
Abstract
Objective
Abdominal examination findings in pediatric acute appendicitis (AA) significantly vary by age. Therefore, grading systems have been developed for diagnosing pediatric appendicitis, and laboratory and radiological findings have an important role in this diagnosis. However, there is a need to develop new parameters for diagnosing AA. This study aimed to investigate the diagnostic value of platelet indices in AA.
Methods
This retrospective, observational study included 207 pediatric patients who were admitted to the Emergency Department and operated on for AA. The patients were divided into three groups on the basis of their surgical and histopathological findings (non-AA, uncomplicated AA, and complicated AA).
Results
There was no significant difference in the mean platelet volume/platelet count (MPV/PC) ratio among the groups. The white blood cell (WBC) count and the MPV/PC ratio showed a significant negative relationship (r = −0.239). The specificity for MPV was 61.8% and the sensitivity was 68.8%. Receiver operating curve analysis of WBC and MPV showed significance for diagnosing AA.
Conclusion
There is a negative, but weak, relationship between the WBC count and the MPV/PC ratio. However, the MPV/PC ratio could be a useful parameter for diagnosing pediatric AA according to receiver operating curve analysis.
Keywords
Introduction
Acute appendicitis (AA) is the most common cause of acute abdomen in patients who are admitted to the emergency room with abdominal pain in childhood. Unlike appendicitis in adulthood, children are more likely to develop perforated appendicitis (20% to 70%).1–6 Furthermore, pre-school children have difficulty in expressing themselves during taking history from the patients and their relatives, and this causes additional difficulties in diagnosis. Abdominal examination findings in pediatric appendicitis significantly vary by age. Expecting the classic clinical features of AA is often misleading. Observing specific examination findings, as well as diffuse, defense, and rebound tenderness, in young children is difficult.7,8 Therefore, grading systems have been developed for diagnosing pediatric appendicitis, and laboratory and radiological findings have an important role in this diagnosis.7,9 Despite the presence of important parameters, such as white blood cells (WBCs), the proportion of polymorphonuclear leukocytes, and C-reactive protein, making a definitive diagnosis of AA is still not easy for clinicians. Therefore, there is a need to develop new parameters.
Platelet indices consist of the mean platelet volume (MPV), platelet count (PC), and plateletcrit (PCT) parameters. Various studies have been carried out on the role of platelet index components, such as the PC and MPV, in the diagnosis of inflammatory disease.10–12 The MPV/PC ratio can be used as a parameter in diagnosing AA, especially because MPV can act as an acute phase reactant in acute inflammatory events and its inverse relationship with PC. 13 Although there are limited studies on this subject in the literature, these studies have only been carried out in adults.1,2,6,7,9 To the best of our knowledge, there have been no studies on the MPV/PC ratio for diagnosing childhood AA. Therefore, this study aimed to investigate the diagnostic value of MPV and the MPV/PC ratio in pediatric patients with AA.
Materials and methods
Patients and study design
This study was conducted as a retrospective evaluation of patients who were admitted to Gaziantep Şehitkamil State Hospital Emergency Department between September 2016 and September 2017. Informed consent was not obtained because the study was conducted using electronic records of the hospital and the identity of the patients was protected so that patients could not be identified. Ethics committee approval for the study protocol was obtained from Hasan Kalyoncu University (02/10/18; decision no: 2018-07).
Patients who were admitted to the Emergency Department with abdominal pain, who were under 16 years of age, and who had clinical, laboratory and radiological findings compatible with AA were included in the study. For this study, all records of patients were evaluated using the first physical examination in the Emergency Department, operative notes, and histopathological diagnosis. One pediatric surgeon and two emergency medicine physicians evaluated the data and patients were divided into three groups: no appendicitis (non-AA group, normal appendix tissue); uncomplicated AA (both surgical and histopathological diagnosis); and complicated AA, such as plastron appendicitis, perforation, and periappendicular abscess (both surgical and histopathological diagnosis).
A total of 223 patients were operated on for AA. Patients who had presented because of acute abdomen and who had undergone previous surgery for AA, patients with chronic inflammatory disease, chronic infectious disease, and chronic liver and kidney disease, and patients who used drugs that may have affected their PC during admission were excluded from the study.
Age, sex, surgical and histopathological examination results, WBC count, PC, PCT, MPV, and the MPV/PC ratio were recorded in all patients who were included in the study.
Laboratory examinations
Blood was collected and placed in EDTA blood tubes for measuring the leukocyte count, PC, and MPV. These variables were measured using the electrical impedance method (LH780, Beckman Coulter, Miami, FL, USA). The normal reference values for the parameters measured in our study were as follows: WBC count, 4.5 to 10.0 × 103/L; PCT, 0.15% to 0.7%; PC, 150 to 400 × 103/L; and MPV, 7.4 to 10.4 fL. Reference ranges were provided by the biochemistry laboratory of Şehitkamil State Hospital.
Statistical analysis
Conformity of the data to a normal distribution was tested using the Shapiro–Wilk test. One-way analysis of variance and least significant difference multiple comparison tests were used for comparison of numerical data in more than two independent groups. The Kruskal–Wallis test and pairwise multiple comparison tests were used for non-normally distributed data. Numerical variables are shown as the mean ± standard deviation and categorical variables are shown as number and percentage for descriptive statistics. The SPSS Windows version 24 package program was used for statistical analysis (IBM Corp. Armonk, NY, USA) and a p value of <0.05 was considered statistically significant. The predictive ability of the WBC count, PCT, MPV, PC, and MPV/PC parameters in diagnosing appendicitis were tested by receiver operating curve analysis, and sensitivity, specificity, and area under the curve (AUC) values were calculated.
Results
A total of 207 patients were included in our study. A total of 130 (62.8%) patients were boys and the patients’ mean age was 11.5 ± 3.4 years. The mean WBC count, PC MPV, and MPV/PC ratio are shown in Table 1.
Age and laboratory results.
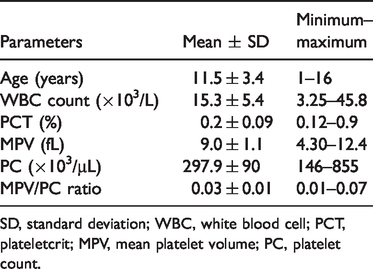
SD, standard deviation; WBC, white blood cell; PCT, plateletcrit; MPV, mean platelet volume; PC, platelet count.
The patients were categorized into three groups. In 16.4% (n = 34) of the patients who underwent surgery, the diagnosis of AA was not supported by surgical and histopathological examinations. The number and percentage of patients in each group are shown in Table 2. The mean WBC count was highest in the complicated AA group, with a significant difference among the groups (p = 0.001). The mean PC was highest in the non-AA group, but there was no significant difference among the groups. The mean PCT was highest in the non-AA group, with a significant difference among the groups (p = 0.047). Mean MPV was highest in the non-AA group, with a significant difference among the groups (p = 0.026). The MPV/PC ratio was highest in the non-AA group, but there was no significant difference among the groups. The WBC count and MPV/PC ratio showed a negative significant relationship (p < 0.05, r = −0.239) (Table 3).
Patient groups.

AA, acute appendicitis.
Hematological parameters.

SD, standard deviation; AA, acute appendicitis; WBC, white blood cell; PCT, plateletcrit; MPV, mean platelet volume; PC, platelet count.
Receiver operating curve analysis showed that the WBC count and MPV were significant predictors of diagnostic performance of AA (both p < 0.05; AUC value: >0.5) (Figure 1). Accordingly, for diagnosis of AA, a WBC count of ≥14,200/mm3 had a sensitivity of 67.1% and a specificity of 70.6%, while the AUC value was 0.702 (p = 0.001). The specificity for MPV was 61.8% and the sensitivity was 68.8%, with an AUC value of 0.641 (p = 0.010). The cut-off values of PCT, the PC, and the MPV/PC ratio were not significant for diagnosis of AA (Table 4).

Receiver operating characteristic curve of parameters.
Diagnostic performance characteristics for parameters.
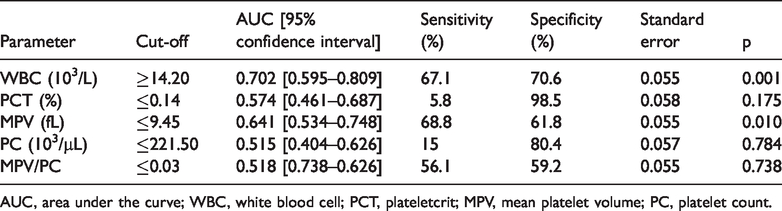
AUC, area under the curve; WBC, white blood cell; PCT, plateletcrit; MPV, mean platelet volume; PC, platelet count.
Discussion
Studies on pediatric AA have shown that the mean age of AA cases is approximately 10 to 12 years and it is more common in boys.9,13–15 Our findings regarding age and sex distribution are consistent with the literature.9,13–15 However, according to surgical and histopathological examinations, our case rates that were not supported by a diagnosis of AA are higher than those in some previous studies. 16
The WBC count in diagnosis of pediatric AA is an important parameter that is also used in scoring systems.17,18 In a meta-analysis, Andersson found that a high WBC count had a sensitivity of 83% and a specificity of 67% for AA. 19 In our study, the WBC count was significantly higher in patients with AA than in those without AA, which is consistent with other studies in adults and children,17–19 and it had a strong diagnostic feature (AUC: 0.702). Previous studies that compared the WBC count in pediatric and adult patients showed that the WBC count was higher in complicated AA compared with AA and non-AA.20–23 Consistent with the literature, in our study, the WBC count was significantly higher in the complicated AA group compared with the other groups.
In complete blood count measurements, the PC, PCT, and MPV, which are platelet indices, are also calculated. Platelets, which have important roles in hemostasis and thrombosis, are involved in microbial host defense, wound healing, angiogenesis, and the inflammation process. 24 Previous studies showed no significant difference in the PC between patients with AA and those without AA.23,25–29 The results of the PC in our study are consistent with these studies.
PCT is defined as the volume occupied by platelets in the blood. Yilmaz et al. 30 found no significant relationship between PCT and AA in pediatric patients with AA. However, in our study, PCT was significantly different among the groups. The PCT value was lowest in the uncomplicated AA group, while PCT values were similar between the non-AA and complicated AA groups. We consider that the diagnostic significance between PCT values and AA should be confirmed by larger studies.
MPV increases and decreases under some inflammatory conditions and acts as a positive and negative acute phase reactant. 25 In our study, we found that mean MPV was highest in the non-AA group, with a significant difference among the groups. Although some previous studies showed a low MPV in patients with AA, this was not significant.21,23,31,32 Low MPV values were also found in uncomplicated and complicated AA cases, but this was not significant.23,32 However, a meta-analysis showed a significantly lower MPV in patients with AA compared with controls (weighted mean difference, −0.64; 95% confidence interval, −0.74 to −0.54; p = 0.037). 33 In our study, the finding of a low MPV in AA is consistent with this previous literature. Furthermore, in our study, MPV showed significance for diagnosing AA.
Studies have shown that the circulating PC has a negative relationship with MPV in inflammatory events, and as a result, the MPV/PC ratio may be significant. The prognostic value of the PC has been studied in diseases, such as myocardial infarction, sepsis, deep vein thrombosis, and cerebrovascular disease.34–37 A study conducted by Biricik et al. 23 in adult patients showed that there was no significant difference in the MPV/PC ratio between patients with AA and those without AA. These authors concluded that the MPV/PC ratio was not useful for diagnosing AA. Similarly, we did not find a significant difference in the MPV/PC ratio among the groups. However, we believe that the relationship between MPV and PC should be investigated in larger population studies because of the significant result of MPV in AA cases. In our study, the WBC count and the MPV/PC ratio showed opposite findings in the groups, with an increase in the WBC and a decrease in the MPV/PC ratio count from the non-AA group to the AA groups. When these two parameters were compared, there was a significant, but weak, relationship between them. This correlation could indicate clinical progression if supported by data from larger studies.
Conclusions
The study shows that there is a negative, but weak, relationship between the WBC count and the MPV/PC ratio. The MPV/PC ratio could be a useful parameter in diagnosing pediatric AA according to receiver operating curve analysis.
Footnotes
Availability of data and materials
Raw data are available upon request.
Author contributions
MMO conceived, designed and supervised the study. MB and STÇ gathered resources. MMO and MS developed materials. MB, HG, and STÇ conducted data collection and/or processing. HG conducted analysis and/or interpretation; MMO and MS conducted the literature search. MMO, MS, and MB wrote the manuscript. MMO and SHE provided a critical review of the manuscript.
Declaration of conflicting interest
The authors declared that there is no potential conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.