
Abstract
Documentation in the patient record must be systematic and rigorous. However, each health care profession documents parts of the electronic health record (EHR) separately. This system can lead to double documentation. The aim of the study was to describe the amount of double documentation in health records for in-patients. A retrospective descriptive review of 30 records for in-patients diagnosed with hip fracture was conducted. Double documentation occurred on all records reviewed during the stay in hospital and in or between all professions reviewed. In total, 822 instances of double documentation were found. The EHRs available today are not designed to monitor processes. Instead, they follow each health profession, which can lead to double documentation. It would be desirable to develop an EHR from a process perspective and not a record per profession.
Introduction
Documentation is a necessity to ensure that patients receive proper and safe care, and documentation is an important area of expertise of the health care professions. 1 The electronic health record (EHR) has been promoted as an important tool to improve quality of care, but no significant relationship between the use of EHRs and quality of care has been shown; it has been concluded that how the EHR is used is a critical determinant of the ultimate impact of EHRs in clinical practice.2,3
The structure of EHR systems is rarely described scientifically in the literature. 4 Swindells and Lusignan have pointed out that vendors offer very different EHR systems, which influences what is recorded as well as affecting health care delivery. 5 Often each health care profession contributes separately to the EHR. This separation of the record into sections according to profession can be time consuming and may be unsafe because responsibility for the documentation is unclear between health professionals. 6 The separation of the patient record can also lead to double documentation. Galster’s definition of double documentation is ‘an entry in the patient record of information that already exists’ (p. 16). 7 To determine whether double documentation has taken place or not, account must be taken of the context or environment in which the assessment takes place. Examples are given of the recording of weight. If a patient’s weight is recorded twice two days apart before surgery, this is deemed to be double documentation, but if a dialysis patient’s weight is recorded at the same intervals, this is not considered as double documentation because the weight is needed to perform the treatment. 8 Other examples are given: when the record text states both the year the patient was born and the patient’s age; or if it states that the patient is a smoker when there is already a note of how much the patient smokes each day. 7
It seems that double documentation is a well-known clinical problem but this is not so well confirmed in the scientific literature. Jensdóttir et al. 6 stated that double documentation was one characteristic of traditional documentation but no results were reported on the existence of double documentation. Nurses reported avoidance of double documentation as a benefit during testing of a technical device for mobile documentation. 9 Documentation of similar information on pain management was included in two or more places in the EHR in one third of the notes studied (n = 1347) and identified as duplicity of documentation. 10 Cowden and Johnson 8 examined whether information in 21 intake forms documenting the nursing admission process in an integrated health care delivery system could be consolidated. The result showed that 42% of the content appeared in more than one form. We also found one student thesis at advanced level, which stated that 15% of nursing documentation was also documented in other places in the EHR. 11
Therefore, the aim of this study was to describe the amount of double documentation between nurses, and between nurses and other professions in the EHRs of in-patients.
Methods
Design
A retrospective descriptive record review was carried out.
Sample
Patient records were obtained for all patients who had been diagnosed with and treated for hip fracture on an orthopedic ward at a western Swedish hospital over three months from February to April 2011. The patient records were stored in an EHR system, in which all health care professionals with documentation obligations worked. The EHR system has been developed in such a way that the different professions make their notes in different parts of the system. Most of the documentation was written as free text, and no standardized terminology was used, except International Classification of Diseases (ICD) codes. A paper checklist for pre and postoperative routine interventions was used when the patient was in the ward, but this was scanned into the EHR after the patient was discharged. All other documentation was added directly into the EHR by each profession.
Kind of information recorded by each profession represented in the EHR reviewed in this study.

Data collection
The authors collected the records regularly from the ward secretaries who printed patient records from the EHR for the care episodes. These printouts were gathered in a locked box in the secretaries’ room for collection.
Data analysis
A search of the relevant literature was performed to find out if there were any specific instruments available to identify double documentation involving nurses. No such instrument was found so a study-specific protocol was constructed. All authors were involved in the development and use of the study-specific protocol. In the protocol, the patient’s overall care episode was divided into three sections to make the review manageable: arrival, care processes, and discharge. In each section, there was room to note double documentation within and between professions as well as the presence of consistent and inconsistent double documentation; each example of double documentation was written in the protocol. As most of the documentation was written as free text, and no standardized terminology was used, we reviewed the semantic content of the documented parts.
Throughout the data processing, all patient records included in the study were read line by line (187 pages of documentation). All double-documented data were highlighted and classified according to arrival, care processes or discharge, between or within professions and whether it was consistent or inconsistent. Information that was highlighted could be a word, such as the diagnosis (e.g. hypertension) or a sentence or part of a sentence (e.g. living alone in an apartment, first floor, without home care). A whole sentence or part of a sentence was identified as one instance of double documentation when the content was coherent (e.g. a patient’s social status). All of the authors were involved in the discussion about what constituted double documentation. Once this was completed, each patient record was assessed based on the study-specific protocol and the number of instances of double documentation was identified for the care episode. The instances of double documentation found for all 30 patient records were then compiled. To validate the outcome of the data analysis, quotations from patient records were identified, and then reported together with the description.
In this record review, double documentation is defined as registration of information that already exists, 7 which means that the information exists in more than one place in the patient record but is not needed in more than one place. The information could be provided by the same profession or by several professions. The double documentation must exist in the original documents in the patient records; a copy of a document is not double documentation. An example of double documentation was when the physician recorded in the note from the emergency department that the patient had hypertension and diabetes mellitus and the nurse added the same information in the care history. Double documentation was grouped as consistent or inconsistent. Consistent double documentation had the same meaning and was repeated, for example, when both the physician and the nurse recorded in different places in the patient record that a patient had a hip fracture on the left side. Some double documentation was identified as inconsistent, when the purpose of the information was the same but the information was contradictory; for example, when the physician said that the patient had a hip fracture on the left side and the nurse said that the patient had a hip fracture on the right side. No levels of seriousness of the inconsistent information were identified. All double documentation that was not consistent was regarded as inconsistent.
Ethics
The World Medical Association’s Declaration of Helsinki 12 and the Swedish Act on Ethical Review of Research Involving Humans 13 were taken into account for the study. The study underwent regional ethics review (DNR 2010/670) and it was decided that no approval was needed from the participating patients because all materials used for this investigation were anonymous. However, participation was approved by the operations manager at the clinic by means of a signed form. Patient records were de-identified by the medical secretary at the clinic before they were submitted for review and could not be traced to individuals. Only information about sex and age was listed on the patient record.
Results
Summary of audited and reported professions.
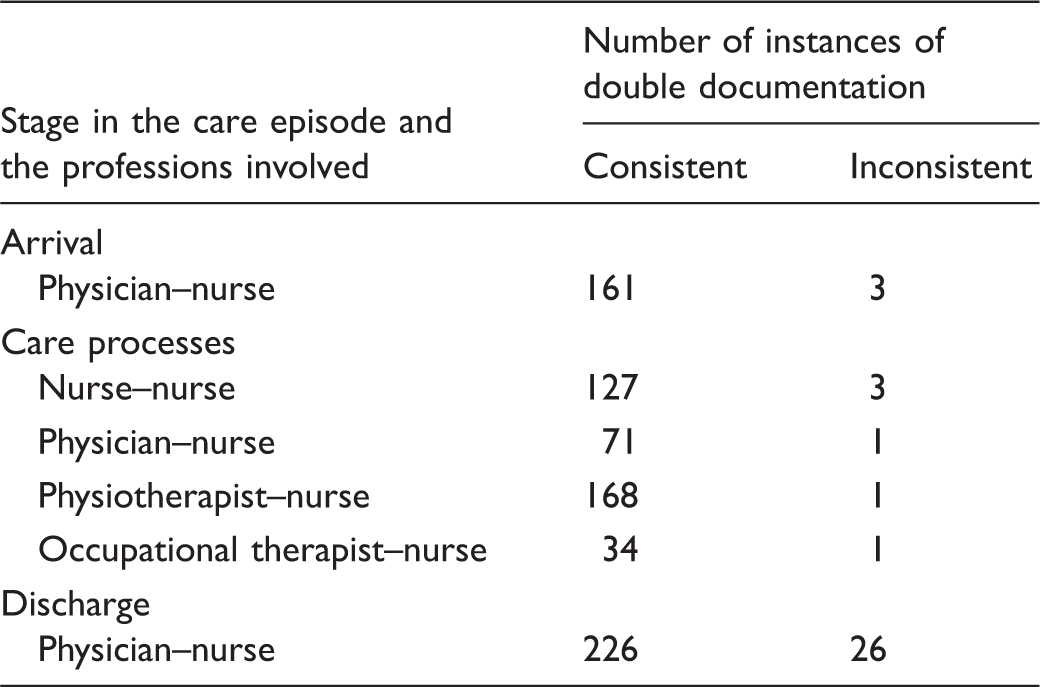
Number of instances of double documentation, when it occurred in the care episode and the professions involved.
Characteristics
The median age of the patients was 82 years (range 34–95 years). There were 19 women and 11 men. The median length of hospital stay was 11 days (range 4–22 days). The patient records covered 350 days of care. The care episodes included the day the patient arrived at the emergency department, all the days spent on the ward, and the day the patient was discharged.
Arrival
The review identified 161 occasions of consistent double documentation at the arrival stage, giving a mean value of 5.3 instances of double documentation per patient on arrival at the hospital. Data that were double documented included the cause of the contact (such as a fall) that resulted in a hip fracture, the preparation for surgery, pain relief and social data such as housing and help effort.
Note from the emergency department from a physician
Contact Reason: Right-sided cervical dislocated hip fracture. Garden 3. Present diseases: diabetes mellitus treated with tablets. Hypertension, angina. Social: Living alone in an apartment, first floor. No municipal assistance.
Care history of nurse
Contact Reason: Right-sided cervical dislocated hip fracture. Garden 3. Health history: diabetes mellitus treated with tablets, hypertension, angina. Social: Living alone in an apartment, first floor, without home care.
Care processes
Four hundred instances of consistent double documentation were identified during the care process on the ward, giving a mean value of 13.3 instances of double documentation per patient per care process. Nurses double documented within their own group on nursing status and the checklist or care plan. Physicians and nurses double documented by including in the physicians’ daily notes the same information already provided in the nursing status, the checklist or care plan. Double documentation between physiotherapists and nurses mostly involved the same information in the physiotherapist’s daily note as signed for by the nurse in the checklist. When the occupational therapist and the nurse double documented, the same information was in the occupational therapist’s daily notes and the nursing care status.
The nurses double documented in the paper-based checklist and nursing status data regarding catheters, diversions and inspection of dressings, existing or incipient pressure ulcers, bowel function and data on mobilization. Double documentation found in the nursing status and the care plan concerned coordinated care planning.
Documentation made by a nurse on two consecutive days
Nursing Status Round Note: Is in need of coordinated care plan. Care Plan Social Planning: Patient is in need of coordinated care plan.
Day notes made by physician Dr NN during round
Radiographic infiltrates and auscultatory also a lot of chatter and even basal reduced breath sounds on the right side. The patient has been coughing a lot but is afebrile. Inserting Cefamox 500 mg ×2
Nursing status by the responsible nurse
Round notes: Dr NN listened to patient’s lungs during the round and put him on antibiotic tablets against pneumonia.
Note from physiotherapist
Walking exercise: Go alone with walking frame out to the small dining room.
Checklist on the same day from the nurse
Training: Go with the walking frame, nurse signature/ 0 (0 stands for with no live support)
Six instances of inconsistent double documentation were found. Two instances concerned different timings of coordinated care plans and occurred between physician and nurse and occupational therapist and nurse. Three instances involved nursing care status and checklist concerning the number of existing peripheral venous catheters and different dates of catheter insertion and withdrawal. The sixth instance involved nurse and physiotherapist assessing the patient’s need for help differently.
Discharge
With regard to discharge of patients, 226 instances of consistent double documentation were identified. Of the 30 patient records reviewed, 28 included a nursing history. This resulted in a mean value of 8.1 instances of consistent double documentation in the history records from both the physician and the nurse. Double documentation occurred on length of stay, cause of contact, actions taken to correct the fracture, previous diseases, social data on housing, management of wounds and any remaining sutures or staples, follow-up inspections or visits, and temporary or continuous drug prescriptions.
Some nurses documented medical information, such as contact reason, previous diseases and how the fracture was corrected. A higher frequency of double documentation was identified in this part of the record.
History notes from the physician
Admission Reason: Arrives on 20 March as emergency case after trauma. X-ray shows a pertrochanteral femur fracture right. Surgery with a short intramedullary gamma nail.
Nursing report from nurse
Care process: 20 March, patient had fall at home. X-ray shows a right pertrochanteral femur fracture. Surgery carried out on 21 March with gamma nail.
History from the physician
Health Progress: Corrected 27 April 2011 with closed reposition and fixation with Twin Hook plate.
Nursing history from the nurse
Care process: 26 April 2011 surgery right hip with Twin Hook.
Discussion
The results of this study show that double documentation occurs throughout the care episode, both between nurses and other professionals and between nurses and other nurses. Double documentation is not always negative. Redundancy of information in EHRs could be considered as positive or negative according to Meum: positive in that it makes information available through time and coordinates different sources of information necessary to create continuity; negative from the view point of wasted time and work overload. 14
The professional split of the record is highlighted as a reason for double documentation. The EHR system used at this hospital has been developed in such a way that the different professions make their notes in different parts of the system. This means that, for example, a nurse prefers to read the documentation in the nurse section of the EHR instead of reading what another profession has documented in another part of the EHR. If the EHR system were structured to make it possible to work in an integrated way and focus on interdisciplinary processes, the amount of double documentation would decrease. Other factors could lead to double documentation, such as long lead times for typing dictated notes from physicians. Documentation by nurses is always available because they write everything up themselves during their shifts. This could be a reason for nurses to record medical information that the physician has maybe dictated but which is not yet available in the EHR. If physicians’ notes were added directly or by a secretary soon after dictation, the instances of double documentation would decrease and the workflow would probably improve. This result is supported by Laitinen et al., who found that documentation that was retrospective and distant in both time and space caused double documentation and led to reduced accuracy. 15
In this study, we found that nurses documented the same information as the other professions. This was unique to the nursing profession compared with the other professions. For example, medical information from the rounds was included in the nursing status. This result is in agreement with a study by Wang et al., which showed that nurses’ documentation consisted predominantly of biomedical information and that other important aspects were lacking. 16
Nursing documentation should not only consist of actions carried out; it should also show altered or unaltered condition and the basis on which decisions are made. 17 The importance of discussing and deciding how documentation should be carried out to ensure a sufficiently high quality of documentation has been pointed out; documenting as much as possible to show what has been done does not equate to high quality. 18 One reason nurses document so much may be to communicate that they have fulfilled their responsibilities for the patients in case of subsequent complaints from the patients or relatives. It was clear that nurses took a lot of responsibility for the documentation of other professions in the team surrounding the patient. For example, round notes were documented by nurses in the nursing status, and at the same time there was no daily note from the physician as would be expected. It is important that nurses continue to discuss the profession’s priorities, so that nurses take on their professional responsibilities, but it is also a management responsibility to ensure that the systems, knowledge and procedures exist to allow documentation to be done to a sufficient standard. Further, a use of more structural and standardized EHR could guide nurses towards less duplication. 10 According to the results of the present study, this is a crucial part of the development of the structure of EHR. Lluch has also described lack of trust in data entered by another health care professional as a barrier. 19 This may be a reason for which each professional documents the same information in the EHR.
In this study, there were 35 instances of inconsistent double documentation, of which 26 were at discharge. According to Swedish regulations, the processing of personal data must ensure that health care is conducted safely and that good quality is maintained. 20 How inconsistent information poses a risk for patient safety differs but essentially all forms of inconsistent information can be a risk. Because most instances occurred at discharge, inconsistent double documentation can lead to missed follow-up care.
In some cases where there was inconsistent double documentation in this study, it was difficult to know whether the physician or the nurse was right or wrong, whereas other cases showed clearly that whoever wrote or dictated the report from the care process had not read the previously recorded text, or otherwise was missing essential information in some way. This was considered a problem, as the follow-up care of patients in some cases depends on the information in the discharge notes, which was sometimes incorrect. If the EHR was backed up by better search engines, this could also contribute to the right information being found more easily, and lead to a reduction in double documentation.
Many instances of double documentation were generated when the same information was documented in several places in the EHR. As already discussed, one way to improve this is to develop the structure of the EHR system. An extensive literature review 19 has stated that the current structure was an organizational barrier to a health organizational system, and that team-based care strategies are the only way forward for care coordination supported by EHRs. The review also stated that there is a need for a multidisciplinary holistic design framework. Another review 21 has also stated that the non-existence of common rules and policies for sharing clinical data was a structural obstacle, and the non-existence of a consistent strategic plan was a concern with regard to health care information systems.
Also, standardized instruments improve both care and its documentation, 6 and should be used in EHR systems to improve documentation. Structured and standardized care of patients diagnosed with hip fracture leads to improved survival and reduced risk of complications. 22 One way of providing high-quality care and reducing double documentation is to use standardized care plans. A standardized care plan can be created for a group of patients with the same problems and should be based on current research review. 23 Most nurses believed that a standardized care plan increases their ability to give all patients the best care, and that if multi-professional standardized care plans were used, they would improve the patients’ chances of receiving high-quality care. Most nurses also believed that the use of a standardized care plan would reduce the time required for documentation and reduce the scope of the documentation. 24 As nearly all documentation was free text, different wording was used both within and between professions. This can be a risk when words can have different meanings, but in different contexts different degrees of precision are required to convey the concepts. An extensive review 25 showed that standardized nursing terminology was found to be essential for measuring, clarifying, and understanding nursing care. These same reasons apply for other professions to use standardized terminologies. If the terminologies are included in the EHR, the time spent writing can be reduced and the risk of misunderstanding can be minimized.
Methodological considerations
We have attempted to describe the analysis process fully and included quotations. Starting from a broad perspective, the amount of double documentation is described together with information on who double documented, where double documentation was done and what was double documented, all captured within the study-specific protocol. This approach gave a broad picture of all double documentation and could be used as a platform to continue research on this topic. Thirty records were considered sufficient to describe instances of double documentation because a clear pattern could be discerned from these records. The content can be interpreted differently but as most of the documentation took the form of free text this was the only way. All authors were involved in the review and interpretation of the content in the documentation. This record review consisted of 30 records from one unit and therefore cannot be generalized to other orthopedic units or other hospitals, but it does present awareness of an essential problem. The findings cannot be transferred to other contexts, so the amount of double documentation is an area that requires further study. The protocol used to audit patient records can be used to identify double documentation in other contexts.
Conclusion
Most instances of double documentation occurred during the care process and especially within the professional group of nurses and between physiotherapists and nurses. The difference in the number of instances of double documentation at arrival and discharge was dependent on how the nurse documented. The amount of medical information in the nurse documentation affected the frequency of double documentation. Thus, both consistent and inconsistent double documentation does occur in patient records at arrival, during the care process and in discharge notes. The structure of the EHR system is a crucial factor in avoiding double documentation; it needs to have a more multi-professional structure that is problem-oriented and therefore patient-centred. Further research is needed to find ways to structure the EHR so that double documentation is minimized, the time spent on documentation is reduced and the system supports patient safety.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.