
Abstract
Background
Physiotherapists play a crucial role in rehabilitating critically ill patients in intensive care units (ICU). However, variations are found in clinical practice amongst physiotherapists working in the ICU, both locally and internationally, due to the lack of minimum clinical standards and varying knowledge on critical care rehabilitation resulting in inconsistent quality of care.
Purpose
To establish a framework of the minimum standards of clinical practice for physiotherapists working in ICU in Singapore and compare the standards with existing literature.
Methods
A three-round modified Delphi questionnaire survey technique collated responses from ICU physiotherapists. The questionnaire contained 222 items, categorised into assessments, conditions and treatments. Responses to the items were either: “Yes, it is essential”, “No, it is not essential”, or “I am not sure”. Consensus for an item was reached when 70% of participants ranked it essential or non-essential. Participants comprised registered physiotherapists who have worked in the ICU for at least six months in the last 12 months and are currently working in the ICU.
Results
23 physiotherapists (median ICU-experience 7.0 (4.3–9.8) years) gave consent and completed the initial survey. 13 completed all three rounds of questionnaires. Overall, 163 items were regarded as essential, 21 as non-essential, and 38 did not reach consensus. The identified 163 items varied from similar studies due to different scopes of physiotherapy practice and professional autonomy.
Conclusion
This framework may guide the content of the physiotherapy education curriculum on critical care rehabilitation and minimise variability in clinical practice across different healthcare institutions in Singapore.
Keywords
Introduction
The advancement of intensive care medicine and multidisciplinary team management has improved the survival of critically ill patients. 1 Physiotherapists play a role in managing respiratory complications and preventing and treating consequences of prolonged immobility in intensive care units (ICU).2,3 However, as patients’ cardiorespiratory and haemodynamic status may rapidly change and require life-supporting equipment and pharmacological therapy, the role of physiotherapists becomes more complicated. 4 Hence, ICU physiotherapists need to be deft in understanding the complex medical issues and equipment in order to provide effective and safe rehabilitation for critically ill patients. 5
In Singapore, entry-level physiotherapists can begin working in ICU after a year of general rotations to the different disciplines. The on-call system of acute hospitals potentially dictates that physiotherapists who are not respiratory specialists practice in the ICU during their weekend shifts, despite being unfamiliar with the setting. To date, there is only one study that describes the vast profiles of patients who require after-hours physiotherapy services in Singapore. 6 In a separate study, the clinically important differences between the treatment provided by the non-respiratory and specialist respiratory physiotherapists illustrates the significance of training and proficiency of non-respiratory on-call physiotherapists, particularly in delivering physiotherapy treatments in the critical care environment. 7 Inferring from these ideas, it is therefore only sensible to establish the minimum standards of clinical practice relevant to the local critical care settings. Furthermore, there are currently no standardised local training guidelines to acquaint physiotherapists with this highly specialised domain. The lack of local consensuses, such as “Oncall Position Statement and Recommendation: Association of Chartered Physiotherapists in Respiratory Care” in the United Kingdom (UK), 8 further hinders benchmarking of local practice with global standards. The different individual in-house induction programmes for entry-level physiotherapists often vary in the content and duration of training. Senior physiotherapy staff usually define competency standards, often subjective and informal, with varying hospital requirements. Unsurprisingly, this results in a wide disparity of skillset and expertise levels among ICU physiotherapists. This difference in expertise level could translate into differing patient outcomes due to inconsistencies in the clinical decision-making process. 9 Experience-informed practice is common among ICU clinicians, thus resulting in variations in clinical practice on the choice of physiotherapy techniques and the interventions provided.10,11 This highlights the potentially detrimental influence on patient outcomes. 12
An international drive has emerged in Australia and New Zealand (AUS-NZ), 11 South Africa, 10 the UK 13 and Japan, 14 acknowledging the importance of standardising the expectations of clinical practice of ICU physiotherapists. Skinner et al. 11 (2016) utilised a modified Delphi technique to examine the minimum standards of skills and knowledge needed for physiotherapists working in Australia and New Zealand intensive care settings. The study recruited 50 highly experienced ICU physiotherapists, who completed three rounds of questionnaires each over a maximal 8 week period. This study concluded that 132 items out of 222 items (2 items were omitted from the original 224 items during the modified Delphi survey) were deemed essential and were included in the final framework. Twose et al. (2019) adopted a similar protocol but recruited a larger panel of 114 physiotherapists, and the study deemed 107 items essential for the minimum standards for ICU physiotherapists in the UK. More recently, Takahashi et al. (2020) further contributed to the Japanese minimum standards, with 188 items established as essential for the practice of physiotherapy in the ICU in Japan. 14 Noteworthily, the Japanese physiotherapists included more essential items than physiotherapists from western countries.11,13 A similar initiative in South Africa took place with van Aswegen et al. (2017) exploring the topic in South Africa ICU. 10 Unlike the studies mentioned earlier, these investigators used the nominal group technique as their approach to determine consensus, with their cohort of 25 experienced clinicians concluding that three main themes were necessary for the practice of physiotherapy in the ICU - integrated medical knowledge, physiotherapy practice components, and multidisciplinary teamwork.
These studies established the minimum standards of ICU physiotherapists in their respective countries. Such results could inform the practice standards of physiotherapy and corroborate the curriculum for entry-level physiotherapy programmes. However, there are anecdotal differences across countries, such as the varied role of ICU physiotherapists, the discrepancy in the scope of patient referrals, levels of professional autonomy, intervention preferences, and resources available. These determine the entry-level curriculum, length of training, and job demands,9,15 thus it may not be feasible to generalise and apply international results to Singapore’s context. Therefore, this study aimed to establish the minimum standards of clinical practice for physiotherapists working in ICU in Singapore. The results will formulate an initial framework to support curriculum development to cater to the training needs of physiotherapists at various career junctures. More importantly, this local initiative will enhance the consistency of clinical practice of the physiotherapists in the ICU in Singapore and enable international comparison.
Methods
Ethics
The University Institutional Review Board granted ethical approval (Project Number: 2020073) for this study. Potential participants received the project information via work email addresses of their affiliated hospitals. The return of the completed questionnaire assumed implied consent in each round of the modified Delphi survey. This study took place between March 2020 and January 2021.
Study design
Guided by the Recommendation for the Conducting and Reporting of Delphi Studies (CREDES), 16 this study adopted a modified Delphi survey technique to obtain the consensus.
Participants and sampling method
A purposive snowball recruitment strategy was employed to recruit participants for this study. Invitation emails were sent to professional networks and the physiotherapy departments of local acute hospitals with ICU to seek potential participants. A screening questionnaire that sought information such as consent to participate in the modified Delphi survey, years of clinical and ICU experience, and the current working ICU settings were sent to each potential participant individually. Additionally, we actively asked the potential participants for their referral of individuals who may be eligible to participate in the study by providing the referees' workplace email addresses. The screening questionnaire filtered their willingness to participate and the inclusion and exclusion criteria. The inclusion criteria for this study were: (1) physiotherapists fully registered with the Allied Health Professions Council, Singapore 17 ; (2) physiotherapists who are currently working in any Singapore adult ICU and have been for at least 6 months in the last 12 months. There was no pre-determined sample size, as there is no local census on the number of physiotherapists working in the ICU. Similarly, our inclusion criteria of 6 months minimum ICU experience was low compared to the 3 years required in the AUS-NZ or the UK reports.11,13 This mechanism in the inclusion criteria could potentially include rotating junior physiotherapists seriously considering future specialisation in critical care, as it is otherwise uncommon for uninterested therapists to stay beyond a typical 6-months rotation. Participants were excluded if they: (1) did not fulfil the inclusion criteria; (2) did not provide sufficient personal and contact information; and (3) wished to remain anonymous, as follow-up was essential for the modified Delphi survey design. Following the similar methodology of Skinner et al. (2016), we aimed to recruit a minimum of 30 participants for all three modified Delphi rounds. Mechanisms to invite additional participants to participate were in place to account for attrition throughout the three modified Delphi surveys.
Modified Delphi survey questionnaire
With permission from the original authors, the questionnaire used in this study was based on the final 222-item list developed by Skinner et al. (2016). 11 It defined the comprehensive role of physiotherapy in the ICU based on existing empirical resources, ICU competency checklists, and current entry-level academic materials from AUS-NZ. Minor modifications of language and medical terminology were made to ensure its relevance to the Singapore context, such as the inclusion of ETT as the abbreviation for endotracheal tube, and ETCO2 to represent end-tidal carbon dioxide. The questionnaire contained 222 items, categorised under assessment, condition and treatment. For each item, participants had three response options: “Yes, it is essential”, “No, it is not essential”, and “I am not sure”. An open comments section was available in rounds 1 and 2 for participants to submit any additional items that may be absent from the questionnaire. The questionnaire was piloted by three investigators who previously worked in the ICU but were not members of the Delphi panel before the full-scale modified Delphi survey began to assess the clarity of the questions and estimate time commitments to complete the questionnaire. The three investigators combined had approximately 35 years of local ICU and 50 years of local clinical experience. The final results did not contain any pilot data.
Data collection procedure
The questionnaire was posted on an online survey platform (QualtricsXM 2020, Provo, UT, USA) and disseminated through an email link. The modified Delphi survey consisted of three rounds of questionnaires, and participants were given a maximum of 5 weeks to complete each round. Due to the lengthy nature of the questionnaire, the “save” function enabled participants to store their responses intermittently if they experienced response fatigue. 18 Participants had the option to resume the survey when they were ready. Email reminders were sent to non-respondents on the second and fourth week during each cycle. A comparison of individual and group quantitative results was provided to each participant at the end of every cycle. The current modified Delphi survey did not include any focus group discussion.
Data analysis
Results from the questionnaires were exported from QualtricsXM and analysed on Microsoft Excel™. Consistent with the earlier studies11,13 and literature recommendation, 19 items were deemed essential or non-essential if they achieved >70% consensus for essential or non-essential accordingly. Any items that attained a >70% response as essential would have their status established and removed from the subsequent survey cycle. Additionally, items that attained >70% as non-essential were considered non-essential and excluded from subsequent rounds. Items that received less than 70% response rate for ‘Yes, it is essential’ or ‘No, it is not essential’ were brought forward to the subsequent round as they did not attain any consensus. Furthermore, items with “I am not sure” as their primary response were also brought to the next round
Results
Twenty-four physiotherapists who met the inclusion criteria consented to participate. Figure 1 depicts the process of panel selection and the response rate at each modified Delphi survey. 10 potential participants were excluded due to inadequate ICU experience or missing information. One recruited participant was never initiated in the modified Delphi survey, resulting in the initial sample size of 23 participants who completed the first round of the modified Delphi survey. 10 participants were lost in rounds 2 and 3 of the modified Delphi survey; 18 participants (78%) completed round 2, and 13 participants (57%) completed all three rounds. The investigators did not manage to recruit additional participants during rounds 2 and 3 of the survey. Panel selection and completion rates.
Comparison of variables between Singapore, AUS-NZ, the UK and Japan.

aRetention rate defined as the percentage of participants who remained until the end of the study. SD: standard deviation; IQR: interquartile range.
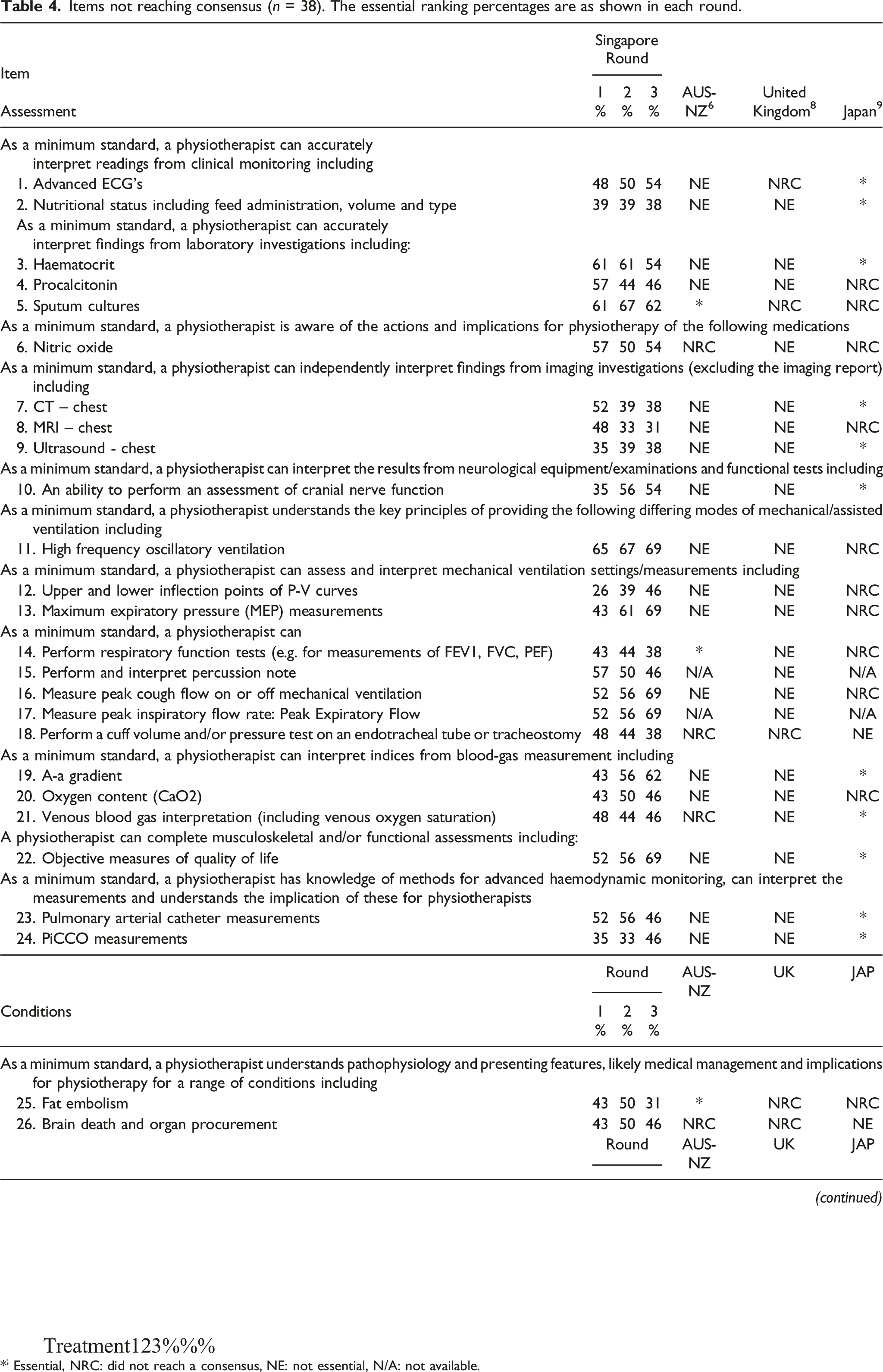
Figure 2 depicts the inclusion and exclusion numbers of the 222 items through the three rounds of the modified Delphi survey, and Table 2 elaborates on the modified Delphi survey results. Twenty-one items were deemed non-essential (Table 3), and no consensus was reached for 38 items (Table 4). The participants suggested no new items via the open comment option throughout the modified Delphi process. Flow of items through the modified Delphi rounds. Items determined as essential, where consensus is defined as >70% of participants agreed. The percentages are as shown in each round. (n = 163). *; Essential, NRC: did not reach a consensus, NE: not essential, N/A: not available. Items determined as non-essential, with consensus defined as >70% Non-Essential (n = 21). The non-essential ranking percentages are as shown in each round. Items not reaching consensus (n = 38). The essential ranking percentages are as shown in each round. *; Essential, NRC: did not reach a consensus, NE: not essential, N/A: not available.


Discussion
This report established the minimum standards of clinical practice for physiotherapy to ensure safe and independent practice in Singapore ICU. The overall consensus was reached on 163 items across the categories of knowledge and skill to conduct a holistic assessment on an ICU patient, knowledge of medical conditions to enhance clinical reasoning, and knowledge of physiotherapy treatment. The 163 items identified as essential to the minimum competency standards of clinical practice of ICU physiotherapists in Singapore are substantially higher than the AUS-NZ and UK studies, which deemed only 132 and 107 items essential, respectively, but similar to the Japanese results (Table 1 161items). It is difficult to pinpoint a reason for this based on this study alone, but one possible reason could be the wide variety of conditions, such as the general medical, surgical, neuro-surgical, and cardiothoracic cases that a typical ICU physiotherapist would have to cover routinely in Singapore. This results from the population-dense city-state with major general hospitals and specialised centres located within proximity to provide highly integrated healthcare. Each specialty requires a relatively distinct set of knowledge and skills, translating into more items being deemed essential in this study. For example, items considered essential in our study and the Japanese report, but not in AUS-NZ or the UK, included many cardiovascular and neurosurgical items such as having an understanding of the extra-ventricular drain (EVD), actions and implications of pharmacological agents and delirium assessments (Table 2, item 16, 36–43, 50). The ICU physiotherapists in Singapore unanimously agreed that knowledge of EVD is essential as post-neurosurgery patients are common across most ICU in Singapore. This was also deemed essential in Japan (91%) but did not meet the essential status in AUS-NZ and the UK. Similarly, knowledge of actions and implications of pharmacological agents and delirium assessment were deemed highly essential. This could be due to the prominent role of ICU physiotherapists in Singapore in facilitating early mobilisation in critically ill patients, proven for its effectiveness to prevent the onset or reduce the severity of ICU-acquired weakness.20–24
Furthermore, Takahashi and colleagues (2020) suggested that identifying more items could be the result of the rapid development of the advancing role of physiotherapists in the Japanese ICU, leading physiotherapists to realise the need for a broader range of knowledge and skills to practise in the multidisciplinary patient-centred care ICU setting. 12 While this does not imply that physiotherapists in AUS-NZ or the UK do not have the same level of knowledge, rather it highlights the difference in perception of what physiotherapists feel is important in their ICU culture. This further emphasises the need for minimum standards that are unique to the local healthcare practice.
Airway secretion clearance management forms another significant role of ICU physiotherapists in Singapore. Hence, it is not surprising that knowledge of manual airway clearance techniques, manual hyperinflation via an endotracheal tube or tracheostomy, and airway suctioning (Table 2, item 131, 138–141) were deemed essential. This finding is similar to our AUS-NZ and UK counterparts. Notably, Japanese physiotherapists are not permitted to perform these interventions and thus resulted in the non-essential status of these items. This variation, therefore, reflects differences in physiotherapist roles and professional autonomy guided by local regulations.
Singaporean physiotherapists did not consider the interpretation knowledge for nutritional status or imaging investigation, particularly for CT and MRI scans (Table 3, item 3–6; Table 4, item 2, 7–9) as essential, which were items that were established essential only in the Japanese study. 14 One possible reason is that dietitians are a well-defined part of the intensive care team in Singapore, AUS-NZ, and the UK. Dietitians in the ICU team are prominent with a strong interest in nutrition management in intensive care medicine in our local settings. 25 This claim is evident from the subsequent representation in establishing the consensus on nutritional therapy for the critically ill. 26 In the same way, while chest radiograph and skeletal X-ray (Table 2, items 44 and 45) were deemed essential, diagnostic radiologists and the timely availability of imaging reports form the cornerstone of intensive care in Singapore, hence CT and MRI interpretations were considered non-essential by the participants.
The role of ICU physiotherapy differs significantly from other disciplines of physiotherapy. Physiotherapists play a crucial and growing role in the multidisciplinary team approach to patient management and rehabilitation in ICU.2,3,5,20,27 The emerging emphasis on improving health-related quality of life and functional outcomes of survivors of critical illness prompts effective physiotherapy treatment to boost patient outcomes in ICU. 28 In such a complex setting like the ICU, this propels health care professionals to describe the minimum standards in clinical practice in order to provide optimal care for patients during their ICU stay. The specific focus on cardiorespiratory health, the acute precarious nature of the patient’s condition, and the higher likelihood of significant adverse events as a result of inadequate clinical decision-making and intervention all warrant physiotherapists to be equipped with sound knowledge and high proficiency in clinical decision-making skills.9,10 It is, therefore, essential to establish minimum standards of competency required to ensure a safe and effective clinical practice. As evident in the results of this study, physiotherapy practice in ICU may vary across countries due to specific local regulations, variance in scope of patient referrals, and disparity in professional autonomy. Hence, it is essential to establish the minimum standards of clinical practice for physiotherapists specific to the local context.
Establishing such minimum standards of competency would aid the formulation of a standardised training framework for physiotherapists to function proficiently in the intensive care setting. This could reduce the variability in the quality of treatment, hence improving patient health outcomes. 29 In addition, the role of the ICU physiotherapist is currently not clearly defined in Singapore and may overlap with the job scope of other healthcare professionals, such as respiratory therapists. This similar struggle is shared with our AUS-NZ counterparts. 27 Hence, developing a framework would strengthen the definition and integration of physiotherapists in the intensive care setting. 11 Skinner et al. 11 (2016) posited that such a framework can enhance the credibility of ICU physiotherapists and the physiotherapy profession as a whole.
Furthermore, such minimum clinical competency standards may inform the planning, design, and implementation of the local entry-level physiotherapy curriculum. Of the surveyed 222 items, 182 items are taught in the local physiotherapy programme, including the 163 items deemed essential by the respondents of this study. This finding reassures that the current curriculum is congruent with national standards. Moreover, as local curriculum has recently eased into an entrustable professional activities (EPA) model, 30 the essential items identified in this study can be used as a basis for EPA assessment in physiotherapy ICU trainees.
Some limitations in this study should be considered. Participants in this study possessed fewer years of clinical and ICU experience compared to other studies (Table 1). The average age of the physiotherapists in Singapore is predominantly younger than our counterparts, evident by Singapore’s Allied Health Professions Council 31 Annual Report 2019 that up to 75.6% of physiotherapists in Singapore are 39 years old and younger. This would inevitably influence the average ICU experience and could also account for the larger number of items deemed essential. As one can postulate, the mastery of knowledge and skills can compensate for the shortfall of experience. Additionally, several physiotherapists working in ICU at the time of the study were mainly junior rotating physiotherapists who only commenced their ICU rotation with less than 6 months of ICU experience. Hence, they failed to meet the inclusion criteria despite being identified as potential participants. The sample size and retention rate in this study were also low compared to the Japan, AUS-NZ, and UK studies. This is likely due to the fact that as a small city-state, Singapore has fewer ICU and hospitals. Consequently, the initial 23 participants recruited in this study represented 12 of the 15 local hospitals with ICU, and may be viewed as the leading authority representing the key opinions relevant to the practice of ICU physiotherapy in Singapore, who are qualified to deliver valid and relevant viewpoints regarding critical care rehabilitation. Although the absolute attrition number (n = 10) was significantly lower than in other studies, which ranged from 16 to 50 participants,9,11 only 13 out of the initial 23 participants completed all survey cycles eventually, translating to a low retention rate (57%) in our study. The survey length might have resulted in fatigue, causing the high attrition. Most importantly, the study was conducted during the peak COVID-19 pandemic in Singapore when there was a sudden surge in survey studies. This might further explain the low retention of the participants, in addition to the strained manpower situation among frontline healthcare workers, especially those in the critical care settings.
Nevertheless, the information gleaned from this study appears valid and relevant to our local context, as previously discussed. This serves as an important basis for how local physiotherapy training should be modelled to prepare therapists for managing patients in this complex and highly specialised setting.
Conclusion
This study identified 163 items of knowledge and skills essential as a minimum standard for clinical practice for ICU physiotherapists in Singapore. The challenge now is to integrate this newly established framework into clinical teaching, position statements and performance management so as to reduce variability in clinical practice.
Supplemental Material
Supplemental Material - Minimum standards of clinical practice for physiotherapists working in adult intensive care units in Singapore
Supplemental Material for Minimum standards of clinical practice for physiotherapists working in adult intensive care units in Singapore by Bernice X Lee, Joyce C Tiew, Jovan G Lim, Diana Sani, Clement C Yan, Shane Patman, Melissa Y Chan and Meredith T Yeung in Proceedings of Singapore Healthcare
Footnotes
Acknowledgement
We would like to thank all the participants and the Health and Social Sciences Cluster of the Singapore Institute of Technology for supporting this research.
Author contributions
BXL was involved in drafting the manuscript, participant recruitment, data collection and data analysis.
JCT and JGL were involved in participant recruitment, data collection and analysis.
DS, CCY, SP and MYC contributed to the conception of the project, reviewed and edited the manuscript.
MTY contributed to the conception of the project, reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Singapore Institute of Technology.
Ethical approval
(include full name of committee approving the research and if available mention reference number of that approval) Ethical approval for this study was obtained from the Singapore Institute of Technology Institutional Review Board (Approval number 2020073).
Informed consent
Consent is Implied when Participants Return the Completed Delphi Survey
Availability of data
The data sets generated and/or analysed during the current study are available from BXL and MTY upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.