
Abstract
This research studies whether children’s gender influences household adults’ perceptions of their illnesses and the pattern of seeking medical treatments for them, the aim of which is to understand to what extent minor girls (under 15) are discriminated against in Chinese rural households’ allocation of curative healthcare. Using the 2014 wave of China Family Panel Studies (CFPS), we find that households in rural China do allocate more medical resources to boys than girls. Gender differences mainly exist in children’s hospitalization rates and medical expenditures. Girls are especially disadvantaged as they grow older. They also face an added problem of sibling rivalry that leads to sick girls being less likely to be taken to a hospital when they have siblings of the same gender. These results suggest that sick girls in rural China may not be able to receive sufficient curative healthcare due to son preference. This is not only a threat to girls’ well-being, but also a potential cause of the imbalanced sex-ratio of the Chinese population.
Introduction
The sex-ratio of the Chinese population, especially for minors, has become increasingly imbalanced during the past few decades. According to the 2010 Population Census (NBS, 2010), the sex-ratio for children under 15 has reached 117, which is much higher than the world average level of 107 (CIA, 2010). This excess of males can be attributed mainly to the persistence of son preference, a Chinese tradition that treats sons as the more valued descendants of the household. Daughters, in contrast, are considered less valuable, since a girl will eventually leave her family of origin to live with her husband’s family. Son preference still influences the sex structure of the Chinese family, as well as the well-being of women and girls within it. For example, the impact of son preference on the use of prenatal sex selection and the high sex ratio at birth has received both social and academic attention. The high mortality rate of girls has also been studied, focusing mainly on female infanticide and the inadequacy of preventive healthcare that girls may receive due to son preference.
However, almost no systematic research has been conducted on the impact of son preference on households’ allocations of curative healthcare resources to sick children in China. Sick girls receiving sufficient household attention and proper medical treatment or the lack thereof indicates the severity of son preference within households. It also determines the general well-being and mortality rate of girls. This research, therefore, attempts to compare household adults’ healthcare-seeking behaviors for sick girls and boys in China. The study focuses on rural areas, where the desire for sons is more intense. Rural households are also more likely to have more than one child, 1 which enables within-household comparisons. Before making detailed analyses, we will briefly introduce the influence of son preference on Chinese girls’ birth rates, health conditions, and mortality rates, as well as households’ gendered allocation of preventive and curative healthcare resources in developing countries.
Son preference and Chinese girls’ disadvantages in health
The impacts of son preference on family formation and children’s well-being in China are well documented. Most past research has studied how families’ desires and preferences for sons influence households’ sex composition and girls’ education attainment and health. The discrimination against girls in households’ allocation of educational resources has been observed consistently in rural China. Son preference beliefs, combined with perceived financial returns, lead parents to have higher educational expectations for boys than for girls. Adolescent girls in rural China, in general, have lower education attainment and higher labor force participation rates compared with boys (Lee, 2012; Li and Tsang, 2003; Song and Appleton, 2006; Wang, 2005). However, one study also finds that despite mothers’ slightly higher expectations regarding boys’ education level, households’ actual investments in children’s education do not necessarily vary between boys and girls. Boys’ advantages in education outcomes are also rather modest (Hannum et al., 2009).
Focusing predominantly on the high sex ratio at birth, high mortality rate of girls, and girls’ disadvantages in preventive healthcare utilization, researchers have also studied the manner in which son preference impacts girls’ health and household sex composition in both rural and urban China. The high sex ratio at birth is one of the strongest indicators of son preference in China. The popularization of ultrasound technology combined with the enforcement of the one-child policy in the late 1970s has made prenatal sex-selection an increasingly common choice for households with son preferences (Chu, 2001; Goodkind, 2011; Hull, 1990; Poston et al., 1997). As a result, by 2010, the average sex ratio at birth had reached 121, and even 131 and 161 for the second and third child (NBS, 2010).
Furthermore, the abnormal excess of young girls’ mortality rate over that of boys has become prevalent in the past few decades, despite healthcare providers’ success in reducing the overall mortality rate of children under five (Cao et al., 1997, 2013; Das Gupta and Li, 1999; Han and Li, 1999). Unlike with prenatal selection, once the child is born, what contributes most to the imbalanced sex ratio is not usually state-enforced fertility, but the unequal distribution of household resources and the family’s intentional or unintentional neglect of girls (Attane, 2009; Li et al., 2004). The high mortality rate of girls may first be explained by their unfavorable position in households’ distribution of nutrition and preventive healthcare. For example, girls from households with more than one child are more likely to be shorter and weigh less than boys at an early age (Goode et al., 2014; Ren et al., 2014). Girls’ health is also more vulnerable to households’ economic difficulties and external social policy changes. For instance, the reform of the economy in the 1980s, which decreased health insurance coverage, especially in rural areas, enlarged the gender gap for immunization among children (Xie and Dow, 2005). Along with biases in preventive healthcare, households’ gendered allocation of curative healthcare resources has also been found in many countries to provide an important explanation for girls’ disadvantages in health and survival rates (Asfaw et al., 2010; Pokhrel and Sauerborn, 2004; Sachar et al., 1990). Yet until now, relatively limited attention has been paid to the medical treatments that sick boys and girls receive in China.
Current studies on curative healthcare utilization have focused not only on factors that determine the choice of healthcare, but also on the process of deciding whether to use certain types of healthcare. While the former type has attracted the most quantitative studies, the quantification of the decision-making process has also received increasing attention. For example, Pokhrel and Sauerborn (2004) have constructed the four hierarchical steps of ‘perception of illness,’ ‘seeking care,’ ‘choose a provider,’ and ‘health expenditure’ to measure how adults in households make the decision to seek medical care for children.
Aimed at understanding how children’s gender influences household adults’ healthcare-seeking behaviors for sick children in rural China, this research attempts to determine not only whether a gender impact exists, but also whether it persists throughout the whole process of healthcare seeking and if not, at which stage of decision-making the impact begins to appear. As a result, we divide household adults’ healthcare-seeking process for children into four steps and check the effect of children’s gender on each of these steps (see Figure 1). First, the probabilities of boys and girls being reported ill by caregivers are compared to see whether gender disparity exists in adults’ perceptions of children’s illnesses. Second, for children who have been reported ill, the gender difference in the utilization of healthcare services is analyzed by measuring whether sick boys have a higher chance of being taken to the hospital and of being hospitalized compared to sick girls. Third, since the pattern of healthcare utilization influences medical expenditures, the final step compares the medical expenditures on sick boys and sick girls. Furthermore, in order to understand the impact of children’s ages and sibling rivalries on the above mentioned gender differences, we also attempt to analyze whether the gender gap in healthcare utilization changes as children grow up, as well as whether siblings’ gender and age influence children’s chance of using curative healthcare.
The framework of analytic strategy.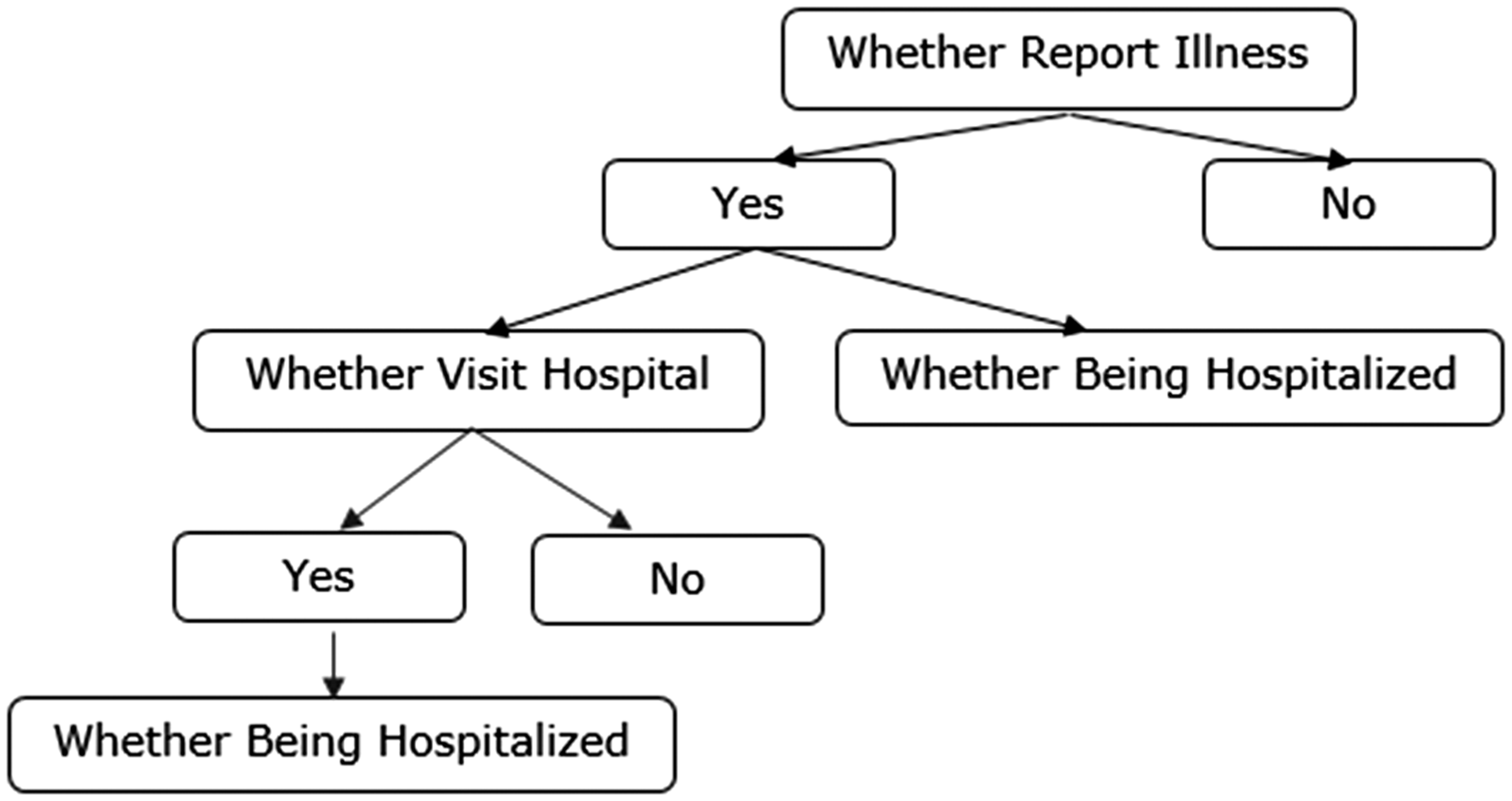
Gendered allocation of household medical resources among children and research hypotheses
Since Amartya Sen’s (1990) attempts to estimate the number of ‘missing women,’ which refers to the females who die due to discrimination, the abnormally high morbidity and mortality rates of female children in many countries have increasingly been revealed and studied. Girls’ disadvantages in households’ food allocation, feeding practices, and immunizations are being widely considered as the primary mechanisms behind it (Choudhury et al., 2000; Das Gupta, 1987, 1995; Jayachandran and Kuziemko, 2011; Larme, 1997; Messer, 1997; Miller, 1997). However, there are also studies showing that, in some areas, girls are at least as well-nourished as boys and that nutritional imbalance is not a dominant part of gender inequality (Hazarika, 2000; Kurz and Johnson-Welch, 1997; Li et al., 2004; Walker and Ryan, 1990). Meanwhile, a growing body of evidence has proven that girls are the victims of severe discrimination in terms of curative healthcare utilization.
Household adults’ healthcare-seeking pattern for sick children is highly gendered in many developing countries. Caregivers tend to report fewer illness symptoms for girls than for boys, although the differences are not always obvious and sometimes insignificant (Ahmed et al., 2001; Larme, 1997; Pokhrel and Sauerborn, 2004; Pokhrel et al., 2005; Rockers and McConnell, 2017; Willis et al., 2009). Relying almost exclusively on parents’ reports with no evidence on the real illness conditions of children, some of these studies choose to maintain cautious attitudes in their conclusions and leave spaces for further study (e.g. Pokhrel and Sauerborn, 2004; Willis et al., 2009). After all, biomedical evidence indicates greater male vulnerability during the neonatal period (Anker, 2007; Waldron, 1983), which means the gender disparity in illness reporting may simply be the result of boys’ fragility. However, in a study of children aged between 0 and 5 years in West Bengal, where children’s illness conditions were observed by a surveillance group, it was found that girls were more likely than boys to fall ill (Pandey et al., 2002). There are also places like rural Peru where parents reported boys to be healthier (Larme, 1997). Although still questionable, existing evidence does tend to indicate that the well-being of boys attracts more household attention and boys are more likely to be reported ill. H1: For children under 15 who live in the same household, boys are more likely than girls to be reported ill by household adults.
While Chinese households’ pattern of healthcare seeking for children of different genders has not been studied systematically, evidence can still be found in regional studies that focus on the causes of children’s deaths and the demographic characteristics of hospitalized children. From less developed rural areas to major cities like Beijing and Wenzhou, girls under five generally receive less treatment than boys before death. They are more likely to die at home or on the way to the hospital. Boys, in contrast, have a higher chance of being brought to better hospitals and hospitalized regardless of their geographical location or severity of illness (Lin et al., 2007; Song Y, 2008; Wang and Zhang, 2016; Xiao et al., 2012). Song L (2008) has also found that the medical expenditure for boys aged 6 or below in rural areas can be more than twice that for girls. H2: For sick children under 15 who live in the same household, sick boys are more likely than sick girls to be taken to the hospital and hospitalized by household adults. The medical expenditure for boys is, therefore, higher than that for girls. H3: Gender differences would be more severe for children under 6 compared with children aged between 7 and 15. H4: Girls receive less medical treatment when they have brothers, especially younger brothers. But parents’ healthcare-seeking behaviors for boys may not be influenced by the age and gender of the other children.
Data and sample
Our research draws on data from the 2014 wave of the China Family Panel Studies (CFPS), which provides adult, child, family economy, and community information on 13,946 households located in 29 provinces, along with 8616 children and 37,147 adults living in these households. The CFPS data was selected for this study first for its comprehensive collection of information. In addition to data on children’s illness and households’ healthcare-seeking behavior for children, which are available in the child dataset, information on family structure, household, and parents’ socioeconomic status can also be obtained from adult and family datasets. Second, and more importantly, the strength of the CFPS is embodied in its national representativeness and large sample size, which provides greater statistical power than other datasets for the making of inferences and interpretation (Xie and Hu 2014). This is especially crucial for our research since current studies on households’ gendered healthcare-seeking patterns for children usually use small-scale regional data, which makes the evidence rather scattered. Nationally representative survey data like the CFPS may then provide a more general view on this topic.
Characteristics of sampled population (percentage/mean (SD)).
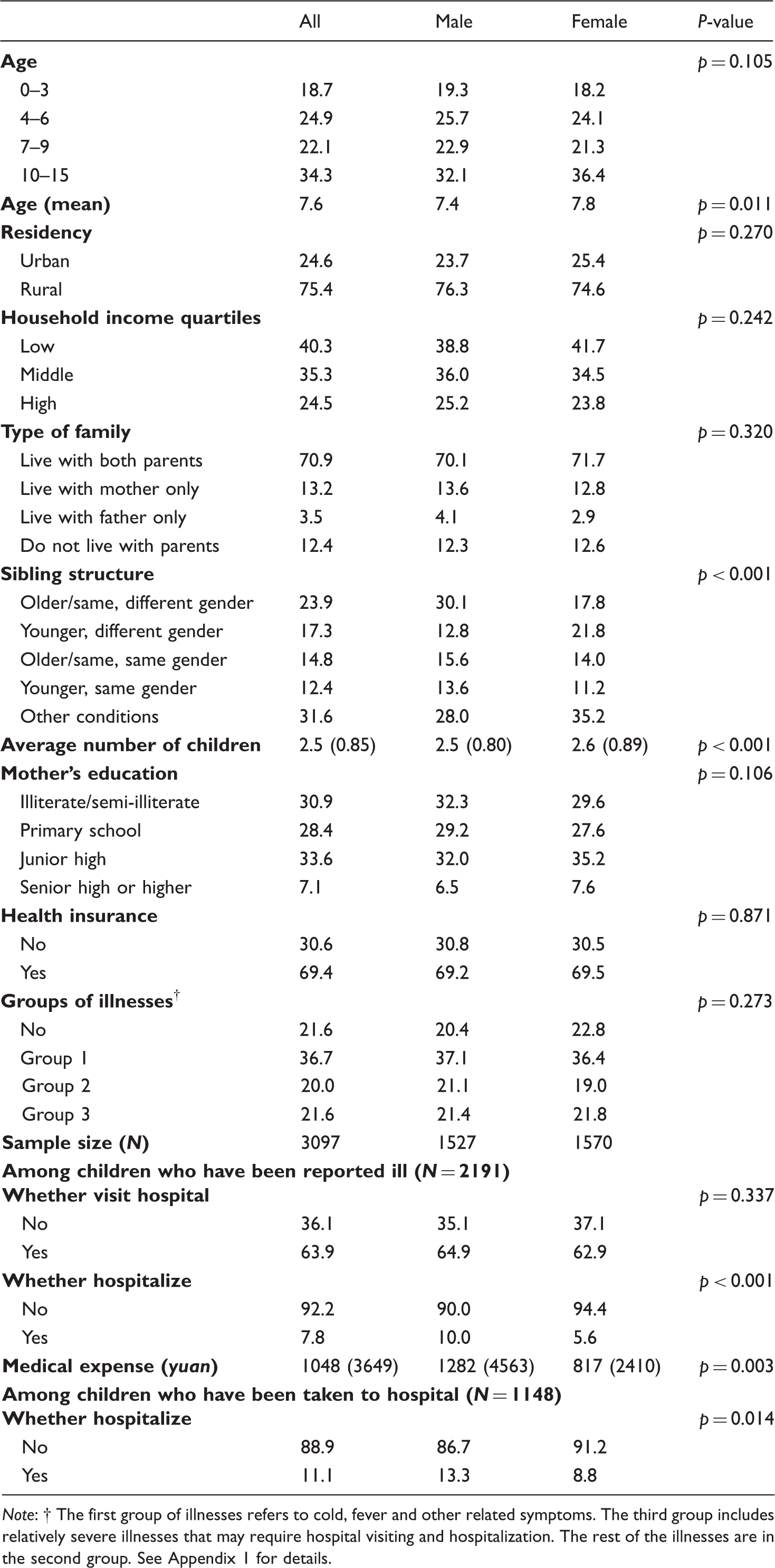
Note:
Variables and analytic strategies
Dependent variables
To analyze whether children’s gender influences households’ decision-making process on seeking healthcare for children, we chose four dependent variables. The first step was to be aware of and report the illness of children. In the adult-proxy report of the CFPS 2014 child dataset, if the child had been interviewed in the 2012 wave of the survey, the household adult who usually took care of the child would be asked to report the most severe illness the child had ever suffered in the past 12 months. The adult-proxy respondent of the newly entered child, instead, reported the most severe illness the child had had since birth. Thus, the newly born children could also be added into the sample for analysis. All reported illnesses were then coded according to the names or symptoms given by the respondents. Since the coding system was highly specific and consists of too many categories, for the convenience of analysis, illnesses were re-categorized into three groups. The first group referred to cold, fever, and other related symptoms. The third group included relatively severe illnesses that might require hospital visiting and hospitalization. The rest of the illnesses were categorized into the second group (see Appendix 1 for details). However, it must be emphasized that although the three categories of illness did have very different levels of severity, since the very severe level could not be accurately judged according to the codes, the categories were treated only as nominal, instead of ordinal.
The second step of decision-making, which is whether households seek external healthcare for sick children, was checked according to adult proxy respondent’s answer concerning whether the child had been taken to a hospital/medical center due to illness in the past 12 months (0 = no, 1 = yes). For the third step of decision-making, some studies (e.g. Pokhrel and Sauerborn, 2004; Willis et al., 2009) have focused on what kind of healthcare provider (public, private, or traditional) is chosen for sick children so as to measure the quality of healthcare that boys and girls receive. However, since such information is not available in the CFPS data and, as mentioned previously, gender disparity in children’s use of inpatient care has been found both in China and in many other developing countries, this research focused on whether the sick child had ever been hospitalized due to illness in the past 12 months (0 = no, 1 = yes) instead. The medical expenditures for sick boys and girls were then compared for the last step of decision-making.
Independent variables
Healthcare seeking for children is a decision made by households based on both the individual characteristics of children and the availability of healthcare facilities. Therefore, in addition to the child’s gender being the key indicator (0 = female, 1 = male), many other individual-, household-, and healthcare system-level factors were also included in our research as covariates. Children’s vulnerability to illness and household adults’ attitudes toward sick children may change according to children’s ages. A categorical variable with four age groups was, therefore, constructed to control age difference.
Families with limited resources are believed to be less likely to seek external medical help, which may intensify gender bias (Miller, 1997). For example, one study of the hospitalization of Indian children has shown that the probability of boys being hospitalized by financing from borrowing was much higher than that of girls (Asfaw et al., 2010). However, there are also opposing voices arguing that discrimination against female children may not be the result of economic hardship. Instead, conditions in relatively wealthy families are even more severe (Das Gupta, 1987; Miller, 1997). Due to large regional disparities and rural–urban gaps in income, household per capita income in itself may not be enough to measure Chinese households’ economic conditions (Xie and Zhou, 2014). Thus, the per capita incomes of households from different provinces were ranked separately and then included into models as a categorical variable with ‘low,’ ‘middle,’ and ‘high’ divisions. In addition, households with rural hukou may reside in urban areas. Therefore, the rural/urban residency of households was also adopted to control economic disparities.
Family size and family structure were controlled first through the number of children within each household. Since extended households are still not uncommon in rural China and many left-behind children also need to live with relatives, this number may be larger than the actual number of children each couple have. For sibling structure, since both sex composition and relative birth order may influence children’s health and healthcare utilization, we constructed five categories: ‘children with older or same age siblings of different gender only,’ ‘younger siblings of different gender only,’ ‘older or same age siblings of same gender only,’ ‘younger siblings of same gender only,’ and a final category that refers to more complex conditions, such as boys with both elder brothers and younger sisters, or girls with both younger brothers and sisters. Whether children live with parents (live with both parents, live with mother, live with father, or live with neither parent) was also controlled, since China has a large number of ‘left-behind’ children in rural areas who live without one or both of their parents. The physical and psychological vulnerability of these children and the lack of parental care for them have long been discussed (Gao et al., 2010; Li et al., 2015).
Mother’s education level was included as a covariate, since mothers’ increasing status and bargaining power in households can bring children better nutrition and healthcare, although to what extent girls can benefit from that is still controversial (Das Gupta, 1987; Richards et al., 2013). Information on mother’s employment and income conditions, and whether the mother was the head of household was either unavailable or had many missing values and hence could not be controlled. For similar reasons, only children’s access to social health insurance could be used to control healthcare system-level differences.
Analytic strategies
Logistic regression models were applied to the first three steps of decision-making. The report of illness was first specified as a binary logistic to see whether boys are generally more likely to be reported ill than girls. The reported illnesses were then divided into three categories and gender difference was rechecked utilizing multinomial logistic regression. Second, after excluding children who were not reported ill, a binary logistic model was adopted again to measure the difference between sick boys’ and sick girls’ chances of visiting a hospital. Third, the analysis of gender disparity in hospitalization rate also relied on binary logistic models. Comparison was made first among the 1148 sick children who visited a hospital, and then among all 2191 sick children. For the final step, the medical expenditure on sick children was estimated by ordinary least square (OLS). Since expenditure data are skewed and have some zeroes, we transformed it into a logarithmic scale after adding a small number of 1 [log10(x + 1)]. In order to check whether gender gaps shrink as children grow up, households with at least two children aged 0–6 (N = 804) and at least two children aged 7–15 (N = 1200) were extracted. Abovementioned analyses were then conducted within each age group. Moreover, to measure the influence of siblings’ gender and age, an interaction term was created to have children’s gender and their sibling structure multiplied together.
One question for controlling omitted household heterogeneity and contrasting children within the same household is whether household fixed or household random effect models should be adopted. The sample has a large number of households with a small number of children within each one, which means fixed effect may not be the most appropriate choice (Goldstein, 2003; Snijders and Bosker, 1999; Townsend et al., 2013). Furthermore, households that only have children of the same gender (no within-group variation) will be ignored when using fixed effect models (Bartels, 2008; Townsend et al., 2013). More importantly, fixed effect logistic model also requires within-group variation in dependent variables. This means, for example, that households lacking at least one child who has been hospitalized and at least one who has not will be dropped out due to all positive or all negative outcomes, leaving a very small valid sample for analysis. To decide which model to use, we conducted a Hausman Test to check the correlations between the independent variables and the unobserved one (Wooldridge, 2002). Fixed effect model assumes the existence of this correlation while the random one does not. A significant difference means that the hypothesis of random effect is rejected, suggesting the use of fixed effect. Most of the models in this research failed to reject the null hypothesis, which proves the appropriateness of random effect models. The only exceptions were the logistic model for testing whether sick boys are more likely than sick girls to be taken to hospitals, and the linear regression model that compares medical expenditures on sick boys and girls. For these two cases, the results of both fixed effect and random effect were analyzed.
Results
Descriptive statistics
There are a few differences between the demographic characteristics of boys and girls. As can be seen from Table 1, among all 3097 children, the mean number of children for households with at least one girl (2.6) was significantly higher than for households with at least one boy (2.5) (p < 0.001). Also, since girls were much more likely to be the elder sister, whereas boys were more likely to be the younger brother (p < 0.001), among households with at least two children, the average age of girls (7.8) in the sample was significantly higher than that of boys (7.4) (p = 0.011). Such differences can first be attributed to the one-child policy, which allows rural households to have another child if the first one is a girl. No second child is allowed, in contrast, when the first one is a boy. Moreover, even without the policy, compared with households that already have boys, due to son preference, those who have only girls are more likely to try for another child (Garg and Morduch, 1998).
Most children (78.4%) were reported to have been sick at least once in the past 12 months. And 63.9% of the sick children had visited a hospital at least once due to illness. But no significant gender difference could be found in either group. Instead, significant gender disparities only began to appear when related to hospitalization. Among the 1148 children who were taken to a hospital, 13.3% of the boys were eventually hospitalized, compared to only 8.8% of the girls (p = 0.014). Gender gaps were enlarged when all sick children were included, where boys’ chance of hospitalization was about twice as high as that for girls (p < 0.001). This then contributed to the gender disparity in medical expenditures. The mean medical expense for sick boys was about 1282 yuan, which was significantly higher (p = 0.003) than that for girls (around 817 yuan).
Whether illness was reported
Regression for households’ pattern of seeking curative healthcare for children (selected main predictors).
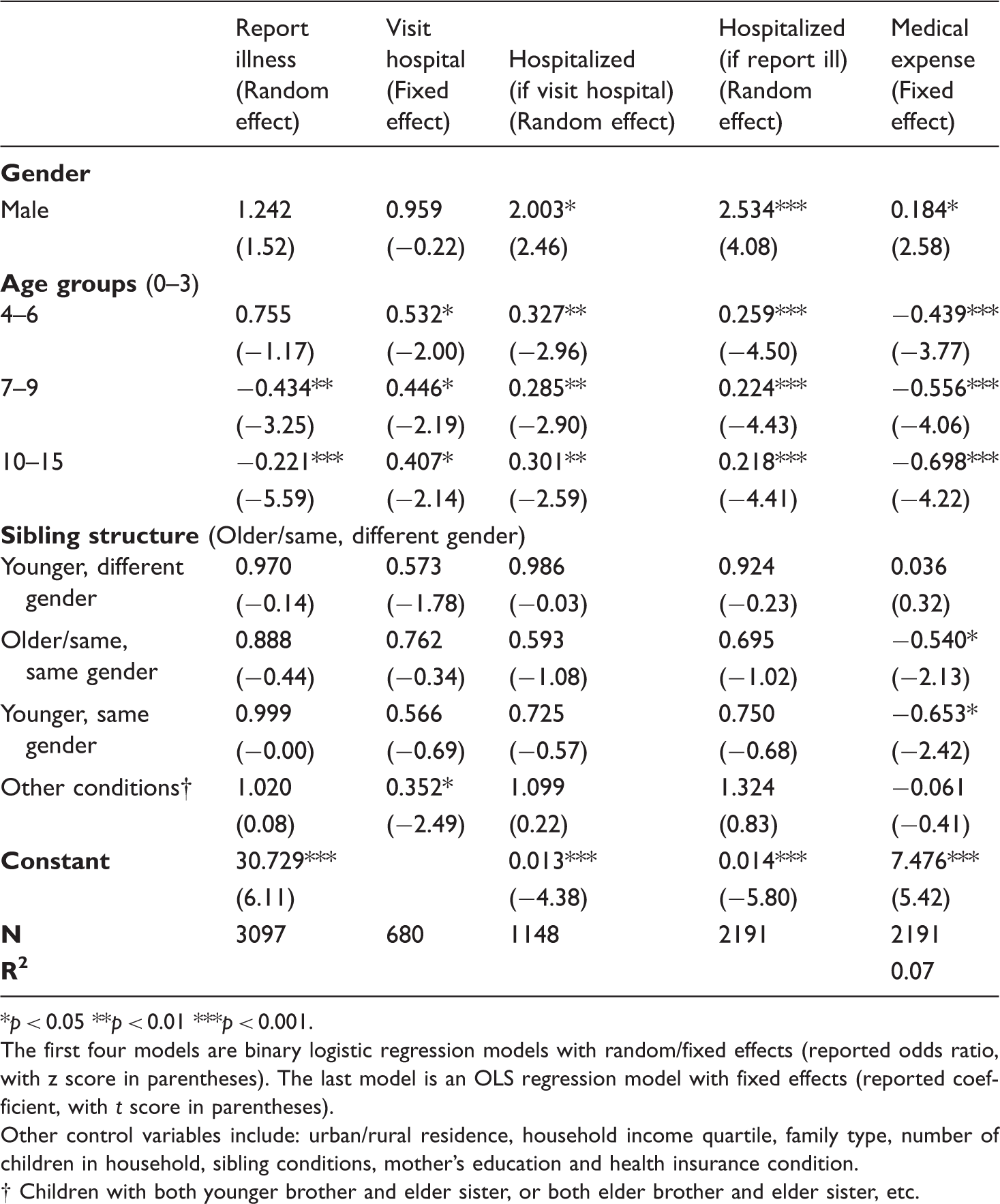
*p < 0.05 **p < 0.01 ***p < 0.001. The first four models are binary logistic regression models with random/fixed effects (reported odds ratio, with z score in parentheses). The last model is an OLS regression model with fixed effects (reported coefficient, with t score in parentheses). Other control variables include: urban/rural residence, household income quartile, family type, number of children in household, sibling conditions, mother’s education and health insurance condition.
Regression for households’ pattern of seeking curative healthcare for children (age subgroups) (selected main predictors).
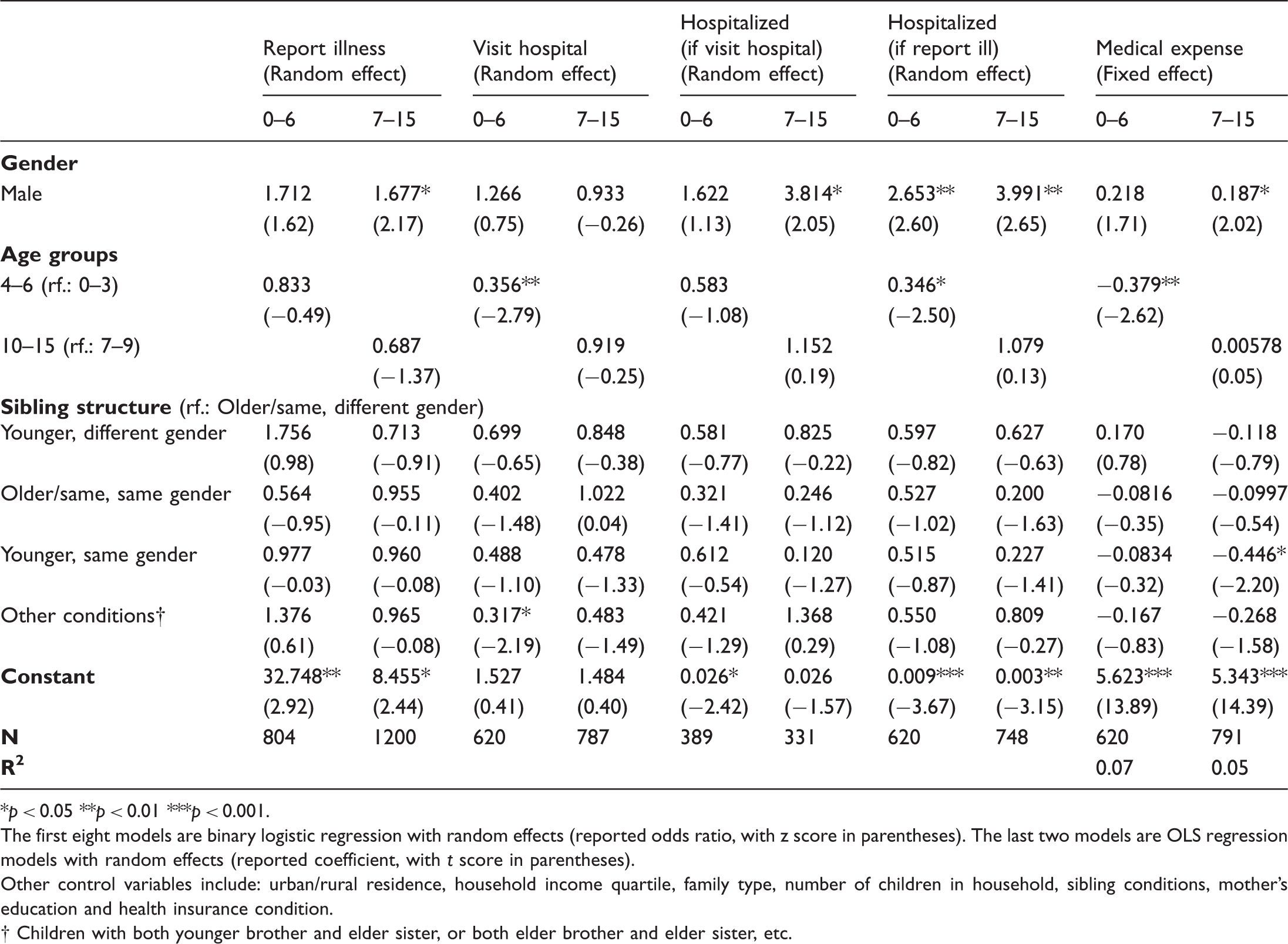
*p < 0.05 **p < 0.01 ***p < 0.001. The first eight models are binary logistic regression with random effects (reported odds ratio, with z score in parentheses). The last two models are OLS regression models with random effects (reported coefficient, with t score in parentheses). Other control variables include: urban/rural residence, household income quartile, family type, number of children in household, sibling conditions, mother’s education and health insurance condition.
Regression for sibling structure’s impact on girls’ chance of being reported ill and visiting hospital (selected main predictors).
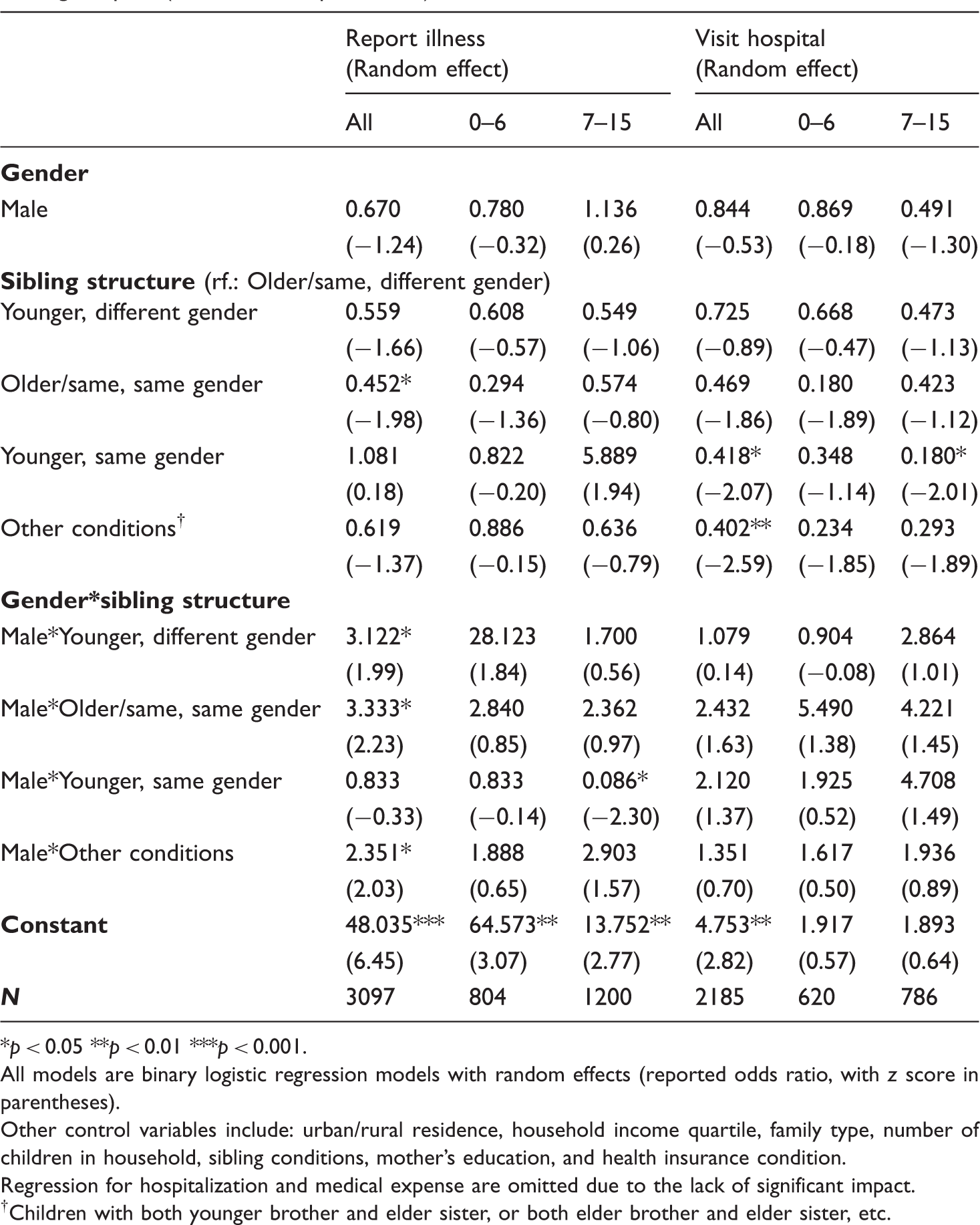
*p < 0.05 **p < 0.01 ***p < 0.001. All models are binary logistic regression models with random effects (reported odds ratio, with z score in parentheses). Other control variables include: urban/rural residence, household income quartile, family type, number of children in household, sibling conditions, mother’s education, and health insurance condition. Regression for hospitalization and medical expense are omitted due to the lack of significant impact. †Children with both younger brother and elder sister, or both elder brother and elder sister, etc.
Being taken to hospital and hospitalization
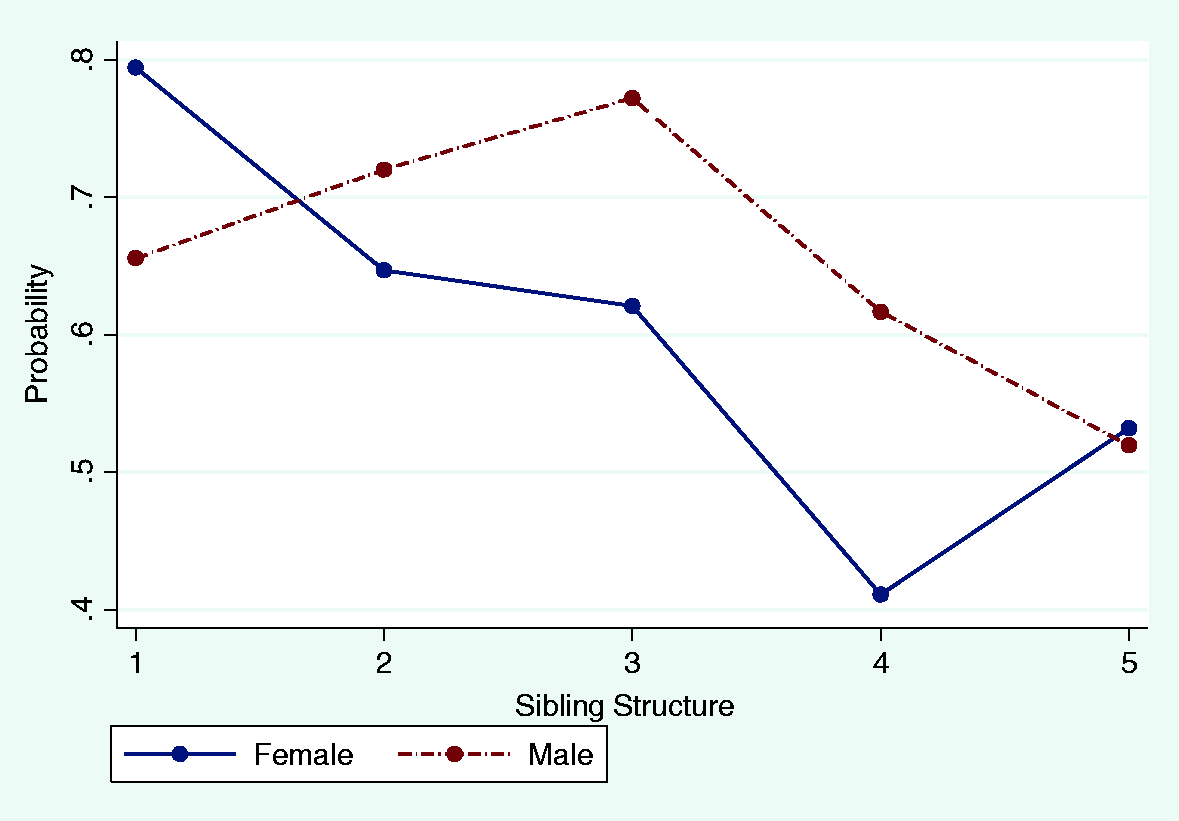
In contrast with hypothesis 2, which predicts a higher chance of sick boys being taken to hospital than sick girls, the results of both fixed effect and random effect show that after we controlled household and demographic differences, children’s gender still had no significant impact on household adults’ decisions about seeking external healthcare from hospitals for sick children (Table 2 and Appendix 3). No significant gender gaps were observed from the two separate age groups either (Table 3). Nevertheless, the odds of sick girls visiting a hospital could be influenced by the gender and age composition of their siblings; deviating from hypothesis 4, it was sick girls with younger sisters, rather than those with younger brothers, who were in a disadvantaged position (Table 4). The odds of sick girls who had only younger sisters being taken to hospital were about 58% lower than those with elderly or same-age brothers only (p = 0.039). Girls were also significantly disadvantaged (p = 0.010) when the composition of siblings was more complex (Table 4 and Figure 3). For girls between 7 and 15, the negative impact of only having younger sisters was even more severe. Their odds of visiting a hospital were about 82% lower than the odds for those who had only elder or same-age brothers (p = 0.044) (Table 4 and Figure 3).
Gender disparities became significant when hospitalization was required. Among the 1148 children who were taken to the hospital, boys’ odds of being hospitalized were about twice those of girls (p = 0.014), as was stated in hypothesis 2 (Table 3). Moreover, the hospitalization rate of children was closely related to their chance of visiting a hospital since in order to be hospitalized, children needed to be taken to a hospital by adults in the first place. When sick children who had not visited a hospital in the past 12 months were included in the analysis, gender gaps enlarged such that boys’ odds of being hospitalized were about 2.5 times those of girls (p < 0.001) (Table 3).
While it is expected that gender differences in hospitalization would shrink as children grow up, what the data showed seems to be the opposite. For sick children aged 7–15 who were taken to hospital at first, boys’ odds of being hospitalized were about 2.8 times higher than those girls (p = 0.041), whereas for those under 6, no significant gender disparity existed. Besides, while gender differences could be observed among both younger (0–6) and older (7–15) children when all the sick children were included, the gap was larger for the latter group. Boys’ odds of hospitalization were about 1.7 times higher than those for girls (p = 0.009) among sick children under 6, but about three times higher when measured for those between 7 and 15 (p = 0.008). However, unlike with visiting a hospital, the gender and age of siblings no longer had any significant influence on the odds of hospitalization for either boys or girls.
Medical expenditure
Utilizing different kinds of healthcare, the medical expenditures on sick boys and girls also varied. Being a boy was associated with about 20% higher medical expenditure in both fixed [exp(0.184) = 1.20, p = 0.004] and random [exp(0.183) = 1.20, p = 0.010] effects models. Such differences could mainly be explained by the different probabilities of hospitalization. When we excluded children who were hospitalized, significant gender differences on medical expenses no longer existed (not reported). Again, in contrast with hypothesis 3, no significant gender disparities could be found among sick children under age 6. But for children between ages 7 and 15, boys’ medical expense was about 21% higher [exp(0.187) = 1.21, p = 0.043] (Table 3). Also, having siblings of different ages and genders did not have any significant impact on the medical expenditures of boys and girls.
Discussion
With the aim of checking children’s well-being and the severity of son preference, researchers have studied the gendered nature of households’ healthcare-seeking behavior for children in several developing countries. While the advantages for boys are obvious in general, detailed conditions in each country and area vary. Attempting to understand how households’ healthcare-seeking behaviors for children are determined by children’s genders and at which stage of decision-making the influence of gender begins to appear, this research first found that rural Chinese households generally pay more attention to and allocate more household resources on the physical well-being of male children. Thus, along with affecting prenatal sex selection and preventive healthcare, son preference also impairs Chinese girls’ utilization of medical treatments.
However, the inferior position of girls does not seem to persist throughout the whole process of decision-making. While household adults’ neglect or concealment of girls’ illnesses has been considered a severe problem in many countries and areas, there is no evidence sufficient to prove that such a phenomenon exists in rural China. Indeed, boys are significantly more likely to be reported ill than girls in certain age groups and for certain kinds of illnesses. But this may be caused by household adults’ preference for boys, as well as young girls’ advantages in resisting illness. The excess mortality of male infants in the neonatal period, which is caused by male infants’ naturally weaker immune systems, is a widely observed and consistent phenomenon (Anker, 2007; Waldron, 1983). Since this research’s report, coding and categorization of illnesses are far from professional and accurate, it is hard to know children’s actual health conditions. Arguing that household adults care more about boys’ health simply because boys have a higher chance of being reported ill is, therefore, arbitrary.
For children who have been reported ill, a significant gender difference does not appear in visiting hospitals, but only emerges when the decision about hospitalization must be made. Consistent with the aforementioned research conducted at Chinese hospitals, the hospitalization rate of boys exceeds that of girls significantly. In other words, girls have a higher probability of being treated unsuitably when the symptoms of illness are severe enough that hospitalization is required. It cannot be denied that whether sick children need to be hospitalized depends heavily on healthcare providers’ diagnoses, but doctors’ advice may not always be followed. It is still the household adults who make the final decision on hospitalization. Moreover, no matter how severe the illness may be, children cannot be hospitalized unless household adults take them to the hospital first. Compared with sick children who have visited a hospital, gender gaps in hospitalization increase when those who never seek external medical care are taken into consideration. As a result, although gender difference is not significant in visiting a hospital, it contributes to the significant gender disparity in the hospitalization of children. Since hospitalization is much more expensive than simply visiting a hospital, it is not surprising that medical expenditure for boys is significantly higher than that for girls.
It is assumed that gendered healthcare-seeking behaviors for children may steadily disappear as children grow up. However, the results of this research show that in term of hospitalization and medical expenditure, gender disparities tend to be especially severe among children between 7 and 15. One possible explanation is that since young children are more vulnerable and their illnesses are more likely to become severe and even fatal, caregivers generally pay more attention to their health conditions and are more cautious about their medical treatment. Some studies insist that female infanticide and life-threatening discrimination against girls, a persistent problem in Chinese history, is still prevalent in the current society (Cao et al., 1997, 2013; Das Gupta and Li, 1999; Han and Li, 1999). Others find that prenatal sex-selection has, to some extent, increased young girls’ survival rate (Coale and Banister, 1994; Goodkind, 1996; Zeng et al., 1993). The results of this research seem to be consistent with the latter argument. Caregivers deliberately ignoring young girls’ illnesses and intentionally killing them through refusing medical treatment may no longer be as widespread a problem as it used to be. After all, when sex-selection abortion becomes available, already delivered female infants may have a higher chance of being treated equally with boys. On the contrary, as children grow older and their immunity improves, non-fatal illnesses may receive less attention from adults, and some medical treatments may no longer be considered necessary. The impacts of son preference then become more apparent. Because of their desire to continue family lineages and anticipation of higher returns from boys, caregivers may invest more in the health of boys than that of girls.
Furthermore, the parenting styles of Chinese parents are relatively authoritarian (Chao and Akira, 2008; Gershoff et al., 2012), which means there is no guarantee that an increase in age will directly bring children more autonomy over their own health. On the contrary, adolescents may still rely heavily on caregivers for healthcare utilization, which prolongs the influence of adults’ son preferences. Moreover, Chinese women tend to receive less medical treatment than men regardless of age. Empirical studies in developed countries usually find that women report worse health conditions and more healthcare use than men do (Nathanson, 1977; Vergrubbe, 1985; Wingard et al., 1989). But conditions in developing countries like China and India, although less well-studied, are much more complex. On the one hand, some studies find that older women report worse health conditions (Anson and Sun, 2002). Adult women’s frequency of using healthcare services is also higher in some areas (Fan et al., 2013; Gao and Yao, 2006). But on the other hand, detailed analyses have found that women use more outpatient and less qualified healthcare than men. Men spend significantly more time and money on hospitalization (Luo et al., 2009; Song and Bian, 2014; Wang et al., 2008). As a result, Chinese women’s disadvantaged position in curative healthcare utilization may be neither an exclusive problem for a specific age group, nor a simple matter of autonomy.
In addition to the overall lower hospitalization rate and medical expenses, girls also face an added problem of sibling rivalry. The gender and age of siblings have no significant impact on the level of medical treatment that boys can receive. But girls’ chances of visiting a hospital decrease significantly if they have only younger sisters. This result is partially consistent with some of the literature that is mentioned above. The enforcement of the one-child policy has given Chinese households with son preferences a sense of urgency to have at least one boy within the limited chances of reproduction. This may intensify the neglect of girls’ health when the second or third birth is still a girl. However, it is not the younger girls who are especially disadvantaged. Instead, in line with our other findings, younger children tend to receive more medical care regardless of their gender. It is the older girls who have higher risks of receiving inappropriate treatment when their families are awaiting the birth of a boy. Families that already have at least one boy, in contrast, may feel more satisfied about the sex composition of the children, and hence pay more attention to the well-being of their children. And both boys and girls can benefit from that.
Since the severity of illnesses is not entirely controlled in our models, we cannot rule out the possibility that boys’ higher hospitalization rate and higher expenditures on their medical care are the results of their biological disadvantages in the neonatal period. However, the above analyses show that boys’ hospitalization rates can be about 60% to 75% higher than those of girls. Expenditures on their medical care are also about 20% higher. It is impossible to attribute these huge differences exclusively to boys’ vulnerability. The preference for sons must have played a very important role. Furthermore, girls’ biological advantages steadily decline after birth (Anker, 2007). But according to our results, gender gaps exist mainly among children aged 7 to 15, rather than among those under 6 years old, which further confirms the existence of son preference in children’s healthcare utilization. Moreover, the fact that sibling rivalry only influences the medical care that girls can receive also proves that sick boys are more advantaged in households’ allocation of medical resources.
Son preference has shaped the sex structure of Chinese households, as well as households’ attitudes to girls’ health. Besides the high sex-ratio at birth and girls’ inferior position in nutrition intake and preventive healthcare utilization, this research found that in rural China, the discrimination against girls also exists in households’ allocation of curative healthcare to sick children. Compared with boys, girls are less likely to receive proper medical treatments, especially when hospitalization is required. Such disadvantages become even more apparent as they grow older or only have younger siblings of the same gender. Insufficient curative healthcare may have short-term and long-term impacts on girls’ health, and even contribute to their high mortality rate. Panel studies can be conducted to test these correlations in the future. Future studies may also focus on the healthcare utilization practices of adults in different age groups to see to what extent the disadvantages of female persist.
This research has several limitations. First, as mentioned above, it relies on household adults’ reports of children’s illnesses, and the severity of illness cannot be coded accurately, which makes it hard to measure the real health conditions of children and household adults’ perceptions of children’s illnesses. Second, the whole analysis relies on the relation between the most severe illness the child had and the medical treatment they received in the past 12 months. The most severe illnesses usually receive more attention from adults than other minor illnesses, and hence can, to a large extent, be considered representative. However, the research results can be more accurate if the medical treatments that children receive for each illness can be recorded separately.
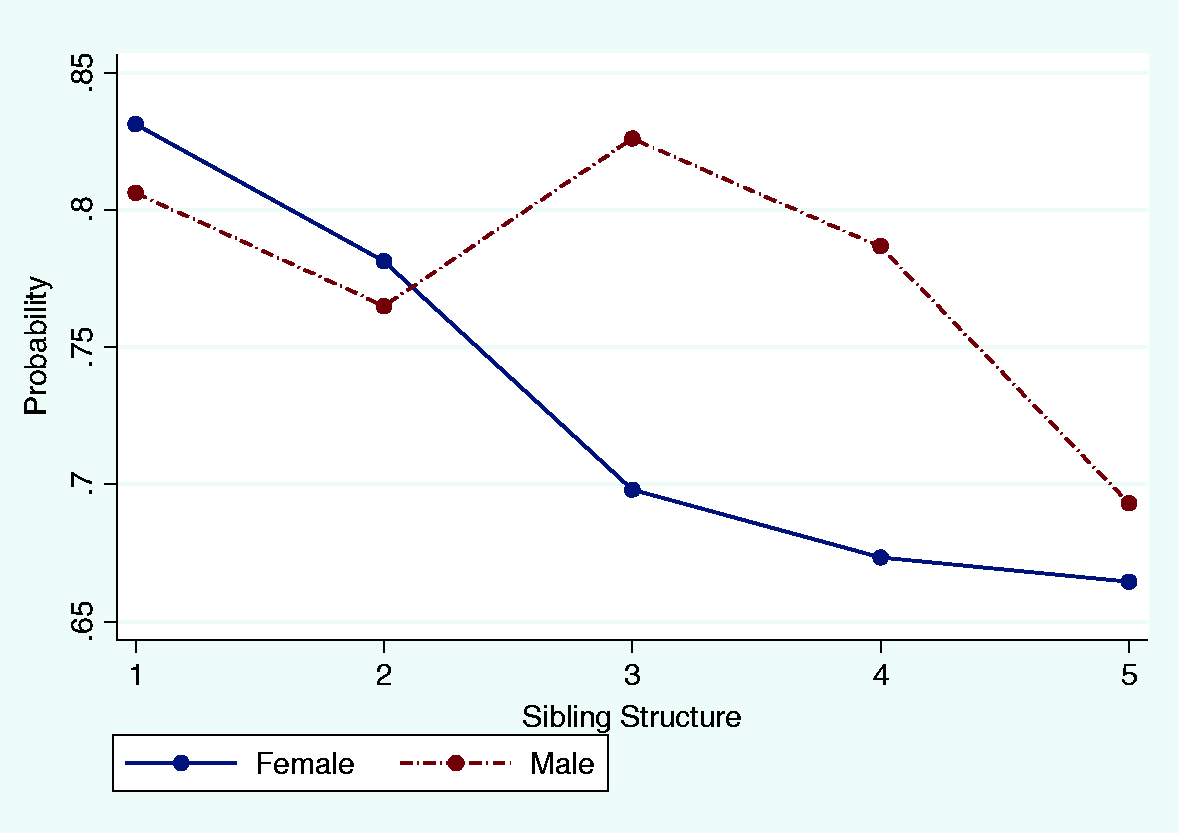
Predicted probabilities of being reported ill (0–15). Predicted probabilities of being taken to hospital (0–15). Predicted probabilities of being taken to hospital (7–15).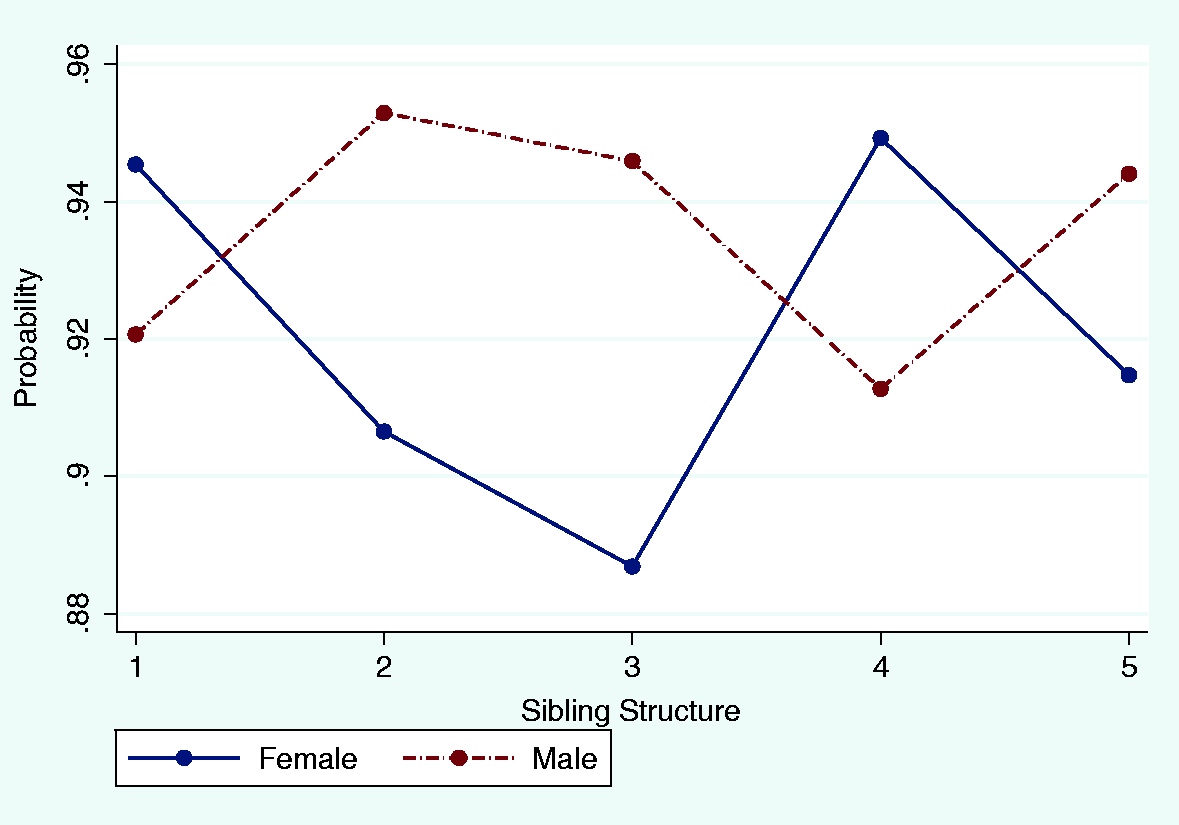
Footnotes
Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
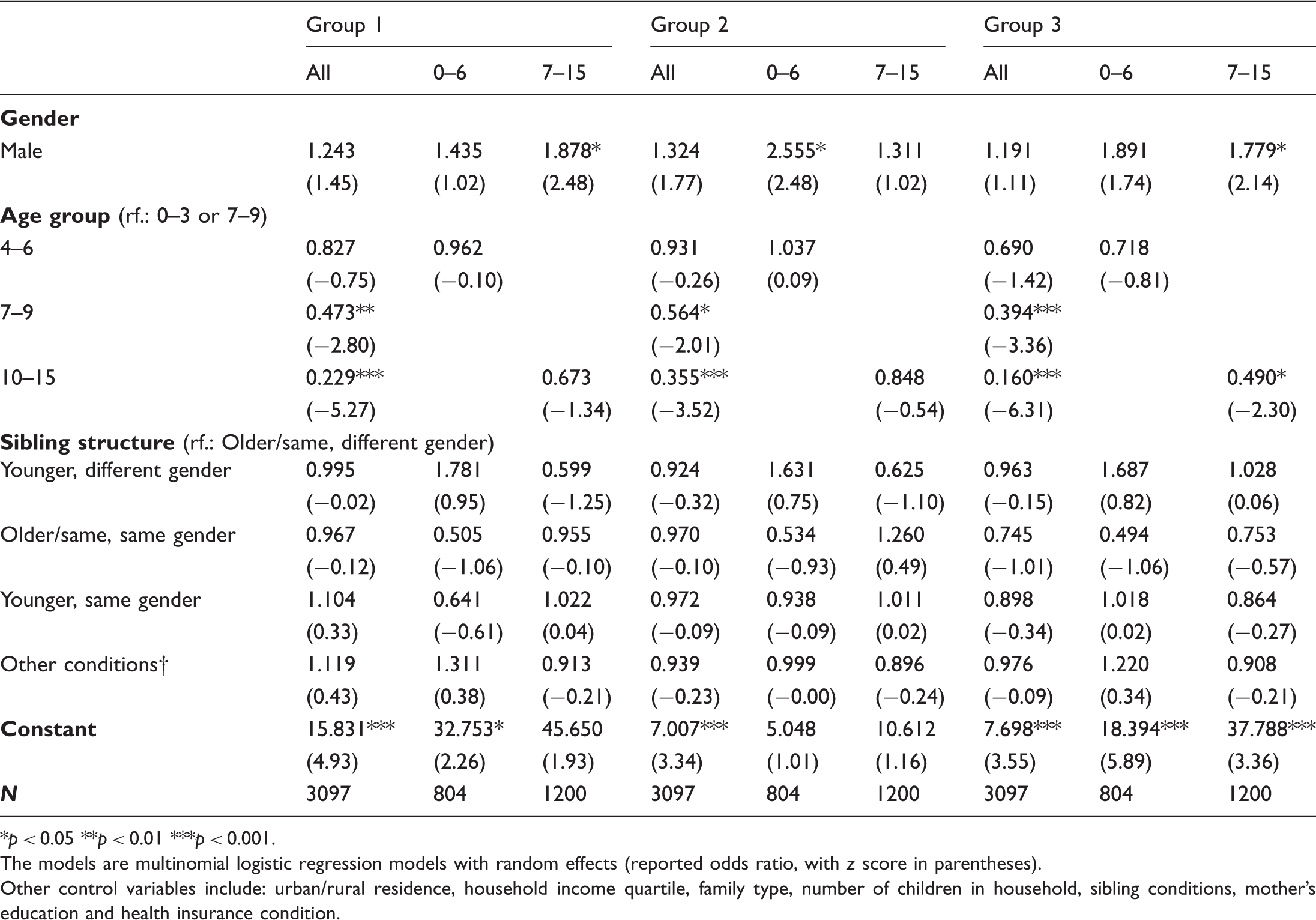
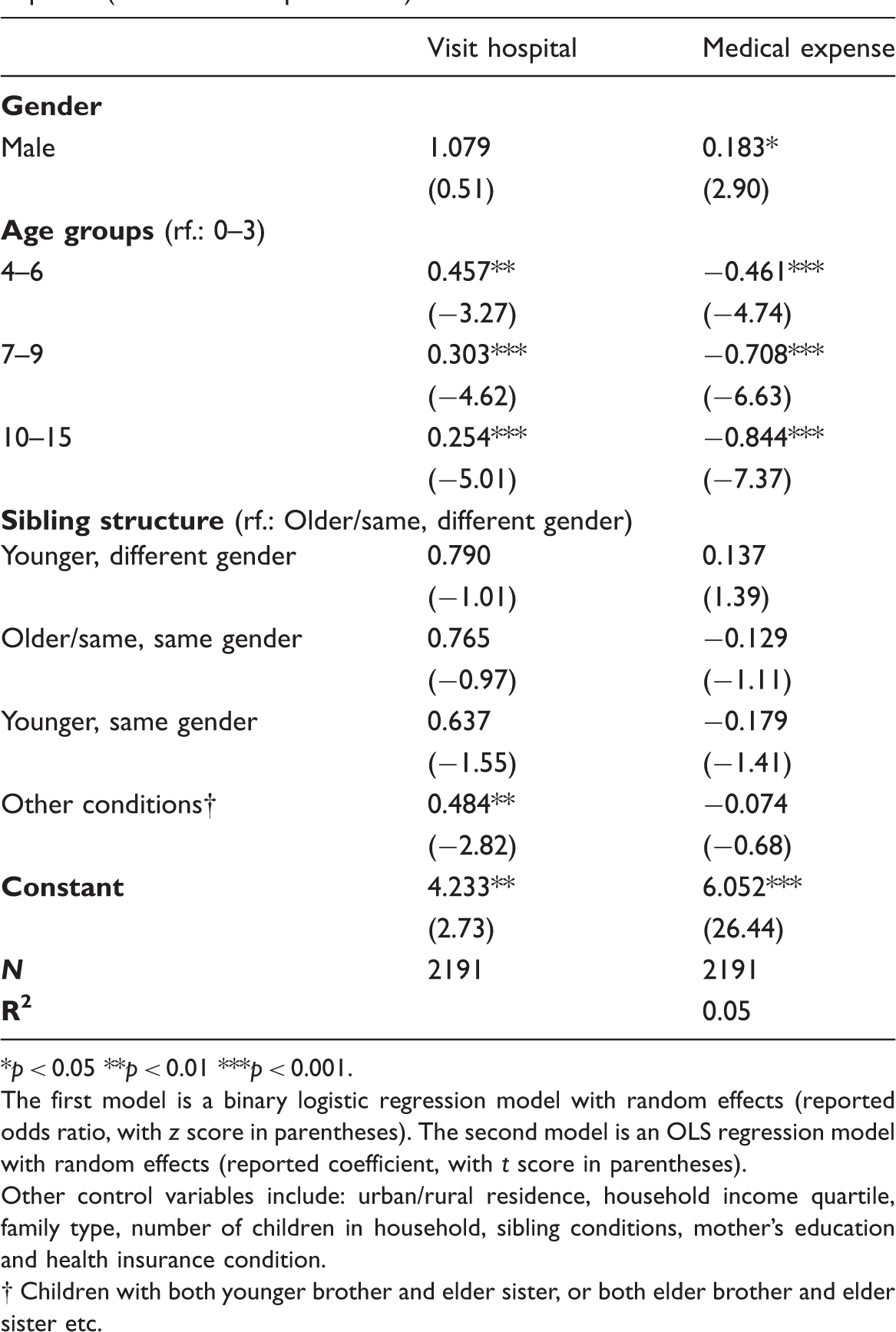
Group of illness. Regression for parent’s report of children’s illness (illness subgroups). *p < 0.05 **p < 0.01 ***p < 0.001. The models are multinomial logistic regression models with random effects (reported odds ratio, with z score in parentheses). Other control variables include: urban/rural residence, household income quartile, family type, number of children in household, sibling conditions, mother’s education and health insurance condition. Random effect models for hospital visiting and medical expense (selected main predictors). *p < 0.05 **p < 0.01 ***p < 0.001. The first model is a binary logistic regression model with random effects (reported odds ratio, with z score in parentheses). The second model is an OLS regression model with random effects (reported coefficient, with t score in parentheses). Other control variables include: urban/rural residence, household income quartile, family type, number of children in household, sibling conditions, mother’s education and health insurance condition. 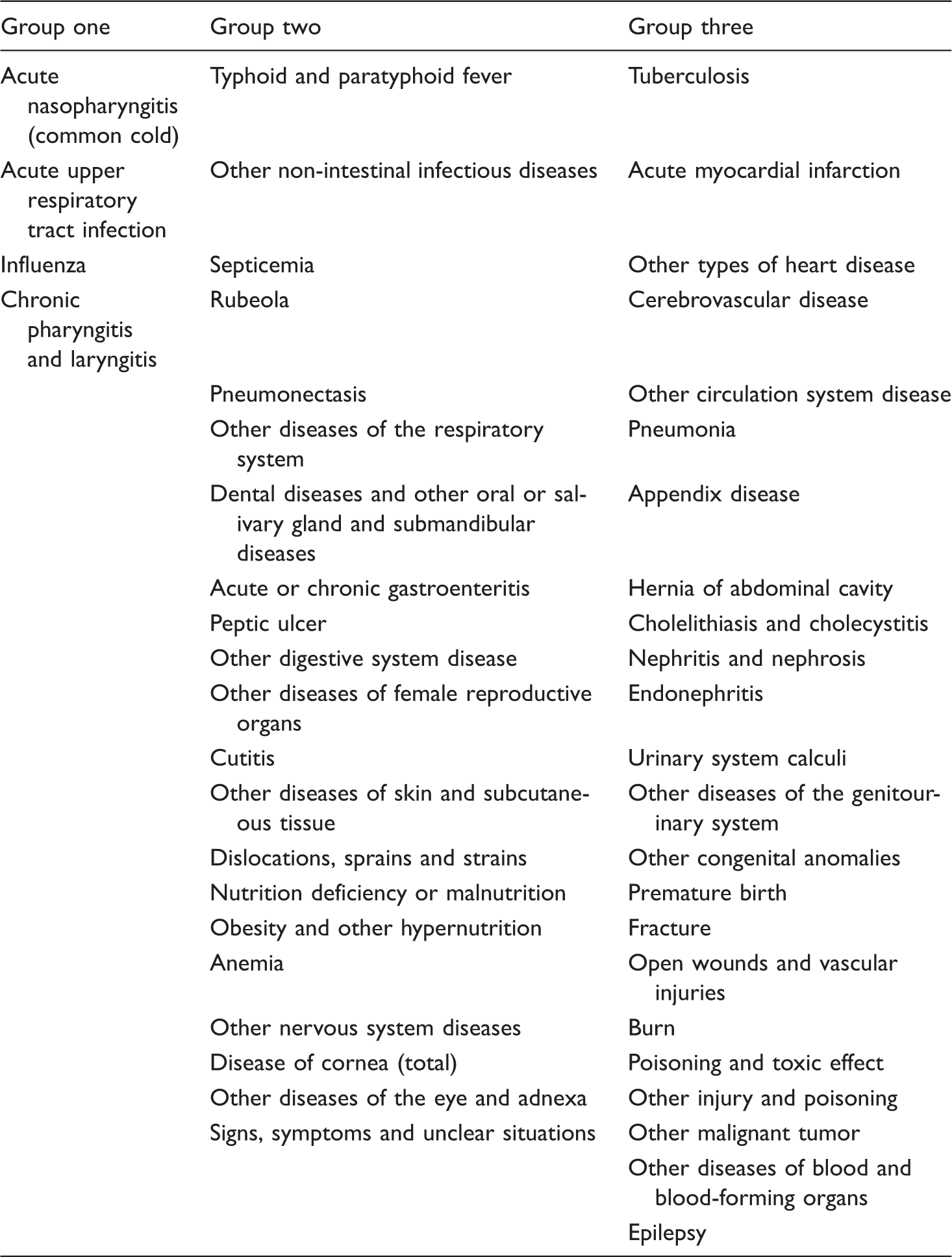
Group one
Group two
Group three
Acute nasopharyngitis (common cold)
Typhoid and paratyphoid fever
Tuberculosis
Acute upper respiratory tract infection
Other non-intestinal infectious diseases
Acute myocardial infarction
Influenza
Septicemia
Other types of heart disease
Chronic pharyngitis and laryngitis
Rubeola
Cerebrovascular disease
Pneumonectasis
Other circulation system disease
Other diseases of the respiratory system
Pneumonia
Dental diseases and other oral or salivary gland and submandibular diseases
Appendix disease
Acute or chronic gastroenteritis
Hernia of abdominal cavity
Peptic ulcer
Cholelithiasis and cholecystitis
Other digestive system disease
Nephritis and nephrosis
Other diseases of female reproductive organs
Endonephritis
Cutitis
Urinary system calculi
Other diseases of skin and subcutaneous tissue
Other diseases of the genitourinary system
Dislocations, sprains and strains
Other congenital anomalies
Nutrition deficiency or malnutrition
Premature birth
Obesity and other hypernutrition
Fracture
Anemia
Open wounds and vascular injuries
Other nervous system diseases
Burn
Disease of cornea (total)
Poisoning and toxic effect
Other diseases of the eye and adnexa
Other injury and poisoning
Signs, symptoms and unclear situations
Other malignant tumor
Other diseases of blood and blood-forming organs
Epilepsy
Group 1
Group 2
Group 3
All
0–6
7–15
All
0–6
7–15
All
0–6
7–15
Male
1.243
1.435
1.878*
1.324
2.555*
1.311
1.191
1.891
1.779*
(1.45)
(1.02)
(2.48)
(1.77)
(2.48)
(1.02)
(1.11)
(1.74)
(2.14)
4–6
0.827
0.962
0.931
1.037
0.690
0.718
(−0.75)
(−0.10)
(−0.26)
(0.09)
(−1.42)
(−0.81)
7–9
0.473**
0.564*
0.394***
(−2.80)
(−2.01)
(−3.36)
10–15
0.229***
0.673
0.355***
0.848
0.160***
0.490*
(−5.27)
(−1.34)
(−3.52)
(−0.54)
(−6.31)
(−2.30)
Younger, different gender
0.995
1.781
0.599
0.924
1.631
0.625
0.963
1.687
1.028
(−0.02)
(0.95)
(−1.25)
(−0.32)
(0.75)
(−1.10)
(−0.15)
(0.82)
(0.06)
Older/same, same gender
0.967
0.505
0.955
0.970
0.534
1.260
0.745
0.494
0.753
(−0.12)
(−1.06)
(−0.10)
(−0.10)
(−0.93)
(0.49)
(−1.01)
(−1.06)
(−0.57)
Younger, same gender
1.104
0.641
1.022
0.972
0.938
1.011
0.898
1.018
0.864
(0.33)
(−0.61)
(0.04)
(−0.09)
(−0.09)
(0.02)
(−0.34)
(0.02)
(−0.27)
Other conditions†
1.119
1.311
0.913
0.939
0.999
0.896
0.976
1.220
0.908
(0.43)
(0.38)
(−0.21)
(−0.23)
(−0.00)
(−0.24)
(−0.09)
(0.34)
(−0.21)
15.831***
32.753*
45.650
7.007***
5.048
10.612
7.698***
18.394***
37.788***
(4.93)
(2.26)
(1.93)
(3.34)
(1.01)
(1.16)
(3.55)
(5.89)
(3.36)
3097
804
1200
3097
804
1200
3097
804
1200
Visit hospital
Medical expense
Male
1.079
0.183*
(0.51)
(2.90)
4–6
0.457**
−0.461***
(−3.27)
(−4.74)
7–9
0.303***
−0.708***
(−4.62)
(−6.63)
10–15
0.254***
−0.844***
(−5.01)
(−7.37)
Younger, different gender
0.790
0.137
(−1.01)
(1.39)
Older/same, same gender
0.765
−0.129
(−0.97)
(−1.11)
Younger, same gender
0.637
−0.179
(−1.55)
(−1.41)
Other conditions†
0.484**
−0.074
(−2.82)
(−0.68)
4.233**
6.052***
(2.73)
(26.44)
2191
2191
0.05