
Abstract
The purpose of this study was to explore factors in the municipal workplace environment that can facilitate experienced nurses in promoting their professional competence. This is of particular importance when critically ill patients are discharged from hospital. We interviewed nine nurses who had more than five years’ experience in the Norwegian municipal healthcare services and analysed data using qualitative content analysis. We found that the informants have to cope with situations for which they have not been adequately prepared. Two factors in their workplace environment influenced the promotion of their professional competence in such situations: access to knowledge and information, and supportive collegial relationships. Experienced nurses are an important resource for information and support. However, the findings also suggest that nurses at all levels of competence are dependent on working environments that promote a high standard of nursing.
Introduction
Nursing environments are constantly changing as a result of the introduction of new technology, economic and political reforms and developments in public health. The move towards primary care as a model of healthcare and service provision has necessitated changes in nursing environments, roles and responsibilities. In a literature review, Barrett and colleagues highlighted the extremely complex role of nurses in community nursing. 1 Community nurses work with a range of patients and service users in very diverse settings, which requires a high level of flexibility and diversity of knowledge and skills. The implementation of the Norwegian Coordination Reform 2 has necessitated that nurses working in municipal healthcare services in Norway have to deal with new and advanced procedures and treatments for patient groups that would previously have been treated in hospital.2,3 Most of these nurses have not had the opportunity to develop their competence in accordance with the increasing demands for specialised nursing skills. 4 In both nursing homes and home care services, nurses often work alone or with a limited number of colleagues and with no formal setting to discuss nursing problems.5–9 Some Swedish studies have highlighted that nurses feel undervalued and frustrated when expected to ‘be everywhere and know everything’,10(p.265) as they are expected to provide specialised care without specialist training. 11 In Norway, well-qualified clinicians are essential to meet patients’ complex care needs. 5 Nursing education alone is not enough; it has to be seen within the context of nurses’ working conditions and collaboration routines with colleagues and leaders. 8 Work conditions such as understaffing, time issues and increased pressure on nursing-home staff all contribute to insufficient care. 12 Nurses seem to find different strategies such as working overtime or dropping breaks to bridge the gap between their professional ideals and their working reality. 13
The workplace environment can be described as the tone of the workplace, influenced by different factors, such as access to necessary resources, good communication with team members, knowledgeable and supportive managers, input into workplace decisions, and a reasonable workload.14–17 Factors that home-care nurses value as being supportive of professional nursing practice are strikingly similar to those valued by hospital-based nurses. 16
A supportive workplace environment is highlighted in a number of studies worldwide as an important factor for nurses’ satisfaction, retention and continuity of employment,13,14,18,19 and for nurses’ confidence in decision-making processes. 20 Several of the studies emphasise the importance of a supportive workplace environment for the nursing role, but focus less on the specific factors of importance in providing nursing care in line with the level of competence of the most experienced nurses.
The purpose of this study was to explore experienced community nurses’ perceptions of workplace factors that can influence professional care delivery in line with their competence. Benner’s theory and insight into experienced nurses’ competence provides an important point of reference for this study.21–23 One of her implications for nursing administration and practice is that times of increasing cost and efficiency with fewer nurses make it more necessary than ever to keep and develop the competence of the most proficient nurses. 23 Experienced nurses can have the necessary skills, commitment and ability to persevere with their work, which makes them an important resource for their environment.21,23 The involvement of experienced nurses can ensure that a clinical situation is viewed from various perspectives and can reduce the likelihood of hasty decision-making. 23
Nursing competence is context and time specific. 24 Benner described five categories of nursing competence: novice, advanced beginner, competent, proficient, and expert nurse. 21 She claimed that clinical knowledge is gained over time, but that this progression does not refer to the mere passage of time or longevity. The individual nurse’s background, experience and knowledge will affect the level of skills, 22 and competence building requires a supportive work environment that promotes sharing knowledge and learning from experience. Nursing is more than a predetermined set of procedures and techniques; it is a complex socially organised activity under constant development that requires situational understanding and clinical reasoning acquired and developed over time. 23
Research methods
Presentation of the participating nurses.
Based on available literature on nurses’ experiences of their workplace environment and nursing competence, a semi-structured interview guide was prepared. In addition to covering the main themes, the participants provided supplementary information. The researchers also had the opportunity to pose follow-up questions and ask for clarifications. The interviews lasted between 50 and 90 minutes and were audio-recorded and transcribed verbatim. The interviews were carried out in 2012 by the first author.
Data analysis
Examples of meaning units, sub-categories and categories emerging from the analysis.
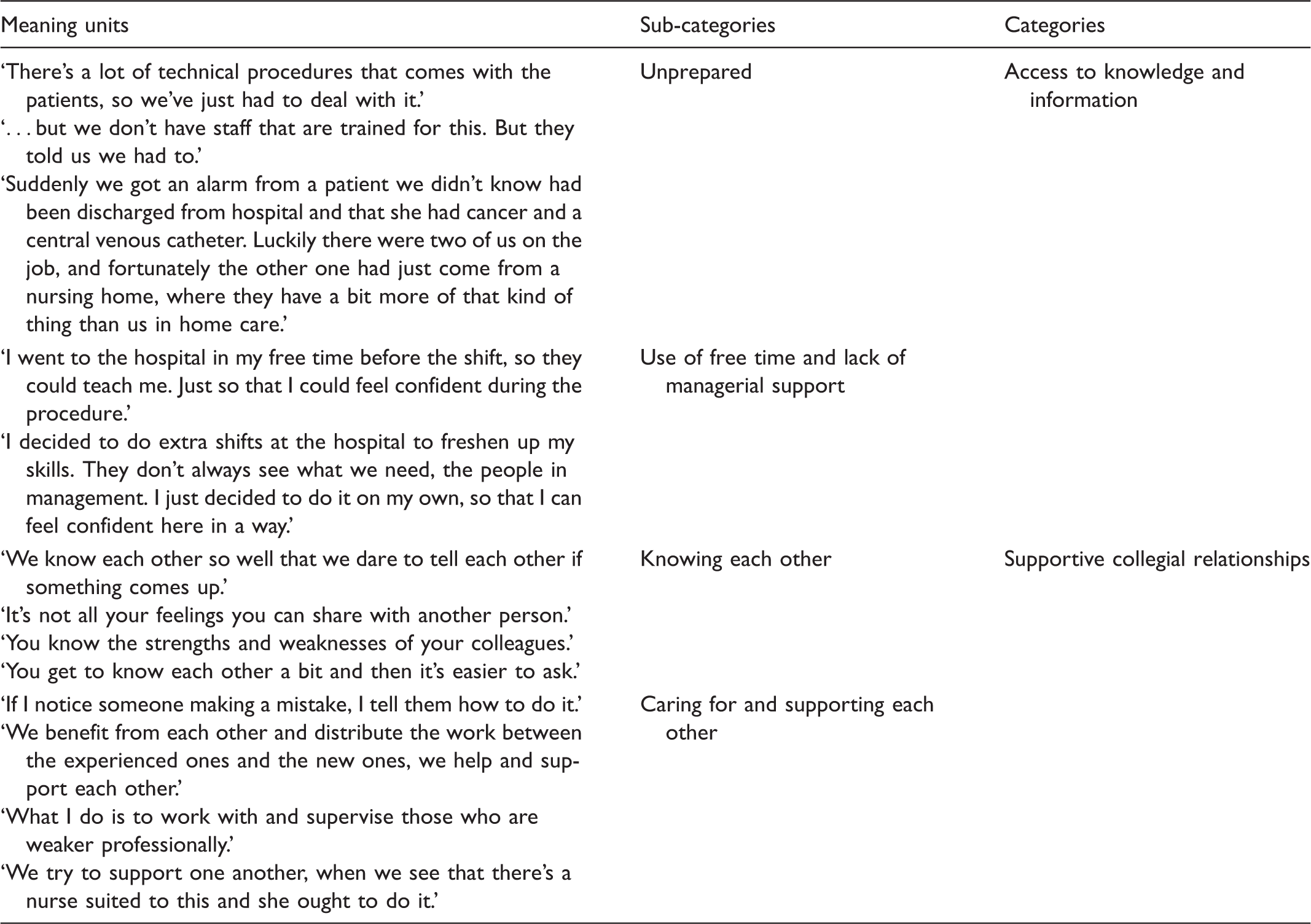
All authors read the transcribed data separately. The first and third authors carried out the main analysis. The second author contributed to the preliminary analysis and to the final stages where all authors reached consensus through discussion.
Ethical considerations
The Norwegian privacy protection commission for research, the Norwegian Social Science Data Services (NSD) reviewed and approved the study. Participation was voluntary and the informants could withdraw from the study at any time. All audio-recordings were deleted after transcription.
Findings
The findings reveal that the nurses lacked adequate information and training in order to meet the challenges they faced in their everyday work. They also spoke about the importance of having supportive relationships with their colleagues. Supportive relationships involved the following qualities: confidentiality, attentiveness and the availability of collegial support in difficult situations. In the following, findings and the content of each category will be described and examples given to illustrate the nurses’ statements.
Access to knowledge and information
All the nurses in the study spoke about patients coming from hospital to their workplace with different treatment regimens to be followed up by the nurses. Several indicated that they needed access to more information on the patient’s condition and further treatment and care, as well as knowledge of how to use any advanced technology that accompanied the patient.
Unprepared
Our informants reported feeling inadequately prepared or completely unprepared for many tasks they are expected to master in their everyday professional practice in both home nursing and in nursing homes. This may involve unfamiliar technological procedures or a lack of information about the patient’s return home and the further treatment regimen. In addition, tasks may arise regardless of the nurse’s available time and opportunity to prepare, as stated by the following informants: Patients may come at weekends (from hospital) at any time of day or night […] it’s awful when they arrive in the evening at shift handover, in the middle of the evening meal and we know little about the patient and we aren’t so many as on the day shift. (SNH1) … It varies how much information comes with the patient [from hospital]. We often find that many of them come without a discharge summary, when it’s not ready, so we have to ring and ask and never get it. This is the patient’s home, but the discharge summary is sent to the doctor and the patient himself, so we’re the odd one out. It may take a week before it comes […] We wonder what’s been done and what we’re supposed to look out for. How is the patient better and what medications have changed? Has the prescription been sent? If it’s at a weekend, we may not be able to get hold of medicine. (SNH3) Suddenly we got an alarm call from a patient that we didn’t know had been discharged from hospital and that she had cancer and a central venous catheter. Luckily there were two of us on the job, and fortunately the other one had just come from a nursing home, where they have a bit more of that kind of thing than us in home care. (HB1) We see more severely ill people and have bigger challenges and, of course, we also notice that they’re being discharged much earlier and there’s a lot of technical procedures that come with the patients, so we’ve just had to deal with it. (SNH4) It’s also happened that we’ve been given patients where they [the hospital] have assumed that we should offer intravenous treatment and Pari inhalations [nebulisers], but we don’t have staff that are trained for this. But they told us we had to. (NH1) We changed the venous cannula. Of course we did, but not all of us have enough confidence to do it. I don’t feel like an expert either, but we hung up the infusion and it worked […] We have the equipment, but we need someone to teach us, so the patients and the relatives can feel safe. (NH1)
Use of free time and lack of managerial support
Our informants expressed a need to feel confident in their nursing practice, which entailed having adequate knowledge and information. Their statements suggest that they felt a sense of responsibility for safeguarding patient care. We usually demand that they [the hospital] teach us. We can’t just accept it, can we, if suddenly the patient’s there? At least for my own sake, I need to feel safe when he comes [home]. (SNH4) We can’t take over a patient if we don’t know what to do. We just have to learn the different things, like various types of aids [...] Then you have to go to the hospital and get training before the patient arrives. (HB2) One of us worked overtime and the other one arrived early so that we could carry out the procedure with the central venous catheter together. So that’s how things work. (SNH4) It’s happened that I’ve rung a nurse on the other side [other department] and asked her in her spare time, ‘What do we do here?’. So it happens that you get a call when you’re off when you know the patient better than the others. (SNH2) I was on the weekend shift and the patient was due to come home on the Friday. So then I went to the hospital in my free time before the shift so that they could teach me. Just so that I could feel confident during the procedure. (SNH4) I decided to do extra shifts at the hospital to freshen up my skills. They don’t always see what we need, the people in management. I just decided to do it on my own, so that I can feel confident here in a way. (NH1) We try to get information from the police about drugs ‘what’s going around’ and ‘how does it work’. New drugs are constantly appearing and we learn about them through the media, the Internet and newspapers. (HB3)
Supportive collegial relationships
The informants’ statements indicated that nurses worked actively to improve both their own and their colleagues’ level of competence. They supported each other in their efforts to provide safe professional treatment for the patients. When they distributed tasks, they tried to take into consideration their colleagues’ skills and expertise and compare them with the individual patient’s condition, and to consider whether a particular care provider is capable of carrying out a specific task. In order to do this, they needed to know each other well, both professionally and as individuals.
Knowing each other
Knowing each other well lowered the threshold and made it easier to discuss uncertainties of a professional or ethical nature. As NH2 said: We know each other so well that we dare to tell each other if something comes up, and we can call each other privately. It’s perfectly all right to call each other and say, I wonder, you know in that room, what was the outcome? It’s so nice that we’re such a tightly knit group. It’s perfectly acceptable to call each other and when you finish the day shift say: ‘If anything’s unclear, just call me’. (NH2) Sometimes the air needs to be cleared and you can’t always discuss these things with everybody: there are some feelings you can’t share with just anyone. (SNH1)
Caring for and supporting each other
The nurses were conscious of the importance of peer support and of asking each other how they were managing and relieving each other if necessary. As SNH1 said: We always find someone to talk to […] and then we help each other and try to share the workload. Experienced nurses as well as novices help and support one another. (SNH1) If I notice someone making a mistake, I tell them how to do it. I’ve done this, and made mistakes myself, so it has nothing to do with being perfect, so feel free to let me know as well. (NH1) You know very well which patients you can pair with which staff and you know the strengths and weaknesses of your colleagues. You also know who’s professionally capable, and who isn’t. What I do is, I work with and supervise those who are professionally weaker by making reports or discussing how different situations panned out and then reminding them that you need to perhaps be more attentive. (HB2) My colleagues are the ones I absorb most knowledge from and make me reflect on things. (HB3)
Discussion
Our findings suggest three workplace factors that can influence professional nursing care delivery: Access to knowledge and information, managerial and systemic support and a supportive work environment.
Access to knowledge and information
Our findings, like those of Benner, 22 show that long experience in itself is insufficient to practice nursing at the highest levels (proficient or expert). For example, the patients and nursing tasks transferred from hospitals to local health services may be unknown and unfamiliar for our informants, who have little or no experience with advanced medical treatment. In this way, their familiarity with everyday work is affected in that the ‘flow’ of their work can easily be disturbed or undermined. According to Benner et al., 23 unforeseen tasks and changes in a patient’s condition will require experiential knowledge for the nurse to be able to detect qualitative differences and make the necessary professional judgements. This knowledge appears to be insufficient when our informants lack training in the use of technological equipment or information about a patient’s treatment regimen after discharge from hospital.
Limited information on patient treatment after discharge seems to be a familiar phenomenon in many parts of Norway.26–28 The nurses in our study reported that they themselves had to seek the information they needed in patient care as this did not always accompany the patient. This seems to be unfortunate in several respects. Firstly, information flow outside an electronic patient record system will increase the risk of leaking sensitive patient information and thus violate confidentiality. 26 It can be conducive to malpractice if nurses rely solely on information received from patients and caregivers, as these facts could be wrong or misunderstood. 29
The nurses in this study reported feelings of discomfort when they were not adequately prepared to meet the needs of their patients. This is in line with Flöjt and colleagues, 30 who have shown that community nurses need both theoretical and practical preparation in order to feel that they master their role. Nurses’ access to important information and specialised training to carry out advanced procedures will influence patient safety and the quality of care. It is suggested that there is an association between readmissions to hospital and patients being discharged before proper municipal nursing care systems are in place. 31
The findings in our study can indicate a lack of systems, which could have had serious consequences for the patients had the nurses not taken responsibility and retrieved the necessary information or acquired the necessary competence. The nurses in the study described being inadequately equipped to deal with these situations. We can only speculate how less experienced nurses would cope. According to Benner,22,23 less experienced nurses are dependent on more experienced colleagues. Experienced nurses who lack expertise in certain situations will often know how to access both information and support.
According to Kihlgren et al., 20 experienced nurses in municipal healthcare are presumed to be able to make the right decisions when a patient suffers acute illness or needs hospitalisation. Kihlgren et al. 20 claim that in order to have faith in their competence and professional role, nurses need sufficient knowledge about patients and a supportive environment. This can be a major challenge to nurses working in municipal healthcare, where they are influenced by organisations that create a power imbalance, 28 discrepancies in competence 8 and increased pressure. 32 Our findings show that the nurses felt pressurised to carry out procedures for which they lack competence, despite having reported this to their supervisors. This can indicate a lack of support from a managerial level.
Managerial and systemic support
Managerial and systemic support can influence work satisfaction and the will to continue working.14,16 The nurses in this study spoke of lacking competence in using advanced technological equipment, which is in line with similar studies. 5 Increased time off for training may be a necessary factor to avoid an unfortunate refocusing of work priorities. For example, a Swiss study 19 showed that limited time for nursing practice implicitly affected nurses’ prioritisation of work tasks, such as a lower focus on the social aspects of patient care.
In our study, we find that experienced nurses wish to act according to their professional standards and take on the responsibility of finding the correct solutions, in line with Benner et al. 23 In their everyday practice, they attempt to find and share knowledge with colleagues, which is a traditional way to acquire knowledge and solve problems.6,9 A necessary precondition is that colleagues are accessible and have the relevant knowledge. The question remains as to whether this is a possible solution for community nurses. From other surveys, we know that in home-based services nurses often work alone 33 and see themselves as ‘lonely fixers’,10(p.265) working with colleagues with limited qualifications.8,10
The findings in this study reveal that relying on colleagues is not always enough to ensure safe practice. Nurses’ colleagues could also have insufficient knowledge, so nurses would have to seek information and necessary training outside their workplace, e.g. by taking on extra work in the hospital or taking courses in their spare time. According to Debesay et al., 34 it is the responsibility of the public authorities to provide adequate learning facilities. The nurses in the present study seem to take responsibility themselves in order to compensate for inadequate systems. Doing a lot of voluntary extra work without getting paid may over time be exhausting for nurses, or, according to Tourangeau, 18 make nurses less inclined to continue their careers as nurses. When nurses in home care try to live up to the profession’s high ethical standards by working overtime and cutting down on breaks, sick leave or working part time may be a solution to reduce the physical and moral stress of working in such a demanding environment. 13
A supportive work environment
According to Bedin et al., 35 nurses are the linchpin that binds functionality and community in nursing homes. A hallmark of nursing as a profession is that it is a coherent, socially organised activity.22,36 It requires a supportive work environment that promotes sharing knowledge and learning from experience in order to develop nursing skills. 23
Collegial support seems to be determined by nurses’ mutual trust and solidarity. Our findings suggest that the greater the trust and familiarity between staff, the easier it is to make contact and discuss professional or personal matters. Through the care they show for each other, they make themselves available to their colleagues in their spare time, answer questions, give advice and listen to their emotional troubles. This can be interpreted as a way of including each other in a secure and trustful working community that makes them unafraid to ask questions.
According to Benner et al., 23 inclusion is particularly important for less experienced nurses, as they are particularly vulnerable to the stress they face when their duties exceed their competence. These nurses need most of all psychological support and space to discuss the various everyday issues they face, according to Benner. Our findings indicate that this is also important for nurses with considerable experience. Even though our informants have many years of experience at their workplace, the responsibility they face may nevertheless be too much for their experience and knowledge. Psychological support and opportunities for discussion therefore seem to be necessary for all nurses, regardless of their level of expertise.
This can be compared to work environment traits, which Flynn calls processes; 16 these are interpersonal activities or interventions related to care delivery. In her study, she found that home-care nurses rate the presence of supportive supervisory staff as the one agency trait they considered most important to them and their practice. Carlson and colleagues 37 found in their study that home-care nurses need to be able to balance independence with the loneliness that the job entails, which requires many years of experience in addition to cooperation. The authors go so far as to say that the relationship between staff is just as important as the relationship built with patients, as a respectful collegial relationship has a positive influence on work satisfaction and the desire to stay in the job.
Our findings suggest that good collegial solidarity enables experienced nurses to strengthen and maintain both their own individual expertise and collegial expertise. The informants stated that they supervise closely and even intervene with their knowledge to ensure that work is done correctly. At the same time, they show each other care and respect, revealing their own shortcomings and fallibility. In this way, they seem to create a positive climate of confidence and possibilities rather than helplessness in the face of any serious and critical situations that may arise.
This seems to be in line with Benner et al., 23 when they point out the importance of developing collaborative and affirmative teamwork with clear communication channels that communicate and develop the cumulative knowledge acquired. To make this possible, it seems necessary to provide nurses with suitable facilities to support them. Such facilities are mentioned by Rosness, 38 who writes about organisations which aim to ensure that work is performed as intended. He argues that this requires the availability of experienced employers and an opportunity to observe, to listen to justifications and also to overlap in knowledge and task management. This type of culture in a workplace and the confidentiality it requires can only be based on systematic facilitation and a supportive environment. This may also aid nurses in their desire for confidence and security and help to develop their skills.
Limitations
The scope of the study is small but the nurses’ rich descriptions of working alone and dealing with complex cases will have relevance in other similar settings around the world. The study was carried out in 2012 but has continued relevance as the working environment for these community nurses has not changed in complexity. It can be regarded as a limitation that the study was conducted in one municipality. However, previous research has documented the relevance of our findings in other contexts. The authors see the necessity of further action research studies involving community nurses.
Concluding comments
Our study suggests that experienced nurses employ a range of strategies to compensate for systems that do not support nursing competence and the safety of patients. While this seems to work in the short term, it is not an ideal situation. It is important to have time, to provide relevant information and to have an overview of collegial skills to enable nurses to have access to the knowledge they require and to share knowledge when necessary. It also seems evident that nurses must have the opportunity to maintain and develop their cooperation with colleagues so that the professional quality of care becomes a shared responsibility. Even though our study shows that the experienced nurses are able to deal with challenging situations, they need support. The responsibility to facilitate a supportive workplace environment, develop systems for competence development and adequate information access lies with management. The contribution from management is essential, in being attentive to employees’ expressed concerns and by creating working conditions that satisfy the professional judgement of experienced nurses. If nurses are expected to adapt to a new work situation, they are dependent on an attentive management that listens and supports. 39 Even though this managerial dimension is beyond the scope of this study, it is an interesting theme for further research.
This study emphasises that experienced nurses and their dedication to safe practice can significantly contribute to establishing a more systematic approach to training and information access. This approach is important to the experienced nurses, but much more so for inexperienced nurses who depend on their expert colleagues to develop their clinical skills. We encourage further studies on how novice nurses handle situations with new work tasks that challenge their existing skills.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.