
Abstract
Pain is a major health problem that has a huge impact on public health. Pain is also the most common reason for patients to seek care at the emergency department. Data were collected at seven emergency departments in Stockholm, Sweden, over 24 hours. Data were gathered from patients via a questionnaire conducted by the triage nurse during the first assessment on arrival. The patient-reported pain intensity was classified and the patients were grouped into age categories. Univariate and multivariate binary logistic regressions were conducted to determine the association between pain and variables: sex, age and taking analgesics prior to the visit. During the 24-hour period, 1344 patients visited the emergency departments and 647 patients (48%) participated in this study. Thirty per cent of the patients reported a pain intensity of eight or more. Despite this, only 33% of the patients took analgesia before visiting the emergency department. The odds of reporting pain were nearly six times higher for a person aged less than 30 years compared to a person over 60 years of age. The differences in the patients’ pain ratings according to age need to be highlighted. Effort on preventive health education should be studied.
Introduction
Pain is a major health problem that has a huge impact on public health by considerably complicating daily activities and sleep. 1 Pain is also the most common reason for patients to seek care at the emergency department (ED). 2 The International Association for the Study of Pain (IASP) defines pain as ‘An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage’. 3
As pain is a sensory and emotional experience, objective measures of pain are difficult to achieve. Extensive efforts have been made to find techniques aiming to solve the measurement problems. Studies state that high pulse rate, high blood pressure and increased respiratory rate can result from intensive pain.4,5 However, the results of Lord and Woollard showed no statistically or clinically significant associations between pain severity score and pulse rate or systolic blood pressure. 6 Since the definition of pain particularly stresses that pain is a subjective experience, patients’ views of pain should be considered when assessing and caring for patients at the ED. Moreover, research has shown that ED personnel have difficulty assessing patients’ subjective pain due to their attitudes and lack of training.7–9 In Sweden, nurses are responsible for assessing pain and treat according to protocol. Nurses have a unique position and opportunity, acting as gatekeepers as at the ED. Despite the wide knowledge existing on factors that affect pain assessment and the risk of long-term complications for patients who are not treated for pain during their ED stay, there is a lack of studies on patients’ own descriptions of pain during emergency care.2,10 The aim of this study is to describe acute pain from the patients’ viewpoint and to consider their own pain medication prior to attending the ED.
Method
Study design and setting
There are seven urban teaching hospitals in Stockholm, Sweden. A prospective survey was conducted in the EDs of these hospitals. On 31 December 2009, the municipality of Stockholm had around 830,000 inhabitants and more than two million lived in the county of Stockholm. 11 In Sweden, unlike many other countries, no referral is needed to seek care at an ED. At the ED in all seven hospitals the routine when a patient arrives by means other than an ambulance is: First, he/she is assessed by the triage nurse. If the patient is in need of pain relief, the triage nurse may administer oral and/or intravenous pain medication according to an analgesic protocol. Usually, the analgesics given are paracetamol, Non Steroidal Anti-inflammatory Drugs (NSAIDs), drugs with paracetamol and codeine in combination, or opioids such as morphine.
Data collection
Data were collected over 24 hours from 7.00 am on 18 May (Monday) until 7.00 am on 19 May (Tuesday) 2009. Data were gathered from the patients via a questionnaire conducted as an interview by the triage nurse in connection with the first assessment on the patient’s arrival at the ED. Inclusion criteria were: age > 15 years, Swedish-speaking and giving verbal and written consent to participate in the study. Exclusion criteria were: Patients requiring an instant response by the trauma team or who were critically ill. The triage nurse conducted the data collection and completed the questionnaire guided by the answers given by the patient during the first assessment. Apart from demographic data, patients were asked: 1) if they were in pain or not, 2) if they had taken any analgesics to alleviate the pain before arriving at the emergency department, 3) to rate the severity of pain on an 10-point scale (Numeric Rating Scale [NRS] – considered to be an appropriate pain-rating scale in the ED and is used internationally and nationally12,13), and finally 4) to describe the location of the pain. Before the start of the study a group consisting of ten emergency nurses and two social workers discussed the questionnaire to validate its purpose and ensure it could be understood by the patients included in the study.
Data analysis
Patient-reported pain intensity was classified into four categories: no pain (0 on the NRS), mild pain (1–4 on the NRS), moderate pain (5–7 on the NRS) and severe pain (8–10 on the NRS). This classification of pain severity has previously been used by Calil et al. 14 The patients were grouped into five age categories: younger than 30, 31–40, 41–50, 51–60 and older than 60 years.
Descriptive statistics were calculated for all variables. Univariate and multivariate binary logistic regressions were conducted to determine the association between pain and variables: sex, age and taking analgesics prior to the visit. P-values less than 0.05 were considered significant. Data were analysed by using IBM Statistics version 20 (IBM Corporation, Route 100 Somer, NY 10589).
Ethical considerations
Ethical permission for the survey was given by the local ethics committee at Karolinska Institutet in Stockholm (2008/991–31/3). Verbal and written consent were obtained after patients had been informed about the study by the triage nurse.
Results
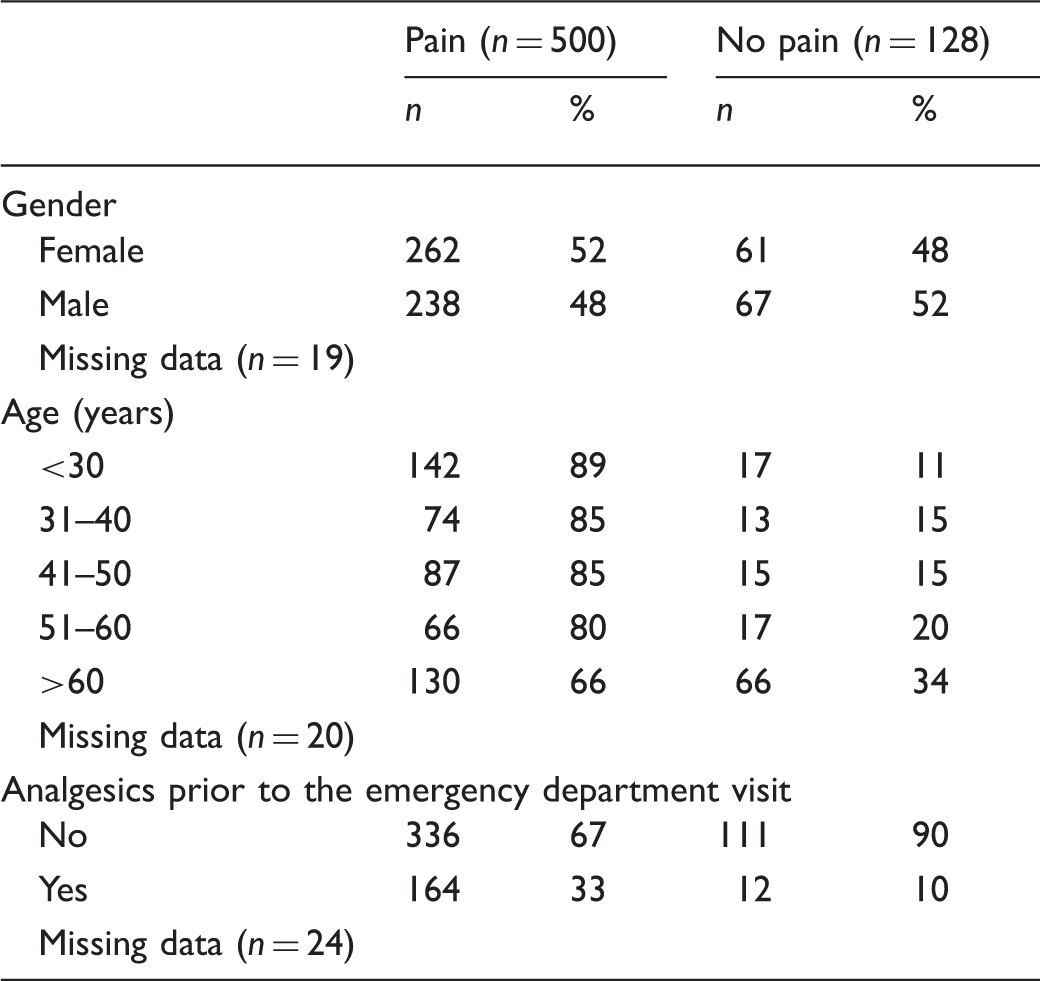
Characteristics of patients admitted to emergency departments in Stockholm County Council over 24 hours.
In the group of patients with reported pain, 69% reported a moderate to severe pain (NRS > 5) and 30% of the patients had a pain intensity of eight or more (Figure 1).
Numeric Rating Scale pain score values among patients who reported pain (N = 495).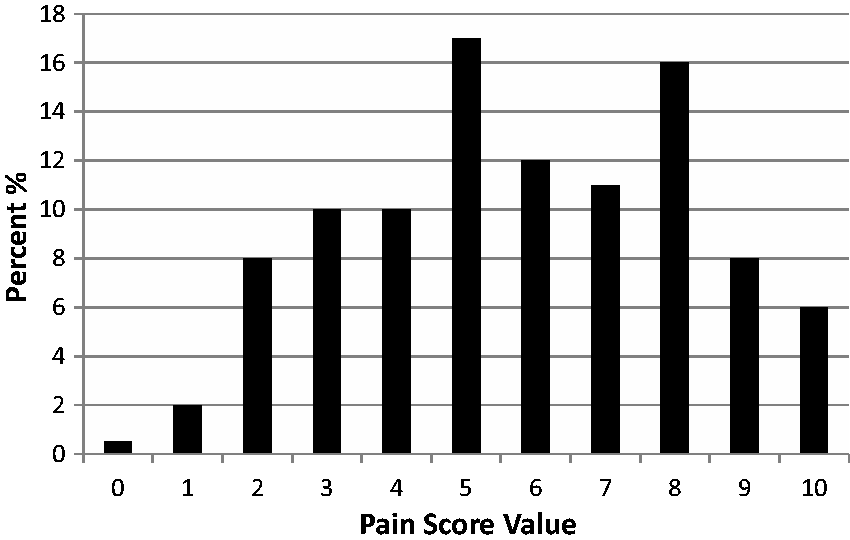
The association between pain and sex, age or taking analgesics in patients included in the study.
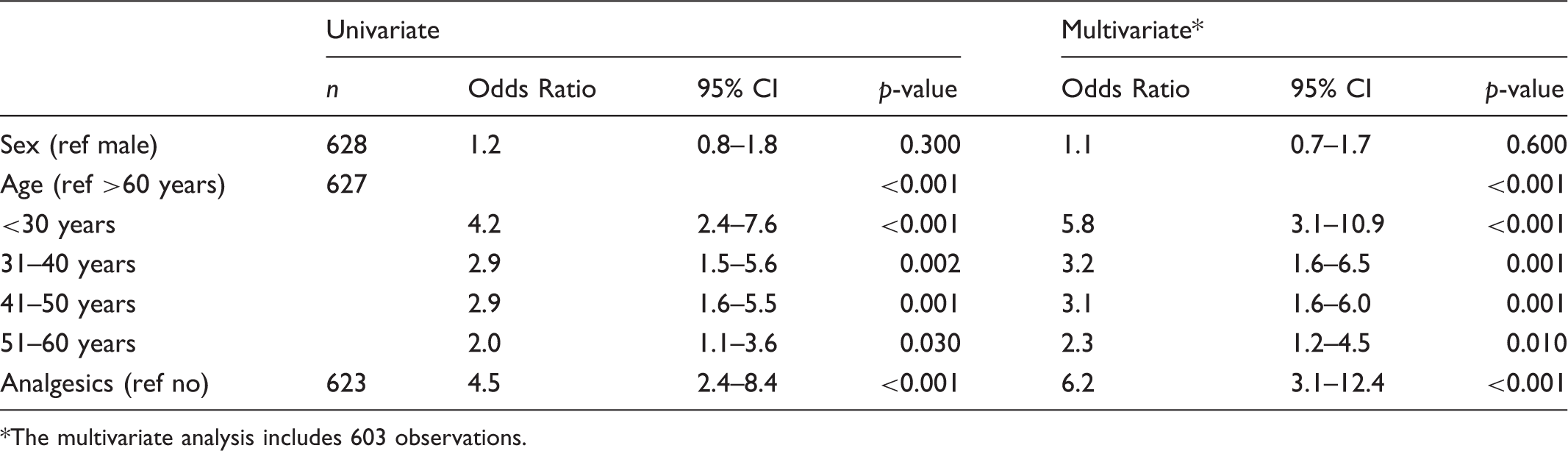
The multivariate analysis includes 603 observations.
Of the 508 patients with reported pain, 336 patients (67%) had not taken any pain medication prior to attending the emergency department (Table 1). There was no significant difference between gender and whether or not patients had taken any pain medication prior to attending the ED (chi-2 = 2.8, df = 1, p = 0.9). The two most common analgesics used by patients prior to attending the ED were paracetamol and NSAIDs. The most common locations of pain reported by the patients were: thoracal 25%, abdomen/genitals 25% and lower extremity 25%.
Discussion
This study was conducted to gain a better understanding of pain experienced by patients who visit emergency departments, and, as our results show, age had an impact on the reported pain ratings. The odds of having pain were nearly six times higher for a person <30 years of age compared to a person >60 years old. It seems that older patients assess their pain as lower on the NRS compared to younger people. The perception of pain from myocardial ischemia in the elderly has been shown to be significantly less severe compared to that perceived by younger patients. 15 There are also results indicating that younger patients with an acute painful condition tend to estimate their pain as more severe than older patients. 16 The threshold for pain is more likely to be higher in older people when the stimulus is brief, of lesser extent, and at peripheral cutaneous or visceral sites. 17
The differences in the patients’ pain ratings according to age should be highlighted in the clinical setting as emergency nurses are the gatekeepers for detecting pain to ensure that correct treatment is given. In the guidelines of Stockholm County Council, pain ratings over three should be treated with medication to minimise the risk of complications. Many of our patients reported severe pain (NRS > 8) and this should be highlighted, since pain affects perceived health. It is well known that untreated pain can prolong the recovery period, increase the length of hospital stay, and create long-lasting psychological and emotional stress for the patient. 4 However, studies from the acute care setting are lacking. Despite reporting severe pain, only 33% of the patients took analgesia before visiting the ED. The reason for not taking any pain medication is not known but could be related to the fact that some patients did not want to take pain-relieving drugs unnecessarily 18 or that they were worried about side effects of analgesics. 19 Our results show an increase in the number of patients taking analgesia as compared to the results of Fullarton which showed that 19% had taken analgesia before attending the ED. 20 Self-medication prior to the ED visit was most often seen in patients with pain located in the lower extremities. Finding the reason for this difference was not an aim of our study but should be considered in future research to further emphasise that pain is a vital sign of serious health risk along with abnormal respiratory rate or blood pressure.
Gender differences in pain perception have been reported, with men less sensitive and less willing to report pain compared to women. 21 However, this is not in line with our result, which showed no gender differences in reported pain, or in the patients’ own management of pain.
Establishing standards of clinical nursing practice in both chronic and acute pain management in different clinical settings should be encouraged. This study shows that a great number of patients attending emergency departments suffer from pain. These results are similar to those described by Todd et al. 22 Further studies to find ways to improve patient care, and perceived care, are necessary. High quality pain care exercised by nurses who have a clear understanding of the patient’s own perception of acute pain should be stimulated in the future.
Limitations
A potential limitation of our study is that the number of patients who declined to participate in this study or who were excluded due to the severity of their illness may have caused a selection bias. It is possible that the patients who participated were seeking medical attention in relation to pain; however, quite a few reported no pain, and whether or not the patients not included in this study reported pain is not known since no comparison between participants and non-participants was conducted. The amount of missing data is about 4% (Table 1) and is due to the triage nurse having to fill in the questionnaire at the same time as filling in the ordinary chart, or to the fact that the patient did not understand Swedish. This is considered insignificant as regards the outcome of the investigation.
Another limitation is that data are somewhat dated as they were collected in 2009. However, we have conducted a small confirming data collection at one of the hospitals in March 2016 (not published), and are confident that our data are still valid.
Despite these limitations we think that our study gives a realistic picture of the actual situation regarding pain in patients seeking emergency care in Stockholm.
Implications
The differences in the patients’ pain ratings according to age should be highlighted in the clinical setting as emergency nurses are the gatekeepers for detecting pain and ensuring that the correct treatment is given. Establishing standards of clinical nursing practice in both chronic and acute pain management in different clinical settings should be encouraged. Finally, the study raises the issue of patient education regarding self-medication. Perhaps it is possible for emergency nurses to participate in a general education programme before people seek care at the emergency department. The prevalence of personal technology, especially ‘smart’ mobile telephones, creates opportunities for new ways of delivering health care services and for service integration. These developments give an opportunity for individuals to have improved access to care as well as choice of care when new companies, products, technologies and service providers enter the market. eHealth solutions have the potential to reduce costs as well as to meet consumers’ rising expectations for quality and availability. This could also reduce the burden on health care organisations and ultimately improve continuity of care for the individual.
We do not recommend that ER nurses should actively go out and meet citizens, but we do suggest that ER nurses with their unique knowledge are an appropriate resource for educating people and providing information about pain and pain-treatment before they seek care.
Conclusion
Describing the pain characteristics of the enrolled patients with acute pain could help us understand the nature of pain from the patients’ viewpoints. Thirty per cent of patients reported a pain intensity of eight or more. Despite this, only 33% of the patients took analgesia before visiting the ED. The odds of reporting pain were nearly six times higher for a person aged less than 30 years compared to a person over 60 years old. The differences in patients’ pain ratings according to age need to be highlighted in the clinical setting.
This article could be used as a reference point when introducing new technology for education and prevention as well as self-care implementation of pain management.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.