehabilitation and recovery. It is imperative that healthcare staff better inform ICU survivors and their relatives that several symptoms and problems may occur during the rehabilitation period. Moreover, it is essential that patients and their relatives understand that recovering from critical illness or injury is an active and demanding process, which means that they must take responsibility for their own wellbeing and seek support when needed.
A suggestion for further research is to explore the experiences of former ICU patients during a longer period of time after ICU stay. This could provide a greater understanding of the whole recovery process, but also give an answer to whether the ICU stay only remains as a memory or will be an experience the patients carry with them for the rest of their lives.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.