
Abstract
Background and Aim
The study investigated the present state of awareness, unmet needs, and barriers faced by participants using wheelchairs in a tertiary care hospital in India.
Methods
This sequential explanatory mixed-method study explored the participants’ experiences in two parts. Part one presents the result analysis of user experience and wheelchair service provision using rATA (n=100). Part two presents a thematic analysis of 100 in-depth semi-structured interviews.
Result
The study and interviews define barriers to wheelchair access provision, including assessment, prescription, customization, training, wheelchair maintenance, and follow-up. The study reported that most participants procured their wheelchairs from the private sector (35%) while 10% received them from the public sector. The main reasons for not having the appropriate wheelchair were affordability (78%), lack of support (64%), and lack of awareness (41%), while road/transport accessibility (63%) and home accessibility (53%) were the main obstacles for the wheelchair non-use.
Conclusion
The study provided insights into wheelchair provision and user satisfaction within healthcare delivery system. Integration of Wheelchair service and delivery into the health care system can strengthen the rehabilitation health system per the WHO guidelines.
Introduction
Disability is a global health issue as per the World Bank and WHO assessment because “people with disabilities deal with numerous challenges in receiving health-related services, such as rehabilitation, and have poor health outcomes as compared to the persons who are not disabled”.1,2 According to the estimate, approximately one billion people, or 15% of the global population, are disabled 3 whereas 26.8 million, or 2.21% (Census 2011), in India, are differently abled. Over 10 years, the number of people in India who are differently abled has increased, from 21.9 million in 2001 to 26.8 million.4,5
People with a disability require assistive products to improve mobility, 6 physical health, and overall quality of life.6–9 As per the WHO, only one in 10 people who require Assistive Technology (AT) 10 have access to it1,11 and it is growing exponentially.12–14 The wheelchair is one type of assistive equipment in high demand but low supply. Worldwide, 75 million people require a wheelchair at present1,5 out of which 2%–5% have access in low- and middle-income nations. The lack of adequate wheelchairs leads to mobility impairment and participation limitation, impacting education and overall quality of life. 15
Provision guidelines for wheelchairs as per WHO recommended eight steps that may be carried out in some wheelchair services, which include referral and appointment; assessment, prescription, funding and ordering, product preparation, fitting, user training, maintenance, repairs, and follow-up. 10 A study by Gowran RJ et al. (2018) suggests that wheelchair supply, demand, availability, and necessity are necessary when accessing an appropriate wheelchair. 8
A study by Dwivedi A et al. (2019) concluded that AT users faced barriers related to its availability, awareness, psychological, and financial, whereas persons already using AT faced repair and maintenance, accessibility, and psychological barriers in addition to the barriers encountered by the first-time users, 9 highlighting the need to expand present technology.
Mhatre A, Rosen et al. (2007) observed a lack of regulations, funding, and awareness of the provision of inappropriate AT models through various procurement channels that impact the quality of the wheelchair. 12 Gallagher A. et al. (2020) concluded in their study that wheelchair and seating provision systems are influenced by interactions between wheelchair, supply, environment, personnel, user-centered, and organizational factors. 13
The Indian government has determined mobility devices to be essential for mobility14,16 for which the government has started the Assistance to Disabled Persons (ADIP) program14,16 and formed the Artificial Limbs Manufacturing Corporation of India (ALIMCO).14,16 Only 20% of people with impairments are advised of the AT, out of which only 16% have access. According to the current data only 25% have obtained their device via a government program, whereas nearly two-thirds have purchased it.16,17
Despite the essential role of assistive technology in enhancing the quality of life for people with mobility impairments, there’s a lack of evidence on wheelchair accessibility and user needs in resource- constrained environments in the Indian scenario. Existing research often overlooks broader aspects of participation and inclusion.
This study investigates the factors affecting wheelchair knowledge and accessibility issues among wheelchair users in India. It provides valuable insights into the current state of wheelchair services and recommendations for enhancing accessibility and unmet needs for informing policymakers, healthcare providers, and disability advocates about the necessary steps to improve the inclusivity and quality of life for wheelchair users in resource-limited settings. The study is based on the WHO’s 8-Step Wheelchair Provision Model, which outlines referral, assessment, prescription, funding, product preparation, fitting, user training, maintenance, and follow-up. This framework includes both the quantitative and qualitative components of the study.
Methods
The research explored the experiences, user needs, and wheelchair provision among wheelchair users in hospital settings. For this, a two-part mixed-method study was conducted. Part one presents the results (n = 100) of survey data using rATA from wheelchair user respondents of wheelchair needs and challenges in accessing service provision. The questionnaire was modified: “assistive product” and “product” were replaced by “wheelchair” to make it study-specific.
Part two presents a thematic analysis of qualitative in-depth semi-structured interviews of wheelchair users with experience related to service provision. The qualitative research design was selected to offer a client-centered approach based on the limitations of the rATA. The results were reported later for the analysis.
Sample
For parts 1 and 2, convenience sampling was used to recruit 100 interview participants meeting the following criteria: individuals of age 18 and above who are using a wheelchair, individuals of age 18 and above who have been advised the wheelchair from hospital but may not be using due to any reason, guardians of children below 18 years of age who are using or have been advised for a wheelchair, individuals who need wheelchair due to disability or owns a wheelchair due to disability, Individuals who do not have their own wheelchair, relevant caregivers of elderly persons or persons with disability involved in their care. Subjects who are unable to communicate in either English or Hindi, unable to understand the questions, critically ill, and who require it temporarily were excluded from the study. Convenience sampling was adopted due to logistical feasibility within a tertiary hospital setup. However, this may have led to selection bias as participants who regularly visited the hospital or were more accessible were more likely to be included.
The quantitative sample size (n = 100) was based on feasibility and aligns with previous wheelchair accessibility studies in similar tertiary settings, providing adequate variability for descriptive and exploratory analysis. For the qualitative interviews, recruitment continued until thematic saturation was reached, defined as the point at which no new codes or themes emerged (after approximately 90 interviews).
Data collection and analysis
The numeric data in part 1 from closed questions were completed using Statistical Package for Social Sciences (SPSS) version 25 for Windows and the Excel Sheet. For part two, a self-constructed interview guide was used to conduct semi-structured interviews consisting of open-ended questions. The interview was scheduled for each participant and lasted 30 to 45 minutes. The results were qualitatively analyzed, and thematic analysis was used as a process to identify the themes from the interpretation of the participants’ experiences. The statistical analysis involved descriptive analysis of the gathered data.
Survey design
The survey was developed and modified in two parts to ensure its relevance to the target population. This study followed a sequential explanatory mixed-methods design, where the quantitative survey (Part 1) informed the qualitative interviews (Part 2). The qualitative phase was used to explain and elaborate on findings from the quantitative analysis. Different participants were included in each phase, although they represented the same population group attending the tertiary hospital in India. The study employed a mixed-methods approach, comprising 12 closed questions with opportunities for open comments, structured around wheelchair awareness and user-unmet needs. Survey questions focused on participants’ experiences and perspectives related to the WHO’s eight steps for wheelchair provision. The data was collected in person in pen and paper format.
Ethical consideration
Ethical approval was granted by the Institute's Ethics Committee (IEC-649/06.10.2023). Interview participants provided written consent before participating in this study and were informed that their consent could be withdrawn. Study information was listed at the beginning of the survey to outline the study’s purpose. All the data was collected, data confidentiality was maintained, and the data were stored securely and protected. Additional measures were taken to protect vulnerable participants, including obtaining consent from caregivers of minors and ensuring voluntary participation without coercion. Interviews were conducted privately to maintain confidentiality and minimize distress.
Results
Demographic and descriptive information
Demographic and clinical characteristics of the study participants (N = 100).

92% of the surveyed participants (n = 100) were not employed, 3% (n = 100) did part-time (less than 40 h/week), and 4% (n = 100) were full-time employed (more than 40 h/week) (as in Table 1). Of wheelchair users, 91% (n = 100) were manual wheelchair users, and 1% (n = 100) were motorized users. Also, 3% (n = 100) used customized/other types of wheelchairs as compared to the standardized wheelchair users. (as in Table 1).
The duration of wheelchair use differs from individual to individual. Based on the data it was found that 5% (n = 100) used the wheelchair for less than 30 min, 7% used it between 30 min and 1 h, 11% (n = 100) used the wheelchair for the duration between 1 h and 2 h, 72% (n = 100) used it for more than 2 h (Table 1).
The data represented the current educational status among the participants, with a vast majority not engaged in education (85%). This might suggest barriers to accessing education, possibly due to socioeconomic limitations, health issues, or lack of educational facilities. The low percentage of participants pursuing education (15%) highlights the need for targeted interventions to increase access to and support for education.18–22
Among the total respondents, it was found that 21% (n = 100) were independent, while 31% (n = 100) required assistance in wheelchair transfer, and 47% needed to be lifted (fully dependent) in wheelchair transfer (as in Table 1). Wheelchair use also varied from individual to individual. 58% used a wheelchair for outdoor mobility, and 42% often required a wheelchair for both indoor and outdoor mobility. None of the individuals reported using the wheelchair only for indoor mobility, due to the small space for wheelchair propulsion at home (as in Table 1).
Part 1
Data collection tools
Part one presents the standardized tool WHO rapid Assistive Technology Assessment (rATA) scales used to record the subject’s responses.
rATA
rATA analysis report.
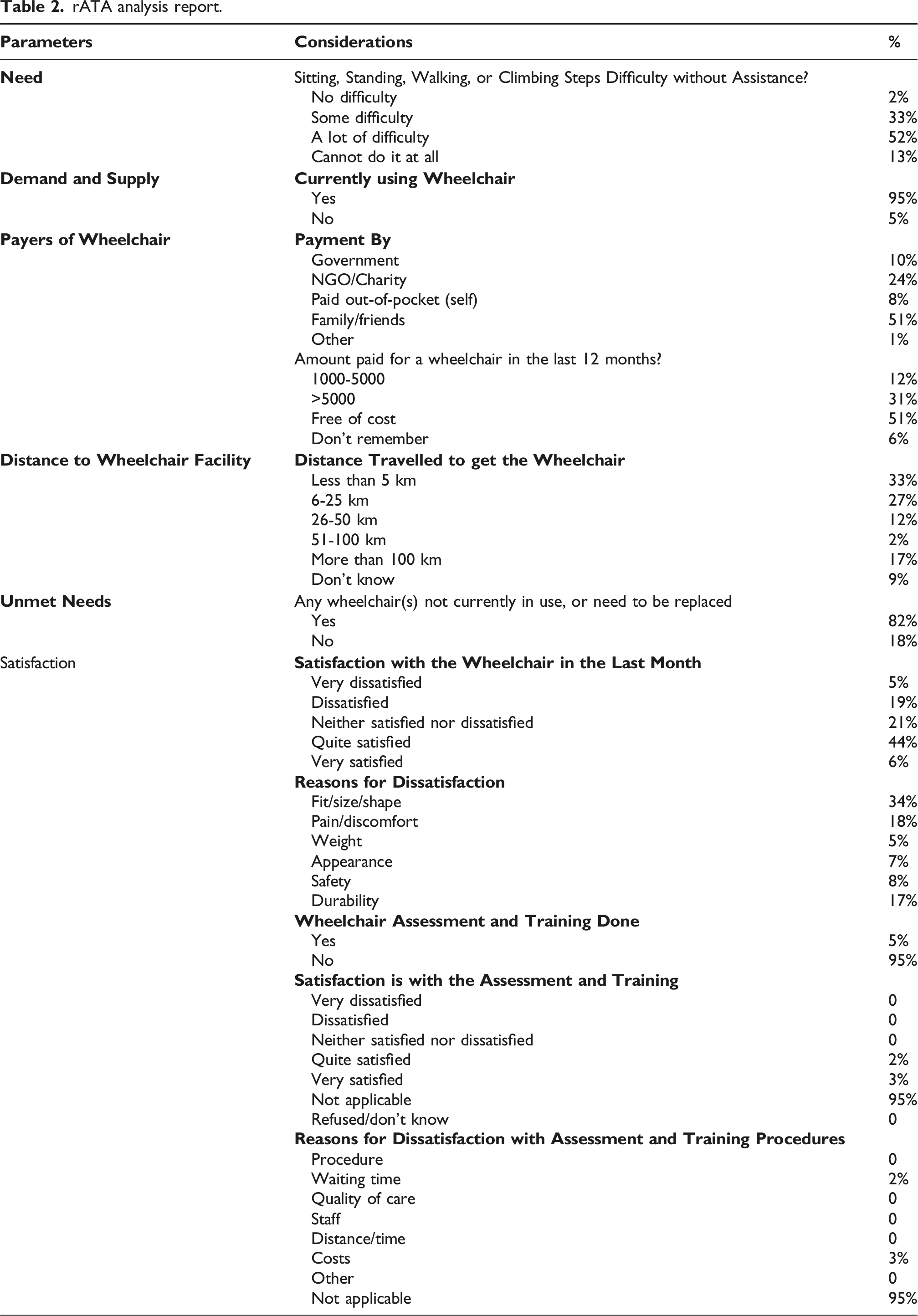
The study revealed that 33% of wheelchair user had to travel less than 5 km, 27% travelled 6-25 km, 12% travelled 26-50 km, 2% travelled 51-100 km and 17% had to travel for more than 100 km to obtain their wheelchair (Table 2).
About 50% of respondents are satisfied or very satisfied with wheelchairs, a significant 24% of the participants were dissatisfied. Fit/size/shape (34%), pain/discomfort (18%), and durability (17%) were the main reasons for dissatisfaction. In addition, 5% of participants reported having undergone wheelchair assessment and training (Table 2).
The majority of the participants procured their wheelchairs from the private sector (35%) followed by 26% procuring their wheelchairs from friends/family. The public sector and NGO account for about 10% and 23% respectively of the wheelchair source (Table 2). The distribution showed different channels from where wheelchairs were obtained, with public and NGO support being the largest wheelchair provider, followed by private and personal sources (Figure 1). Wheelchair source.
Amount paid by the user varied with half of the informants receiving it free of cost, 31% paying more than Rs 5000, and 12% paying between Rs 1000-5000. A small proportion of the participants did not remember the amount paid by them to buy their wheelchairs. 24% were donated by NGOs, and 8% paid out of their pocket. (Table 2).
The respondents claim financial constraints as a major barrier to not having an appropriate wheelchair, with 78 unable to afford it. 64 reported a lack of support, and 41 didn’t know where to procure a wheelchair. Other barriers included lack of time (n = 12), lack of transport (n = 9), unsuitability of available wheelchairs (n = 4), and unavailability (n = 5) (Figure 2). Reasons for not having the wheelchair and not using the wheelchair.
Several reasons were identified for not using the wheelchair despite having it. Among the 100 surveyed participants, 63 reported road and transport difficulties as the major challenge faced followed by work and school accessibility by 53 participants. Additionally, 36 reported fit, size, or shape issues. Safety concerns were noted by 15 participants while 7 mentioned the weight of the wheelchair as the major concern and 7, highlighted experiencing negative attitudes from others. (Figure 2).
The degree of satisfaction with wheelchair accessibility showed 35.35% of respondents were completely dissatisfied with the accessibility of their home and surroundings, 21% thought it was moderately accessible, and 15.15% regarded it as mostly accessible. When asked for assistance by wheelchair to the user, 44% stated it was moderately helpful, while 31.31% reported it didn’t help them much. Wheelchair accessibility in public spaces was rated as having moderate satisfaction by 49% of users, generally satisfied by 22%, and completely satisfied by 9.09% of users (Table 2).
The reasons behind individuals being unable to afford their wheelchairs illustrate significant barriers that restrict individuals from accessing the wheelchairs. Financial constraints are the main obstacle, as 78% of respondents can’t afford to buy the appropriate wheelchair. 64% of respondents claimed a lack of help, and 41% didn’t know where to purchase a wheelchair. Other difficulties were lack of tools or transportation (9%) and time limits (12%). Moreover, 4% of respondents said the solutions offered were inappropriate, and 5% said that wheelchairs were not available (Figure 3). Satisfaction with wheelchair accessibility.
Many barriers were found for those who have wheelchairs but do not use them. Roads and transportation (63) were the common barriers faced by the users, followed by accessibility at work or school (n = 53), and fit, size, or shape (n = 36). 15 respondents mentioned safety concerns, 7 mentioned weights, and 1 mentioned how the attitudes of others were impacted (Figure 4). Barriers to wheelchair access.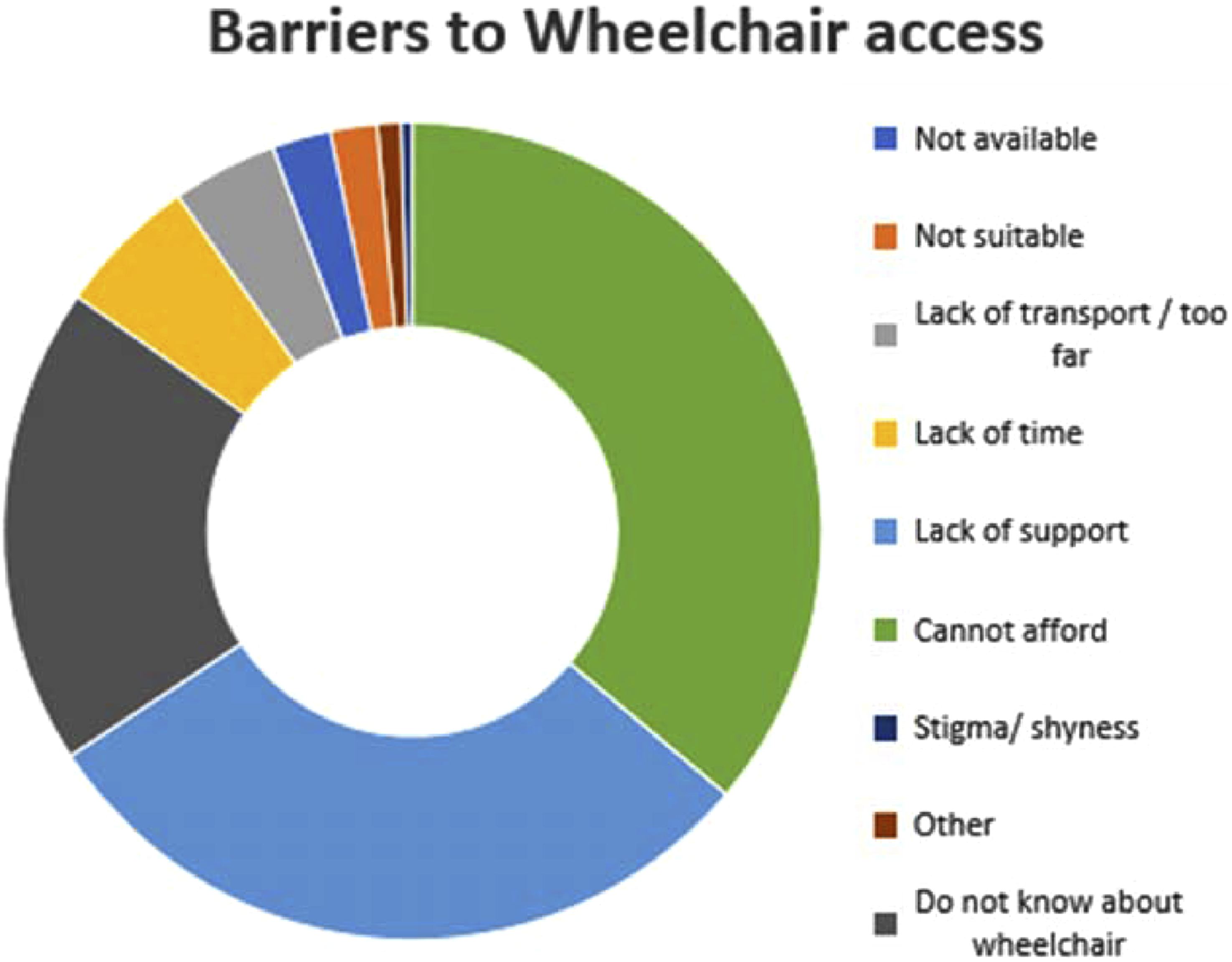
Part two
Interview themes and Sub-Themes.
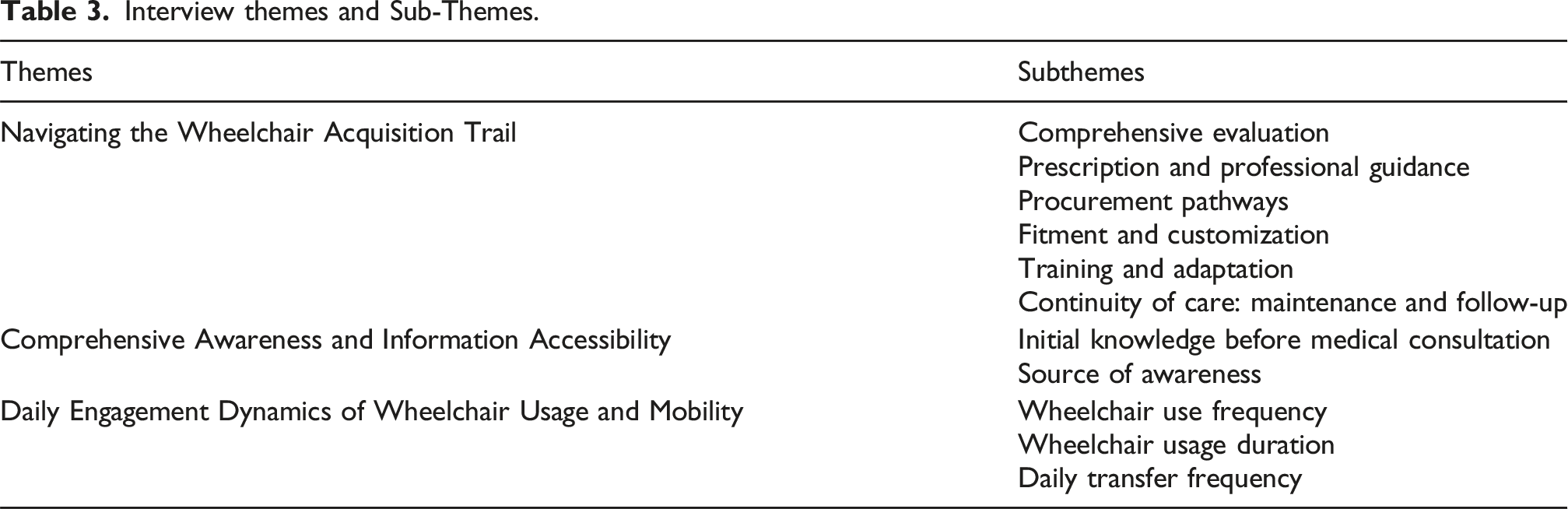
Theme 1 – Navigating wheelchair acquisition trail
Most of the individuals have their wheelchairs for free from NGOs or government programs, but due to limited access to comprehensive wheelchair evaluation and limited finances, it makes it difficult to choose the right wheelchair, which negatively affects the quality of life. Only 5% of the individuals had received a comprehensive evaluation for an appropriate wheelchair. Out of these, 3% were evaluated by a physical therapist, and 2% by social workers. Generally, wheelchairs were available if procured through an NGO. Participants, who had no prior knowledge or personal experience with wheelchairs, described the unknown world of wheelchair use after their injury: “My 26-year-old child diagnosed with cerebral palsy has been using a wheelchair for 22 years. As a single mother, it is difficult for me to take the child for regular follow-up. The wheelchair we obtained was from the NGO and is currently not functioning properly. Due to financial limitations, I hired a wheelchair from Gurudwara for hospital visits.” (P 49).
It was observed that healthcare professionals referred patients to the main wheelchair source. Around 32% of participants consulted their healthcare provider regarding wheelchair purchase, out of which 22% reported that they procured it as advised by the prescriber. In addition to wheelchair measurement, individuals reported being asked about their condition, activities of daily living (ADL), and pressure sore risks. Others reported purchasing their wheelchairs—new or old ones directly from the NGOs or from the market. People who got wheelchairs from NGOs were asked to provide their identifying information—identity cards and photographs for record purposes. “I was diagnosed with AEDM and was advised by psychiatrists to use a wheelchair. The travelling cost was a big challenge, for which I used to borrow money. An NGO visited the Department to donate the wheelchairs. During my evaluation process, I submitted my photo and Aadhaar Card to procure it. In the past, I had difficulties in carrying out daily activities. However, after procuring the wheelchair, my life changed dramatically. In addition to increasing my mobility, my quality of life and active participation in the community also improved.” (P 19)
Occasionally, participants were given wheelchairs as gifts by well-meaning individuals, such as their neighbours or the school. “In the past, I had to carry my child on my lap for OPD visits. Financially, I had no issue procuring the best for my child…..lack of awareness resulted in the development of deformities……….a special school advised us to get a customised wheelchair……..” (S87)
Participants mentioned that limited options for wheelchairs were available in their area, or were not offered many choices. 5% of the participants described going through an active prescription and selection process. 23% received wheelchairs through donations and reported that they felt they had no choice in the matter because the wheelchairs were gratis.
Experienced wheelchair users preferred having more options to choose from and the opportunity to try out different wheelchair models, rather than just relying on recommendations from service providers. They also recommended that new wheelchair users need to receive counselling and training to help them choose the right wheelchair. It was observed that the users who paid for all or part of their wheelchairs were more actively involved in the selection process.
Mobility, independence, and quality of life are enhanced by professional advice, whereas inadequate advice and inaccessibility can lead to the development of secondary complications. 61%, purchased their wheelchairs, being unable to be carried by a caregiver from one department to another, long waits to procure the wheelchair after submission of their identification proof. This interaction between the participants, their wheelchairs, and the world was emphasized: “My 14-year-old child has an amputation of the left lower limb…….borrowed a wheelchair during our visits. However, we had to wait for hours for our turn to use the wheelchair. Sometimes, the patient using the wheelchair took a long time to return…. We missed our appointment slot and we had to make a new appointment, either online or offline. To avoid these challenges during hospital visits, we rented a wheelchair from the Gurudwara.” (S7)
It was observed that participants used their wheelchairs to move out of their homes and meet other people. When a wheelchair was prescribed by doctors or rehabilitation professionals, the major reasons for wheelchair prescription were improving mobility, preventing secondary complications, promoting independence, enhancing the quality of life, reducing the burden on the caregiver, and protecting the caregiver from musculoskeletal damage.
Participants reported that they were prescribed a wheelchair by a healthcare provider, including 20% by non-physiatrist physicians, 17% by physiatrists, and 5% by physiotherapists. These participants were informed about the significance of having a personal wheelchair. “The doctors advised my son to rest for 2 weeks, but it resulted in a decrease in ambulation and generalized muscle weakness. Visiting the hospital for follow-up, we observed others using wheelchairs, so we purchased our wheelchair so that it would be easy for us to carry him to the hospital visits”. (S2)
Participants expressed their reasons for not engaging in physical rehabilitation and the lack of proper guidance for wheelchair use by family members, which ultimately led to the worsening of their condition and the development of secondary complications: “My daughter has been diagnosed with generalized dystonia and kernicterus, which has resulted in involuntary body movements and loss of control…………due to my breast cancer, I am unable to help my daughter with her daily exercises………….condition has worsened compared to what it was earlier.” (S8)
The wheelchair acquisition resulted in financial and functional challenges for many participants in obtaining their wheelchairs. Participants who received their customized wheelchairs (5%) found them to be more beneficial than standard models. Wheelchairs that failed to fit correctly resulted in severe discomfort and health problems, highlighting the importance of customization. The prescription-based customized wheelchair providers are not easily available and often patients with limited education and digital awareness are unable to get the customizations done. No such facility is available in Governmental setups, and very few private service providers, NGOs, and hospitals have this facility. “I visited the private hospital ….assessment and counselling for wheelchair done…..with an increase in body weight and height, the current wheelchair is not at all comfortable for her to sit in. She has severe pain in both legs and back once she is out of bed. Being a single mother, I am unable to afford the new wheelchair for my daughter”. (S41)
Lack of proper wheelchair usage, daily living challenges, and difficulties with public transportation highlight the importance of comprehensive training and assistance for new users and their families. Generally, research participants did not receive much instruction on how to maneuver their wheelchairs, except those who underwent long-term rehabilitation in the hospital or received other institutional treatment.
Wheelchair users find it difficult to operate it with ease due to frequent maintenance and repair issues, added expenses, and poor-quality materials, emphasizing the urgent need for more dependable and reasonably priced solutions. Some also had trouble obtaining replacement components. Users expressed dissatisfaction with the brakes and tires, which require frequent repair. Most of the donated wheelchairs had fixed armrests, which were also very high and made the transfers challenging. “……..avoiding using the wheelchair during the rainy season and monthly cleaning and oiling to keep it in good condition………but now it has rusted and requires replacement…… had fallen 2-3 times while transferring from the heelchair to the bed or vice versa due to poor brakes and bad seat quality…currently, not safe for me to use for long”. (S19)
Theme 2: Comprehensive awareness and accessibility
When selecting a wheelchair, evaluation and modification are essential, which they learn by personal experience and observation. Many participants discussed the crucial role of personalized, well-informed decision-making in the selection and use of wheelchairs. “….. For me, assessment, selection, and wheelchair customization are important factors before purchasing a wheelchair”. (S3)
Theme 3: Usage
Wheelchair users utilize it daily, yet they have limited independence and movement due to improper wheelchair conditions, a lack of accessible places to visit, and difficult transportation. According to the survey, 8.08% of the participants used a wheelchair a few times a month, 15.15% used a wheelchair a few times a week, and 71.72% used it daily. 53% of the participants used their wheelchairs for outdoor mobility, while 42% used them for both indoor and outdoor access. None of the participants reported using the wheelchair only for indoor mobility due to the small space at home. “I use my wheelchair daily, but its poor condition limits my activities and requires me to adapt.” (S10)
Participants expressed dissatisfaction with the lack of wheelchair-friendly public places and difficulties in transportation, especially if their homes were not on the ground floor. Concerns about uneven roads, obstacles, and traffic were also highlighted. Participants expressed fear of accessing their wheelchairs independently and sometimes relied on family members or caregivers for help. “……..adapting to the environment is most challenging for me…… face a lot of challenges in my daily living using this wheelchair……..fatigued from pushing my wheelchair for a long duration, and my skin cuts with increased use. Due to strong heat waves, in summer, the wheel rim gets extremely hot, making it difficult for me to propel the wheelchair. Even I face a lot of problems using public transport…… bus does not stop at the particular point where wheelchair services could be provided to the user, most of them don’t have ramps for wheelchair accessibility, or if they have, then it is not in good working condition. Even most of the cab drivers do not take rides as they would have to transport the wheelchair inside the cab, or their seat cover may get damaged keeping the wheelchair inside their cab. (S19)
Wheelchairs are challenging to use because of accessibility issues, emphasizing the need for better infrastructure and mobility aids. Regarding the duration, they used their wheelchairs every single day; 78% of individuals reported using them for more than 120 min. Wheelchairs play an essential role in their everyday routines, and their frequent use highlights the urgent need for accessible environments. A smaller percentage utilizes their wheelchairs for less than 30 min, accounting for 5% of users, and spends between 60 and 120 min (11%) and 30-60 min (7%) using them. Such differences imply that individuals’ levels of mobility and dependence on other devices differed.
The variation in number of transfers in and out of wheelchairs: 69% of participants reported fewer than five transfers per day, indicating prolonged stays in their wheelchairs; roughly 28% reported five to 10 transfers, indicating more active mobility or the need to switch between different aids; and 3% reported 10 or more transfers, indicating very high activity or frequent switching between mobility aids.
Discussion
The findings of this study offer insights into wheelchair awareness, usage, unmet needs, and barriers faced by wheelchair users in India. The mixed-methods approach provided valuable information on improving wheelchair provisions and services. Participants expressed varying levels of satisfaction with the services they received. The most common age for injury occurrence is between 16 and 30 years old.23,24 This study also supports this, as 39% of the total study sample was between the ages of 25 and 50 years old. Integration of quantitative and qualitative findings revealed that while quantitative data captured the magnitude of unmet wheelchair needs, qualitative narratives explained the underlying factors, such as affordability and lack of tailored services. Together, they provided a comprehensive understanding of the user experience.
Females in India face many challenges due to their gender and disability, as their demands are unmet. For example, they have lower accessibility to assistive devices compared to males. Females face significant challenges due to gender inequality. Patriarchal societal norms prioritize males, resulting in lower accessibility to essential assistive devices and healthcare for females. Cultural stigma and discrimination lead to social exclusion and neglect.1,25,26
Our study reported that 28.29% of the participants use the Indian toilet even if they have a disability. Overall availability of washroom facilities within the housing area is limited, and if available, they are inaccessible. The reason was no access to western toilets or modifications in their areas. A survey-based study by Agarwal A., and Jain Y (2018) 27 reported that the use of seated toilets is as high as 20%–50% in some parts of urban India, but in rural India, the use of seated toilets is 5% which points towards its increased cultural acceptance in urban areas.
Manual wheelchairs (91%) were mostly procured due to affordability, durability, and easy access. Government and NGO initiatives prefer providing manual wheelchairs, which are not customized wheelchairs, as even getting the removable armrest significantly increases the price. Customisation adds cost to the donor and reduces the number of beneficiaries of the donors. 16 Subsidizing customization in wheelchairs, providing insurance schemes, expanding their availability in rural areas, providing maintenance services, and integrating wheelchair provision in hospital and healthcare systems are also important aspects of wheeled mobility provision. The study revealed that participants with good upper limb strength were able to propel their wheelchair independently, while those with less than grade 3 muscle power were not able to propel it by themselves and required assistance from the caregiver or the attendant.
Most of the participants with long-term disabilities, such as Spinal Cord Injuries (40%) and Cerebral Palsy (12%), highlight an increased need for long-term and effective solutions for mobility. By 2028, the Indian wheelchair market is expected to expand at a Compound Annual Growth Rate (CAGR) of 9.5% 28 primarily because of an increase in Spinal Injuries, the geriatric population, and increased awareness of improved wheelchair technologies and comfort. 28
Thus, the results of this study highlight the importance of wheelchair solutions to improve mobility and the level of independence for wheelchair users. Studies such as those by WHO, 29 and GReAT 30 revealed that without appropriate wheelchairs, PWDs are at a greater risk of social exclusion and reduced quality of life. The small proportion of people with no difficulty at all with wheelchairs emphasizes the need for increasing accessibility and availability of wheelchair services to fully address these issues. 30
The present study suggested a high demand for wheelchairs related needs. The source for wheelchair procurement mainly from friends or family, the private sector, and public facilities, indicates the dependence on NGO and private sources. Most of the time, it is the hospital where the patient goes to get the care and opinion of the doctor. A streamlined approach to prescription, procurement, and follow-up is lacking in health systems. Participants procured their wheelchairs from their families, neighbours, scrap dealers, and gurudwara; therefore, policy interventions should enhance public provision and financial support for wheelchair provision. 31
A study by Gupta S et al. (2021) stated that two-thirds of the users purchased the device themselves, while only one-fifth acquired their mobility aids through government programs 16 which supports our study findings.
Many studies support wheelchair cost as the main obstacle when procuring. Many people can’t afford the expense of basic wheelchairs, especially in low- and middle-income nations. One way to lower the cost of wheelchair provision is to encourage recycling and refurbishment as sustainable practices. Assessing the additional expenses and advantages of substitute delivery strategies will assist policymakers in optimizing health outcomes for wheelchair users.8,32
Modifications are necessary for individual needs, as most of the study participants came from lower socioeconomic backgrounds. The study findings were consistent with those of White et al. (1995), who found that the major concern for people with disability was the lack of affordable and wheelchair- accessible housing.33,34 Furthermore, the demand for appropriate wheelchairs and the lack of good supply from manufacturers were felt. The gap is in the integration of affordable prices and service delivery. Most patients were offered wheelchairs from charitable organizations and Government schemes leading to dissatisfaction and wastage of resources.
The present study has limitations such as a small sample size and potential recall bias due to self-reporting and may have exaggerated or underreported their experiences due to cultural or desirability bias. The study’s urban setting and mainly focused on the tertiary health care service area may not accurately represent challenges faced by wheelchair users in rural areas, though most of the participants come from rural and semi-rural areas in the hospital as it is a tertiary care referral hospital. As the study used convenience sampling, findings may not represent all wheelchair users across diverse communities or rural settings. Also, it was evident that further studies should focus on gender- specific policies for specialized assistive technology needs, the availability and effectiveness of customized wheelchairs, and the long-term impacts on the health and mobility of female wheelchair users.
The rATA has several limitations in the context of wheelchair assessment and usability. The scale doesn’t consider cultural differences in behaviour and communication. It could be filled by the user’s caregiver, leading to reduced involvement of the user in the decision-making process, resulting in a mismatch between the user’s preferences and the recommended wheelchair. The scale is time-consuming, which hampers the accuracy and appropriateness of the recorded response. It doesn’t measure the user’s needs as they change over time. Further studies supplemented with focused scales on assistive technology evaluation and assessment may be needed for detailed evaluation of user satisfaction, compliance, and outcomes.
Conclusion
The study provided insights into wheelchair provisions and user satisfaction, highlighting provision, prescription, and participation barriers and the gender disparities in access. Wheelchair users face challenges due to a lack of awareness and infrastructure. The assistive technology provision and follow-up services need to be integrated into the health systems as a starting point for the inclusion of comprehensive rehabilitation provision for persons with temporary or permanent impairments as a consequence of disease or disorder in a healthcare setting. The mixed-method approach provided preliminary information which may lead to improving wheelchair provisions and services in India. The need for educational programs, policy changes, and improved facilities for assistive technology is well understood and highlighted by the WHO in its vision document “Rehabilitation 2030,” and hence, policies and frameworks need to be put in place for the same.
Footnotes
Acknowledgments
The authors thank the individuals for their participation in the study. Dr. Sandeep Singh (PI -NCHAT), and all the team members of the National Centre for Assistive Health Technology (NCAHT), Indian Council of Medical Research (ICMR), New Delhi, All India Institute of Medical Sciences, New Delhi, and all the Residents at AIIMS-PMR Department are acknowledged for their guidance and assistance in data collection. Dr. Brijesh Kumar (PhD), Ms. Priyanka Morbale and Mrs. Prarthana Sanya Lall (PT) are acknowledged for their support with data analysis and management.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Indian Council of Medical Research, New Delhi, India.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this research is available to be shared if required