
Abstract
Introduction
Manual wheelchair users (MWU) frequently experience upper limb (UL) injury and pain. Clinical practice guidelines (CPG) provide guidance on how to reduce risk of UL injury and pain but the recommendations provide only general advice such as to minimizing repetitive strain by reducing rolling resistance (RR). RR is due to energy loss between wheels and ground during wheelchair propulsion and is a major contributor of repetitive strain for MWUs. Motivated by the recommendation to reduce RR, we developed a clinical decision support system (CDSS) to provide client-specific RR predictions across several wheelchair setups to allow clinicians and users to make informed decisions.
Methods
An iterative user-centered design process (mixed methods) recruited ATP certified occupational or physical therapists to suggest modifications, assess usability and usefulness, identify client use cases, and provide rear wheel and caster selection criteria.
Results
Six clinicians participated and suggested over 100 modifications. Usability (SUS = 83.8; modified QUIS = 7.5) and perceived usefulness (TAQ = 4.7) were acceptable. Client use cases and rear wheel and caster selection criteria were identified. All clinicians thought it would be a useful tool.
Conclusions
RightWheel online CDSS provides user-customized RR estimates for equipment options in an easy-to-understand format, and was deemed ready for pilot launch.
Keywords
Introduction
Upper limb (UL) injury and pain are frequently experienced by manual wheelchair users (MWU).1,2 Clinical practice guidelines (CPG) for preservation of UL function were developed to provide guidance to clinicians on how to reduce risk of UL injury and pain for MWU. The CPG’s 3 recommend minimizing repetitive strain, but only general guidelines are available, such as minimizing rolling resistance (RR) by using pneumatic versus airless insert tires, positioning the axle as far forward as possible to distribute more weight on the rear wheels, and optimizing propulsion biomechanics through proper hand position relative to the axle and appropriate elbow angle relative to the push rim.
Importantly, RR is the primary source of repetitive strain for MWU, and is caused by energy dissipation when the wheels roll on the ground. 4 RR varies depending on factors such as the wheel type and size, load, and the surface propelled upon. 5 RR is often tested at a system-level, which makes it difficult to understand how the RR for each rear wheel or caster varies according to changes in factors like loading, ground surface, and tire pressure. With a system-level test, the weight on the rear wheels and caster can be measured, but separating their contribution to RR is more difficult. A component-level RR test was developed5,6 and validated, 7 which provides RR forces for individual wheels and factors. From this, individualized system-level RR predictions for a specific user weight can be estimated. These estimates, in turn, can be generated for several prospective wheelchair setups and thereby be used to help MWUs and clinicians select the equipment setup that can reduce RR and thereby UL risk while meeting other criterion. These prospective estimates could serve as a valuable clinical decision support system (CDSS) that could help optimize the wheelchair prescription process.
Precision and accuracy of component-level RR was assessed and validated in two studies, comparing with treadmill RR system-level tests 7 and with SmartWheel system-level RR tests. Both studies demonstrated the precision and accuracy of component-level RR compared with system-level RR tests. Component-level RR predictions are somewhat lower than system-level tests, 7 with −1.1 N offset observed versus treadmill, and excellent reliability based on intraclass correlation coefficient (ICC) of 0.94 with 95% confidence interval [0.91–0.95]. 7 Component level RR has also been used to quantify the effects of corrosion, shock and abrasion for casters. 8
Compared to system-level tests, component-level tests cannot assess differences in user propulsion technique and the effect of speed on component-level RR force is minimal (comparing 0.5 and 1.0 m/s), whereas system-level tests do report differences related to speed. 9 Surfaces must be able to be applied to the drum.
Decision support system benefits
CDSS provide patient specific recommendations via computer-based systems and are often integrated into the electronic medical record. 10 CDSS provide many benefits, including (1) clinical management to support adherence to CPG,10,11 (2) diagnostic support by providing suggestions for clinicians, 12 (3) communication and education with patients, 13 (4) improved workflow, 14 and (5) alerts for follow up appointments. 15 Clinicians value CDSS when they are easy to use and implement into clinical care, especially if they save time during the clinical encounter and patients are more satisfied with care after using CDSS. 16 CDSS also adds value by increasing patient and clinician knowledge, engaging patients in sharing preferences and in decision making and reducing decisional conflict. 16 Barriers and facilitators research suggest that the CDSS should support clinician assessment and decision making, not replace it, because there are many comorbidities and other considerations that the tool cannot incorporate. 17 Currently, pressure mapping is the only CDSS used by clinicians for wheelchair provision, which provides visual feedback on high pressure points and pressure distribution to assist with cushion selection to prevent pressure injuries.
RightWheel concept and considerations
We conceptualized a CDSS that would incorporate component-level RR data in a user-friendly format, developed with clinicians’ input on necessary revisions, usability, and perceived usefulness. The objective was to incorporate as many of the important benefits of CDSS as possible in RightWheel, and usability and perceived usefulness were identified as important outcome measures because how ‘easy to use and implement in clinic care’ are criteria which will determine if the CDSS will or will not be used by clinicians. To accomplish this, an iterative user-centered design process was planned, which incorporates human factors and usability methodologies and considerations into the design process. 18 User-centered design is often used for development of computer-user interfaces to improve the user experience, 18 and is a widely accepted approach to product design.
Our goals were to develop the prototype RightWheel CDSS, and then iterate the RightWheel design features until the tool had acceptable usability and perceived usefulness, and adds value to the work of clinicians/wheelchair providers based on if it would be a useful tool and their intention to use RightWheel. The hypothesis is that RightWheel has acceptable usability based on system usability scale (SUS)
While iterating the RightWheel design, we will identify use cases where RightWheel can provide value to clients and understand and outline the rear wheel and caster selection criteria.
Methods
A three stage (0→2) development process (mixed methods) was used to develop RightWheel. The objectives and software platform for each stage are summarized in Figure 1. The development steps are summarized in Table 1. Development objectives and software by stage. Development steps by stage.

The Stage 0 objective is to develop a proof-of-concept RR calculator, and completion criteria is a working prototype. The Stage 1 objective is to develop an online CDSS integrating a graphical user interface and completion criteria is a working online prototype which can be demonstrated to stakeholders.
The Stage 2 objectives are to develop an expanded online CDSS that is intuitive, easy-to-use and provides actionable information for clinicians, using an iterative development process and recruiting clinicians to provide feedback on ‘must-have’ and ‘nice-to-have’ changes and preferred images. The think-aloud method 19 was used during clinician interviews because it has been shown to assist in the development of a usable CDSS. 20
The completion criteria for Stage 2 are (1) all feasible ‘must-have’ and ’nice-to-have’ changes are implemented, (2) RightWheel has acceptable usability and perceived usefulness, (3) a list of clients who would benefit from RightWheel are identified (use cases), (4) decision criteria for rear wheel and caster selection are summarized, and (5) RightWheel is deemed ready for a pilot launch study.
Participant recruitment (stage 2)
Institutional Review Board review determined that the focus groups/interviews for this study (STUDY20060124) met regulatory requirements for exempt research. The inclusion criteria for participants are occupational therapists, physical therapists, or assistive technology engineers who evaluate at least ten manual wheelchair clients per year in a seating clinic, with an ATP certification. There were no exclusion criteria. Recruitment was planned until redundant feedback is obtained or ten clinicians have been interviewed. Clinicians were recruited from individuals who had expressed interest in participating in development of the tool during a RR state of the science webinar, and clinicians who are known to the research team.
Outcome measures (stage 2)
Two standard usability surveys (SUS
21
and modified QUIS
22
) were selected as outcome measures because they are often used in development of technology, are validated, reliable, and have an established threshold for acceptability. SUS assesses usability using ten general questions scored on a scale of 1 to 5 and converted to a 100 point scale, with overall average reported. QUIS evaluates satisfaction of the user-computer interface, with twenty seven questions grouped into five categories (overall reaction, screen, technology and system information, learning, and system capabilities), is scored on scale of 0 to 9, and reports the average score. The modified QUIS included eighteen questions, and removed questions which were not relevant to RightWheel. Both surveys have been widely used and have pre-determined scores representing ‘acceptable’ threshold. A technology acceptance questionnaire (TAQ) was developed to measure perceived usefulness, and incorporates the identified CDSS benefits aligned within the technology acceptance model (TAM) framework. TAM was developed to increase use of information technology and promote technology acceptance, and is based on the theory of reasoned action, a social-psychological behavior theory
23
that intention to accept technology is determined by attitude, perceived usefulness, and perceived ease of use (Figure 2).23,24 TAM has proven validity and reliability, has been used widely and increasingly is used to assess healthcare and mobile health.23–25 Variations to the TAM framework have also been used to assess technology acceptance.23,24 The rationale for criteria of TAQ ≥ 4 is that an average response of “agree” (i.e., 4) on a scale of 1 (strongly disagree) to 5 (strongly agree) indicates an acceptable threshold of perceived usefulness, leading to behavioral intention to use RightWheel. Technology acceptance model.
Interviews and surveys (stage 2)
Participant interview sequence for RightWheel development.

Rear wheels and casters selection criteria questionnaire.

Image preferences for percent difference and equivalent weight were assessed by displaying four options for each image type in RightWheel (via use of drop-down menus) and asking the clinician their preference. To determine the most promising use cases, clinicians were asked the profile of users who would and would not benefit from the tool. All feasible recommended design changes were made to RightWheel, and as needed, clinicians were asked to review and confirm that their recommendations were appropriately implemented into the revised prototype during a short (∼15 min) follow-up online meeting. All feasible recommended design changes were incorporated prior to the next clinician interview.
At the end of stage 2, multiple images had been refined or newly generated based on clinician suggestions, and resultant force had been added to the results. To obtain input from all clinicians on these image options, an online preferences survey was developed which included questions about image preferences, awareness of resultant force, and value of resultant force estimates.
A rear wheel and caster database with equipment which is meaningful to clinicians was developed, based on equipment previously evaluated in our lab,5,7 frequency of equipment observed in prior field study, 26 and clinician interview feedback. The nine rear wheel tires included high pressure pneumatic, low pressure pneumatic, knobby pneumatic, solid polyurethane, and airless insert, with 24” diameter (7) or 25” diameter (2). All were mounted on standard spoked wheels with one exception (solid polyurethane on mag wheel). The fourteen casters include soft roll casters (3, 4, 5, 6 inch diameter × 1.5” width), polyurethane (4, 5, 6, 8 inch diameter × 0.75 to 1.0” width) rollerblade (3” diameter × 1” width), pneumatic (6 or 8” diameter × 1.25” to 2” width), and semi-pneumatic (8” diameter × 1.75” width). Two surfaces representative of typical commercial and home environments were selected, linoleum (Forbo) and low pile carpet with ¼” felt padding.
Data and statistical analysis
All surveys were conducted online using Qualtrics. Meetings were recorded and transcribed, with clinicians de-identified using a participant number, and the recording deleted approximately 1 month after the interview. Both the researcher and illustrator participated in all interviews. Responses to rear wheel and caster selection criteria were tabulated and analyzed by question to extract common themes. Clinician quotes were selected that highlight important challenges and common viewpoints. Think-aloud 19 ‘must-have’ and ‘nice-to-have’ suggested changes were categorized in four areas: layout, content, look/style, and images, by participant, with suggestions compiled in a spreadsheet by participant and category, and completion of changes tracked. A summary of the recommended changes implemented are reported, and suggested changes not implemented are summarized with rationale. Clinician image preferences (Likert-scale ratings) were tabulated. Use cases were summarized into a list of clients who would benefit from RightWheel, and type of clients who are not appropriate.
Clinician demographic characteristics are tabulated and reported. Usability and perceived usefulness participant scores mean and standard deviation (SD) are reported, with acceptable thresholds of SUS ≥ 68, modified QUIS ≥ 6 and TAQ ≥ 4.21,22
Results
Stage 0: define design criteria
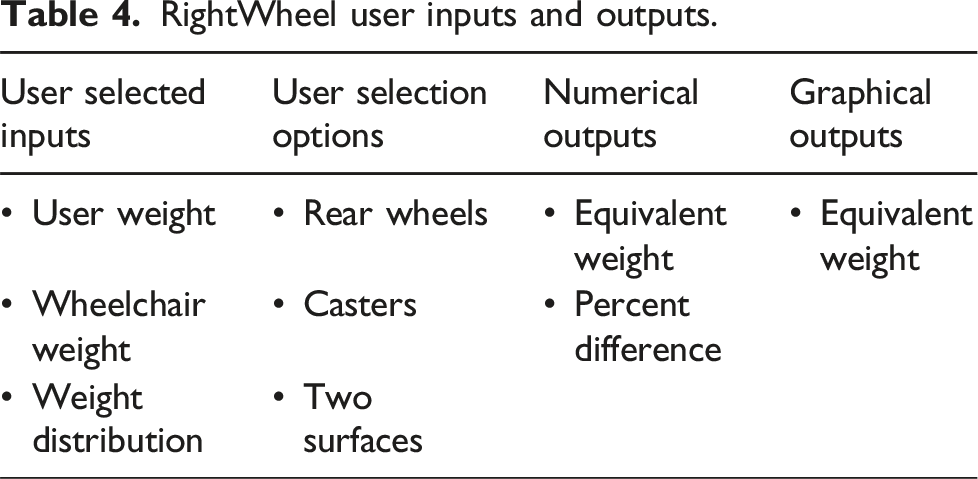
RightWheel user inputs and outputs.
Stage 0: Define algorithms and equations
The calculations are broken into multiple steps: rear wheel and caster loads, RR force, percent difference, and additional equivalent weight. RR force calculations use the slope and intercept from linear regression of load versus RR force test data and calculates the RR force for the specific rear wheel and caster loads to calculate system-level RR. Equivalent weight is calculated using RR slope and intercept to estimate the additional weight needed on the reference rear wheel and caster to equal the RR of the compared equipment. 27 The output displays the increase or decrease in RR, equivalent weight and percent differences, depending on the equipment compared.
Stage 0: Develop prototype and verify accuracy
The stage 0 prototype selected the appropriate slope and intercept data for each wheel/surface combination using ‘IF (AND’ logic. ‘IF’ logic was also used to select equivalent weight images. The stage 0 prototype was functional but not aesthetically pleasing or user friendly (Figure 3). Accuracy of excel output were compared with hand calculations for multiple rear wheels and casters at various weights to ensure that there are no calculation errors. The outcome of Stage 0 was a working prototype that could be used to complete calculations and demonstrate functionality with stakeholders. Stage 0 RightWheel prototype.
Stage 1: Define design criteria
Overview of design criteria by development stage.

Stage 1: Develop prototype and verify accuracy
The online CDSS was developed for an existing WordPress website, utilizing add-on software, with the final prototype shown in Figure 4. Accuracy of calculations was verified by comparing results with the stage 0 prototype. The add-on software had three challenges. First, the add-on software had limitations that made programming and troubleshooting difficult and was quickly identified as a significant weakness by the investigators; second, the software had limited options for user interface look and layout; and third, there were monthly software use fees. Stage 1 RightWheel prototype.
Stage 1: Gather feedback
The prototype was demonstrated at a state-of-the-science online webinar in November 2021, and a poll with 49 participants (comprised of 53% clinicians, 12% suppliers, 12% manufacturers), found 82% agreeing RightWheel would be useful in their context. Of these participants, 15 responded with interest in assisting in our development of this tool.
Stage 2: Define design criteria
The Stage 2 design criteria builds on the Stage 1 prototype, with additional design criteria outlined in Table 5. R Studio Shiny app was selected because it provides an aesthetically pleasing graphical user interface and the open-source software has free and low-cost monthly online hosting options at shinyapps.io. Shiny has extensive user tutorials, guides, and examples of working program code, making the development process easier.
Stage 2: Develop prototype and verify accuracy
The initial stage 2 prototype placed all the content on a single page. Accuracy was verified by comparing results with the stage 0 prototype. The illustrator created four concept image options for equivalent weight, consisting of a wheelchair user with either a backpack, trailer, on a ramp, or with wind blowing, to visualize the difference in force required to propel (Figure 5). The person in the wheelchair was a neutral character, not the focus of the image. Four different concept images representing percent difference were also created, based on a speedometer concept, with cool to hot colors indicating lower or higher differences (Figure 6). Initially only three percent difference gauge versions (representing minimum, zero, and maximum) and three to five equivalent weight versions (representing low to high) for each image type were developed. Initial equivalent weight image options. Percent difference image options.

Stage 2: Gather feedback
Recruit clinicians
Clinician characteristics.


Clinician Rear Wheel and Caster Preferences *Other considerations for selecting tires and rims: goals for use, client factors such as grip strength, funding **What makes rear wheels and/or casters preferred? Reduced RR (2), lighter weight, better shock absorption, terrain management, durability, rigor.
Suggested changes
Number of suggestions by category and participant.

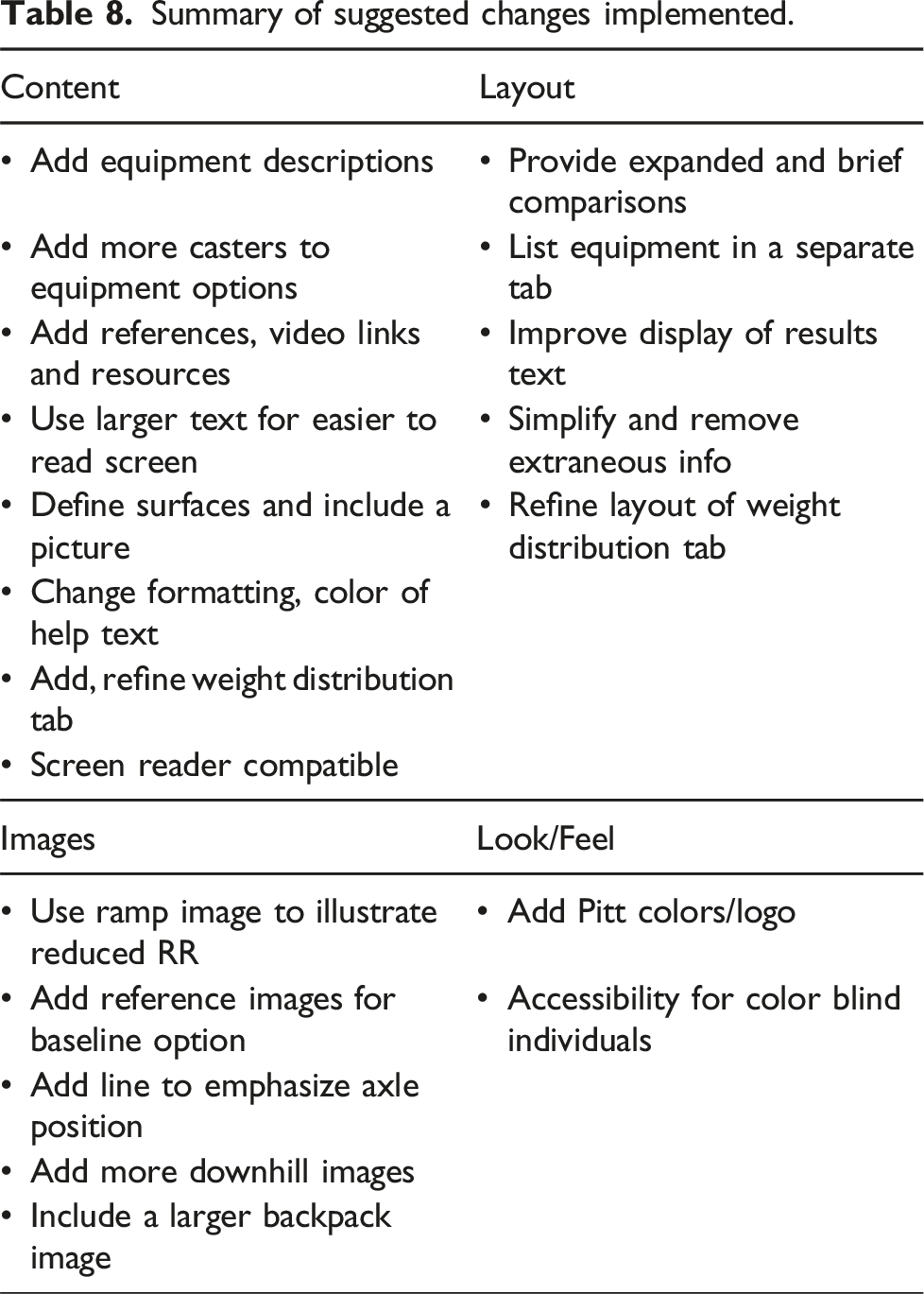
Summary of suggested changes implemented.

Stage 2 final RightWheel prototype - brief comparison tab.
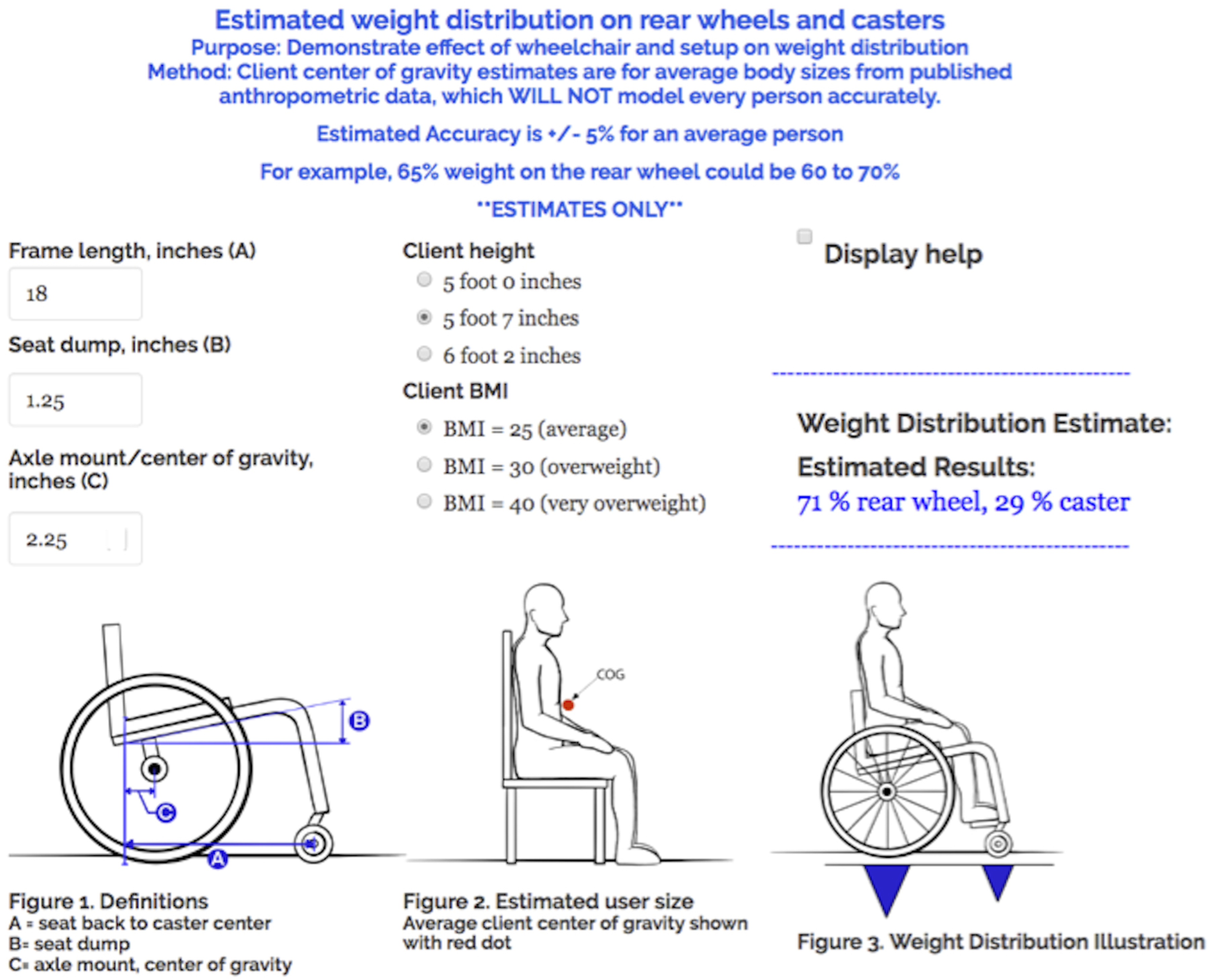
Stage 2 final RightWheel prototype - estimated weight distribution tab.
Two accessibility considerations are incorporated: (1) legibility and visibility, including for colorblind individuals, and (2) screen reader compatibility. For optimal legibility and visibility, a white background with black text and larger font size are incorporated throughout. 28 A limited amount of blue text is used for contrast. Results are conveyed with text and images, and the images have cues which are understandable even if colors cannot be discerned, for example, the red needle indicating percent difference and resultant force has a black outline, and equivalent weight images do not require color to understand the information conveyed. RightWheel is screen reader compatible, and was evaluated using standard accessibility Voice Over Mac software, which demonstrated the ability to read text, drop down menu options, results text, and alt text for results images.
Suggested changes not implemented.

Image preferences
The clinician preferences for equivalent weight (Figure 5) and percent difference (Figure 6) are summarized in Figure 10. For equivalent weight, there was no single preferred image. The backpack and trailer were preferred by most clinicians, and wind and ramp preferred by some. Based on the lack of a single preferred option for equivalent weight, that each image resonated with different clinicians, and because all images could be retained using an image selection button, all four equivalent weight image options were included in the final version. For images representing percent difference, the full gauge version 1 was preferred by all clinicians and was selected for use in RightWheel. At the end of the study, the full range of selected images were developed (minimum to maximum for gauges, low to high for equivalent weight). Image preferences (interview).
The clinician preferences survey image options are shown in Figures 11 and 12, with results in Figure 13 and Table 10. There was a strong preference for the red trailer and backpack images (equivalent weight), angled slider (resultant force), and triangle (weight distribution), all of which were incorporated in final version and displayed in Figures 6 and 7. For images conveying reduced RR, there was no clear preference, so the image with no backpack or trailer was retained. Clinicians valued resultant force and supported including that information in RightWheel (Table 10). Image options for weight distribution (triangle, square, rectangle) and resultant force (angled or flat slider). Downhill reduced rolling resistance image options. Image preferences (survey). Value of resultant force (RF) information.



Usability and perceived usefulness
SUS usability and usefulness results by participant.

When asked ‘would this be a useful tool for you’, all the clinicians thought it would be useful, often stating specific types of client use cases where it would be most useful. Clinician quotes include: • “Yeah, it’s just a different method vs the resources that I have that show the differences between the rear tires. This takes into effect a little bit more of the frame configuration along with the casters and how all those play together. It’s pretty cool.” • “To me, it would be a useful tool, because number one, I didn’t know there was so much difference in the different options.” • “I’m rather impressed… This, there’s a lot happening on the screen, but it all makes sense.” • “I love it. I think it’s very useful. I think it’s practical. I think you can use it in letters of justification.”
Client use cases
The clients who would benefit from use of RightWheel include manual wheelchair users who are (1) active, (2) have shoulder concerns or (3) use airless insert or big knobby tires. These may be individuals who are (4) open to optimizing, (5) interested in their care, (6) set in their ways, or (7) newer curious users. Clients that are thought not appropriate for RightWheel include (1) clients who are pushed who have either cognitive limitations or who are frail and elderly; (2) clients who are overwhelmed, including first time wheelchair users. The rationale for not using RightWheel with first time wheelchair users was that it is overwhelming due to the large number of decisions and because every decision and choice is new. Not all clinicians agreed with this, but many did agree that first time wheelchair users are often very overwhelmed.
Rear wheel and caster selection criteria
Rear wheel and caster selection criteria.
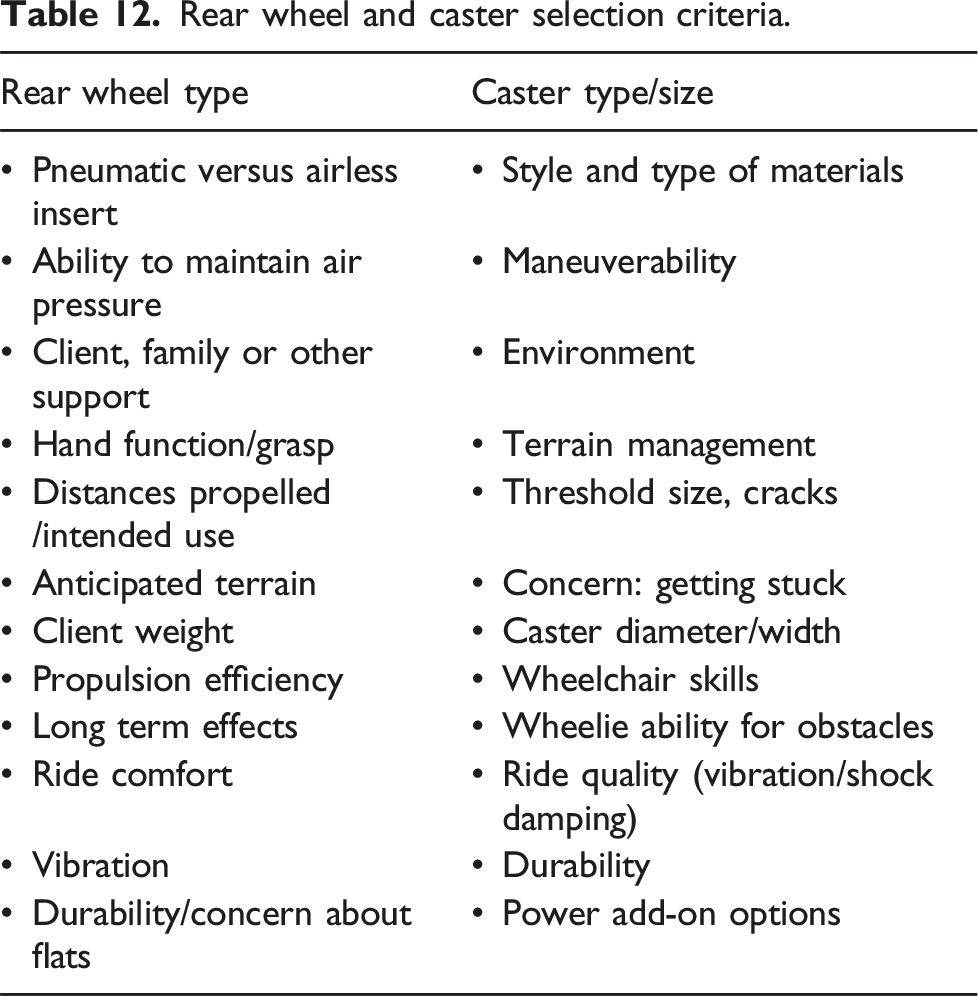
For casters, all prefer soft roll casters, and the primary considerations are terrain (in terms of threshold size and cracks) and concerns about getting stuck, as well as client wheelchair skills and the ability to do wheelies, vibration, durability, and use of power add-on equipment. During this process, clinicians educate clients on options and discuss benefits and challenges related to equipment choices.
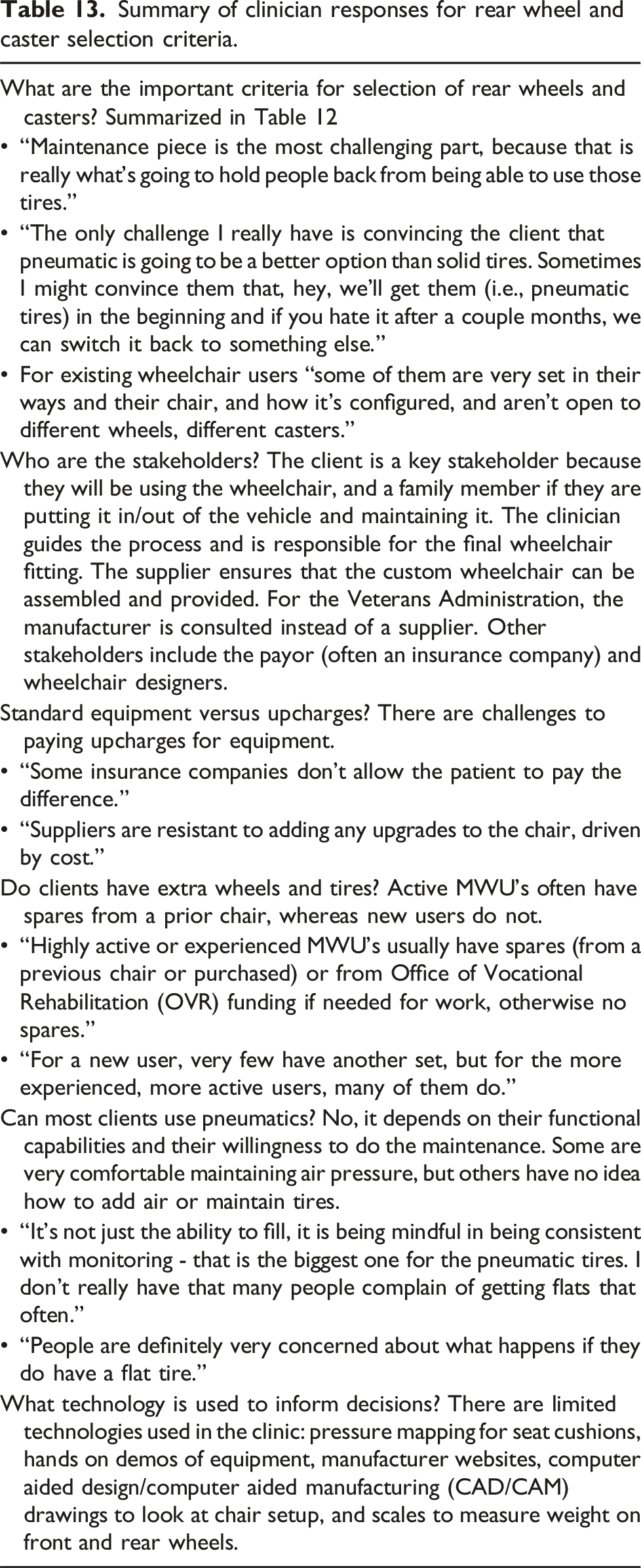
Summary of clinician responses for rear wheel and caster selection criteria.
Discussion
RightWheel development objectives were met. The CDSS was refined through an iterative development process, and the hypothesis that RightWheel would have acceptable usability and perceived usefulness was confirmed, along with clinician intention to use the tool in the future. Clinicians agreed the intended benefits are provided, and thought RightWheel would be a useful tool. The use cases where clients would benefit from its use were identified, and the rear wheel and caster selection criteria were compiled and summarized. RightWheel 29 is deemed ready to proceed to a pilot launch.
The iterative development process used to refine RightWheel incorporated >100 suggested modifications. The clinician’s recommendations were insightful and helped improve RightWheel to meet the objective of being intuitive and easy to use, demonstrating the value of a user-centered design process. Clinician image preferences had common themes for some but not for all images. Clinicians suggested ways to modify and improve images to make them more intuitive and easy-to-understand, changes that the development team would not have identified without their input. Although the iterative development process took time to recruit, interview and integrate feedback before the next interview, RightWheel was significantly improved by following this process. The clinicians who participated in this study were experienced and very aware of the importance of minimizing RR, which could be a source of bias. The lack of anonymity for surveys and interviews could have caused participants to be more positive in their feedback.
Usability and usefulness
Clinician usability scores may reflect perception differences of the questionnaire scale. Participant 4 had lower scores for both surveys, which may reflect more critical grading than other participants. Each clinician evaluated a different revised version of RightWheel, since all prior suggested changes were incorporated before the next clinician assessment. The number of suggestions and type of suggestions varied by clinician, with some providing more suggestions on content, and others more on layout and/or improving images, reflecting each clinician’s own preferences and expertise. The last clinician had fewer suggestions for improvement, indicating a plateau had been reached. Because the TAQ questionnaire was added mid-study, only two clinicians completed it. The two scores reflect agreement in perceived usefulness of RightWheel, (with 4 = agree, 5 = strongly agree), and overall average of 4.7, and responses to ‘I plan to use this tool' (average = 4.5) and ‘I would recommend to other clinicians’ (average = 5).
Use cases
Seven use cases types/descriptions were identified where RightWheel would be useful to the client. The rationale for ‘individuals set in their ways’ is that the visualization could help the client evaluate information differently and potentially make a different decision. There were also examples of cases where the tool would not be useful. For first time wheelchair users, some thought they would be an ideal case, by providing clear information for decision making and avoiding poor equipment selection that may be difficult to change in the future. Others thought there is so much going on, so many decisions, that there is no extra time available during that type of assessment appointment “for new wheelchair users, its overwhelming the number of decisions and choices.” One clinician stated they use two evaluation visits to address the situation of being overwhelmed, because it is so important to ensure they get the appropriate equipment from the beginning.
RightWheel was developed to provide clinicians an improved way to communicate the impact of RR on equipment choices to their clients. Other potential clinician uses of RightWheel includes training clinician-students, educating novice clinicians and ATP’s, and supporting clinicians in daily practice to communicate and educate clients. One clinician suggested they could use screenshots in their letter of medical necessity.
Rear wheel and caster selection criteria
The responses provided insight into how clinicians think through rear wheel and caster selection for their clients. There were a few key considerations (1) can the client maintain the air pressure in the tire; (2) what is the anticipated use, typical distance and terrain, and what equipment would be best for the client; and (3) how do caster and rear wheel size effect the overall wheelchair setup (i.e., floor to seat height, independent transfers and/or foot propelling). Challenges preventing use of pneumatic tires could also be viewed as product development opportunities. Can pneumatic tire air refilling be simplified or automated? Can the requirements for dexterity to attach the pump to the valve be reduced through improved design? Can lower RR tires be developed that do not require air? Is run-flat technology feasible for wheelchair tires? It would be helpful to understand the perceived versus actual risk of a flat tire, and how often flats occur for MWU’s.
Each wheelchair order form identifies standard versus upcharge items, but clinicians had commented “some insurance companies don’t allow the patient to pay the difference” and “suppliers are resistant to adding any upgrades to the chair, driven by cost.” If the optimal rear wheel or caster for the user requires upcharges, this could be a barrier to access. Soft roll casters often require an upcharge, which could limit their use. For example, soft roll casters provide benefits of somewhat lower RR, reduced vibration
30
and the increased width which may help avoid getting stuck for some terrain. For rear wheels, the standard option is often a 1 3/8” wide pneumatic or airless insert tire, with most others requiring an upcharge. Ott et al. measured 200 manual wheelchairs, primarily at adapted sporting events and found 54% high pressure pneumatic tires (
Equipment preferences
Clinician equipment preferences were aligned with low RR rear wheels and casters, with most preferring pneumatic tires and all preferring soft roll casters, which corresponds with published RR results. Comparing identical diameters, pneumatic tires have significantly lower RR compared to airless insert tires,5,31 and soft roll casters have somewhat lower RR than polyurethane and provide some vibration reduction. 30
For clinicians who want to explain to clients about RR forces and equipment choices, RightWheel provides a system-level RR estimate for each client and illustrates differences between options. For example, all else being equal, larger diameter wheels have lower RR4,32,33 and RightWheel illustrates this for both rear wheels and casters, for example when comparing 24 and 25” diameter rear wheels with identical tires. Wheel diameter is an important aspect of rear wheel and caster selection, which affects wheelchair setup including seat to floor height, ability for independent transfers and foot propelling.
RightWheel was developed to assist clinicians with appropriate provision by providing user-customized RR and quantifying differences between rear wheel and caster options, and is the first online tool available to clinicians to quantify repetitive strain from RR for individual MWUs.
Conclusion
Using an iterative, user-centered design process, we successfully developed and refined the CDSS RightWheel, and met all development goals, with acceptable usability and perceived usefulness. All clinicians thought that RightWheel would be a useful tool. RightWheel provides user-specific RR in an easy-to-understand format, quantifies differences between equipment options, and is ready for a pilot launch study. There are very few online tools used to assist in the wheelchair provision process, and RightWheel would be a unique tool in the clinic.
Clinicians described the rear wheel and caster selection criteria and challenges. Clinicians preferred pneumatic tires and soft roll casters, both of which provide low RR compared with other options. Some MWU’s who might benefit from pneumatic tires are not able to maintain air pressure either due to physical limitations and/or lack of support. For these clients, if changing the rear wheel to a pneumatic is not possible, modifying the caster can also reduce RR.
Many manual wheelchair users could benefit from use of RightWheel: clients who are active, have shoulder concerns, or use airless inserts or big knobby tires, and are either open to optimizing, interested in their care, set in their ways or newer curious users.
Limitations
A limited number of clinicians were interviewed, and most were highly experienced. Some of the clinicians were known by the researcher and/or our research group. If RightWheel is used for less experienced clinicians or for ATP training, it may require additional assessment of usability for these stakeholders. Other important stakeholders’ (MWUs, suppliers, and manufacturers) preferences and opinions were not surveyed but will be assessed in a future study. The selection of rear wheels and casters tested could be expanded, and an additional surface, such as a simulated outdoor surface, could be included. The weight distribution estimate function (developed at the request of a clinician) utilizes average anthropometric measurements for a limited number of client height and body mass index combinations to estimate client center of gravity, and has limited accuracy when comparing to actual clients. Understanding how this feature would be used by clinicians is needed to determine the necessary changes to improve accuracy.
Future work
A launch study is planned to follow this development phase, and will have clinicians use RightWheel, assess usability and usefulness over time, provide feedback on value and recommended changes, and confirm the type of users (use cases) who most benefit from RightWheel and obtain further feedback on most impactful images representing reduced RR. An evaluation by individuals who are colorblind or use screen readers could provide feedback and suggestions to improve accessibility. Increased RR from simulated long term use could be incorporated in future versions of RightWheel. A prior study measured increased RR for some casters after environmental exposure (corrosion, shock, and abrasion), which highlighted the importance of caster maintenance and appropriate replacement. 8 The effect of wheel type on RR should be evaluated and considered for inclusion in RightWheel.
Supplemental Material
Supplemental Material - Development of RightWheel manual wheelchair wheel rolling resistance clinical decision support system through iterative clinician interviews
Supplemental Material for Development of RightWheel manual wheelchair wheel rolling resistance clinical decision support system through iterative clinician interviews by Holly Wilson-Jene, Rachel Cowan, Zachary Roy and Jon Pearlman in Journal of Rehabilitation and Assistive Technologies Engineering
Footnotes
Acknowledgements
We would like to thank the International Society of Wheelchair Professionals (ISWP) Standards Working Group for their continued support of this research, and Sofia Main for developing the stage 1 online prototype.
Statements and declarations
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Improving Health and Function Through Use of Performance Standards in Wheelchair Selection Grant # 90REGE0001-02-00, U.S. Agency for International Development through Agreement Nos. APC-GM-00068, SPANS-037, APC-GM 0107, and FY19-A01-6024.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
JP, REC and HWJ conceived of the manuscript. HWJ developed and revised CDSS prototypes (stage 0, stage 2). ZR developed and revised custom illustrations for the CDSS. HWJ and ZR conducted the clinician interviews. HWJ wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.